Download presentation
Presentation is loading. Please wait.

2
© 2008 Thomson - Wadsworth Opening Quiz Which of the following contributes most to the weight of the human body? a.Iron b.Water c.Protein d.Calcium Among the following groups, which has the highest percentage of body water? a.Elderly b.Children c.Obese people d.Female adolescents Copyright 2005 Wadsworth Group, a division of Thomson Learning

3
© 2008 Thomson - Wadsworth Opening Quiz What percentage of a person’s total sodium intake derives from naturally occurring food sodium? a.0 b.10 c.50 d.80 Salt-sensitive population groups include all of the following except a.Caucasians. b.African-Americans. c.people with obesity. d.people with diabetes. Copyright 2005 Wadsworth Group, a division of Thomson Learning

4
© 2008 Thomson - Wadsworth Opening Quiz All of the following are known to enhance calcium absorption from the GI tract except a.lactose. b.pregnancy. c.oxalates. d.stomach acid. At what age do adults normally begin to lose bone mass? a.30-40 yrs b.40-50 yrs c.50-60 yrs d.60-70 yrs Copyright 2005 Wadsworth Group, a division of Thomson Learning

5
© 2008 Thomson - Wadsworth Opening Quiz What percentage of people with osteoporosis are female? a.20 b.40 c.60 d.80 All of the following factors are known to enhance the absorption of iron except a.MFP factor. b.stomach acid. c.ascorbic acid. d.calcium from milk. Copyright 2005 Wadsworth Group, a division of Thomson Learning

6
© 2008 Thomson - Wadsworth Opening Quiz In the United States, iron is currently added to which of the following foods? a.Milk and cheese b.Breads and cereals c.Peanut butter and jellies d.Orange juice and tomato juice What is the name given to the ingestion of nonnutritive substances? a.Pica b.Goiter c.Tetany d.Hemosiderosis Copyright 2005 Wadsworth Group, a division of Thomson Learning

7
© 2008 Thomson - Wadsworth Opening Quiz Which of the following is the richest source of iodine? a.Corn b.Seafood c.Orange juice d.Cruciferous vegetables What is the most reliable source of dietary fluoride? a.Public water b.Dark green vegetables c.Milk and milk products d.Meats and whole-grain cereals Copyright 2005 Wadsworth Group, a division of Thomson Learning

8
© 2008 Thomson - Wadsworth Opening Quiz The diseases most common today include all of the following except a.cancer. b.diabetes. c.tuberculosis. d.diseases of the heart and blood vessels. What disease accounts for the majority of deaths of U.S. women? a.Diabetes b.Lung cancer c.Breast cancer d.Coronary heart disease Copyright 2005 Wadsworth Group, a division of Thomson Learning

9
© 2008 Thomson - Wadsworth Opening Quiz What blood cholesterol carrier is of greatest concern in atherosclerosis? a.HDL b.LDL c.HDK d.VLDK Moderate daily alcohol consumption is defined as a.1 drink for both women and men. b.1 drink for women and 2 for men. c.2 drinks for both women and men. d.2 drinks for women and 4 for men. Copyright 2005 Wadsworth Group, a division of Thomson Learning

10
© 2008 Thomson - Wadsworth Opening Quiz Almost every person with type 2 diabetes has a.sarcopenia. b.osteoporosis. c.excess body fat. d.insulin dependency. Which of the following is known to speed up the passage of bile through the large intestines, thereby decreasing exposure time to microorganisms? a.Milk b.Fiber c.Omega-3 fats d.Refined starches Copyright 2005 Wadsworth Group, a division of Thomson Learning

11
© 2008 Thomson - Wadsworth Chapter 12 Water and Major Minerals

12
© 2008 Thomson - Wadsworth Water and the Body Fluids The main role of water is to maintain an appropriate water balance to support vital functions. To maintain water homeostasis, intake from liquids, foods, and metabolism must equal losses from the kidneys, skin, lungs, and feces.

13
© 2008 Thomson - Wadsworth Water and the Body Fluids Water’s roles in the body Carries nutrients and waste products Maintains the structure of large molecules Participates in metabolic reactions Solvent for minerals, vitamins, amino acids, glucose and others Lubricant and cushion around joints, inside the eyes, the spinal cord, and in amniotic fluid during pregnancy Regulation of body temperature Maintains blood volume

14
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Balance and Recommended Intakes Intracellular fluid (inside the cells) makes up about two-thirds of the body’s water. Extracellular fluid (outside the cells) has two components—the interstitial fluid and plasma. Water Intake Thirst is a conscious desire to drink and is regulated by the mouth, hypothalamus, and nerves.
 has two components—the interstitial fluid and plasma. Water Intake Thirst is a conscious desire to drink and is regulated by the mouth, hypothalamus, and nerves..")
15
© 2008 Thomson - Wadsworth

16
Water and the Body Fluids Water Intake Dehydration occurs when water output exceeds input due to an inadequate intake or excessive losses. 1-2% loss of body weight – thirst, fatigue, weakness, vague discomfort, and loss of appetite 3-4% loss of body weight – impaired physical performance, dry mouth, reduction in urine, flushed skin, impatience, and apathy 5-6% loss of body weight – difficulty in concentrating, headache, irritability, sleepiness, impaired temperature regulation, and increased respiratory rate 7-10% loss of body weight – dizziness, spastic muscles, loss of balance, delirium, exhaustion, and collapse

17
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Intake Water intoxication is excessive water contents in all body fluid compartments. It is rare.

18
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Balance and Recommended Intakes Water sources include water, other beverages, fruit, vegetables, meat, cheese, and the byproduct of metabolism. An intake of 1450 to 2800 milliliters of water is usually represented by: Liquids – 550 to 1500 mL Foods – 700 to 1000 mL Metabolic water – 200 to 300 mL

19
© 2008 Thomson - Wadsworth

20
Water and the Body Fluids Water Balance and Recommended Intakes Water losses occur through urine output, water vapor from the lungs, sweating, and feces. An output of 1450 to 2800 milliliters of water is usually represented by: Kidneys – 500 to 1400 mL Skin – 450 to 900 mL Lungs – 350 mL GI tract – 150 mL

21
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Balance and Recommended Intakes Water Recommendations 1.0 to 1.5 mL/kcal expended for adults (approximately 2-3 liters for a 2,000 kcalorie expenditure 1.5 mL/kcal expended for infants and athletes ½ cup per 100 kcal expended Adequate Intake for males is 3.7 L/day. Adequate Intake for females is 2.7 L/day. Both caffeine and alcohol can have a diuretic effect.

22
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Balance and Recommended Intakes Health Effects of Water Meeting fluid needs Protect the bladder, prostrate, and breast against cancer Protect against kidney stones

23
© 2008 Thomson - Wadsworth Water and the Body Fluids Water Balance and Recommended Intakes Kinds of water Hard Water –Water with high calcium and magnesium content –Leaves residues –May benefit hypertension and heart disease Soft water –Water with high sodium and potassium content –May aggravate hypertension and heart disease –Dissolves contaminate minerals in pipes –Practical advantages

24
© 2008 Thomson - Wadsworth Water and the Body Fluids Other types of water: Artesian water – water drawn from a well that taps a confined aquifer in which the water in under pressure Bottled water – drinking water sold in bottles Carbonated water – water that contains carbon dioxide gas, either natural or added Distilled water – free of dissolved minerals Filtered water – water treated by filtration with lead, arsenic, and some microorganisms removed Mineral water – water from a spring or well that contains about 250-500 parts per million of minerals Natural water – water from a spring or well that is certified to be safe and sanitary Public water – water from a city or county water system that has been treated and disinfected Purified water – water that has been treated to remove dissolved solids Spring water – water originating from an underground spring or well Well water – water drawn from ground water by tapping into an aquifer

25
© 2008 Thomson - Wadsworth Water and the Body Fluids Blood Volume and Blood Pressure Fluids are essential to the regulation of blood volume and blood pressure. ADH and Water Retention Antidiuretic hormone (ADH) is released from the pituitary gland and causes kidneys to reabsorb water, thus preventing losses Vasopressin is another name for ADH Renin and Sodium Retention Kidneys release renin to reabsorb sodium Helps to restore blood pressure and blood volume
 is released from the pituitary gland and causes kidneys to reabsorb water, thus preventing losses Vasopressin is another name for ADH Renin and Sodium Retention Kidneys release renin to reabsorb sodium Helps to restore blood pressure and blood volume.")
26
© 2008 Thomson - Wadsworth

27
Water and the Body Fluids Blood Volume and Blood Pressure Angiotensin and Blood Vessel Constriction Angiotensinogen converts to angiotensin A vasoconstrictor that raises blood pressure by narrowing blood vessels Aldosterone and Sodium Retention Angiotensin mediates the release of aldosterone from the adrenal glands Kidneys retain sodium in order to retain water

28
© 2008 Thomson - Wadsworth

29
Water and the Body Fluids Fluid and Electrolyte Balance Several minerals including sodium, chloride, potassium, calcium, phosphorus, magnesium, and sulfur are involved in fluid balance. Dissociation of Salt in Water Dissociates into positive ions called cations and negative ions called anions Ions carry electrical current so they are called electrolytes. Solutions are called electrolyte solutions. Positive and negative charges inside and outside the cell must be balanced. Milliequivalents is the concentration of electrolytes in a volume of solution.

30
© 2008 Thomson - Wadsworth

31
Water and the Body Fluids Fluid and Electrolyte Balance Electrolytes Attract Water Water molecules are neutral, polar Oxygen is negatively charged. Hydrogen is positively charged. Enables body to move fluids

32
© 2008 Thomson - Wadsworth Water and the Body Fluids Fluid and Electrolyte Balance Water Follows Electrolytes Sodium and chloride are primarily outside the cell. Potassium, magnesium, phosphate and sulfur are primarily inside the cell. Osmosis is the movement of water across the cell membrane toward the more concentrated solutes. Osmotic pressure is the amount of pressure needed to prevent the movement of water across a cell membrane.

33
© 2008 Thomson - Wadsworth

35
Fig. 12-6, p. 405 ABABAB With equal numbers of solute particles on both sides of the semipermeable membrane, the concentrations are equal, and the tendency of water to move in either direction is about the same. Now additional solute is added to side B. Solute cannot flow across the divider (in the case of a cell, its membrane). Water can flow both ways across the divider, but has a greater tendency to move from side A to side B, where there is a greater concentration of solute. The volume of water becomes greater on side B, and the concentrations on side A and B become equal. Stepped Art
. Water can flow both ways across the divider, but has a greater tendency to move from side A to side B, where there is a greater concentration of solute. The volume of water becomes greater on side B, and the concentrations on side A and B become equal. Stepped Art.")
36
© 2008 Thomson - Wadsworth Water and the Body Fluids Fluid and Electrolyte Balance Proteins Regulate Flow of Fluids and Ions Proteins attract water and regulate fluid balance. Transport proteins regulate the passage of positive ions. Negative ions follow. Water flows toward the more concentrated solution. The sodium-potassium pump uses ATP to exchange minerals across the cell membrane.

37
© 2008 Thomson - Wadsworth Water and the Body Fluids Fluid and Electrolyte Balance Regulation of Fluid and Electrolyte Balance Digestive juices of GI tract contain minerals and these are reabsorbed as needed Kidneys maintain fluid balance using ADH Kidneys maintain electrolyte balance using aldosterone

38
© 2008 Thomson - Wadsworth Water and the Body Fluids Fluid and Electrolyte Imbalance Medications and medical conditions may interfere with the body’s ability to regulate the fluid and electrolyte balance. Different Solutes Lost by Different Routes Vomiting or diarrhea causes sodium losses. Kidneys may lose too much potassium if there is adrenal hypersecretion of aldosterone. Uncontrolled diabetics may lose glucose and fluid via the kidneys.

39
© 2008 Thomson - Wadsworth Water and the Body Fluids Fluid and Electrolyte Imbalance Replacing Lost Fluids and Electrolytes Drink plain cool water and eat regular foods for temporary small losses. Greater losses require oral rehydration therapy (ORT) –½ L boiling water, 4 tsp sugar and ½ tsp salt –Cool before giving.
 –½ L boiling water, 4 tsp sugar and ½ tsp salt –Cool before giving..")
40
© 2008 Thomson - Wadsworth Water and the Body Fluids Acid-Base Balance The body must maintain an appropriate balance between acids and bases to sustain life. Acidity in measured by the pH value, the concentration of hydrogen atoms. Regulation by the Buffers First line of defense Carbonic acid and bicarbonate can neutralize acids and bases. Carbon dioxide forms carbonic acid in the blood that dissociates to hydrogen ions and bicarbonate ions.

41
© 2008 Thomson - Wadsworth

42
Water and the Body Fluids Acid-Base Balance Regulation in the Lungs Respiration speeds up and slows down as needed to restore homeostasis. Regulation in the Kidneys Selects which ions to retain and which to excrete The urine’s acidity level fluctuates to keep the body’s total acid content balanced.

43
© 2008 Thomson - Wadsworth

44
The Minerals--An Overview Major minerals are found in large quantities in the body, while trace minerals are found in small quantities. Minerals receive special handling in the body. They may bind with other substances and interact with other minerals, thus affecting absorption. Inorganic Elements Major minerals or macrominerals retain their chemical identity when exposed to heat, air, acid, or mixing. Minerals can be lost when they leach into water.

45
© 2008 Thomson - Wadsworth

46
The Minerals--An Overview The Body’s Handling of Minerals Some behave like water-soluble vitamins. Some behave like fat-soluble vitamins. Excessive intake of minerals can be toxic. Variable Bioavailability Binders in food can combine chemically with minerals and prevent their absorption. Phytates are found in legumes and grains. Oxalates are found in spinach and rhubarb.

47
© 2008 Thomson - Wadsworth The Minerals--An Overview Nutrient Interactions Sodium and calcium Phosphorus and magnesium Often caused by supplements Varied Roles Sodium, potassium and chloride function primarily in fluid balance. Calcium, phosphorus and magnesium function primarily in bone growth and health.

48
© 2008 Thomson - Wadsworth Sodium Sodium is one of the primary electrolytes in the body and is responsible for maintaining fluid balance. Dietary recommendations include a moderate intake of salt and sodium. Excesses may aggravate hypertension. Most of the sodium in the diet is found in table salt and processed foods.

49
© 2008 Thomson - Wadsworth Sodium Sodium Roles in the Body Maintains normal fluid and electrolyte and acid-base balance Assists in nerve impulse transmission and muscle contraction Filtered out of the blood by the kidneys

50
© 2008 Thomson - Wadsworth Sodium Sodium Recommendations Minimum Adults: 500 mg/day Adequate Intake (2004) For those 19-50 years of age, 1,500 mg/day For those 51-70 years of age, 1,300 mg/day For those older than 70 years of age, 1,200 mg/day The upper intake level for adults is 2,300 mg/day. Maximum % Daily Value on food labels is set at 2400 mg/day.

51
© 2008 Thomson - Wadsworth Sodium Sodium and Hypertension Salt has a great impact on high blood pressure. Salt restriction does help to lower blood pressure. Salt sensitivity is a term to describe individuals who respond to a high salt intake with high blood pressure. Dietary Approaches to Stop Hypertension (DASH) is a diet plan that helps to lower blood pressure. Sodium and Bone Loss (Osteoporosis) High sodium intake is associated with calcium excretion.
 is a diet plan that helps to lower blood pressure. Sodium and Bone Loss (Osteoporosis) High sodium intake is associated with calcium excretion..")
52
© 2008 Thomson - Wadsworth Sodium Sodium in Foods Large amounts in processed foods (approximately 75% of sodium in the diet) Table salt (approximately 15% added sodium in the diet) Sodium may be present in surprisingly high amounts if chloride is removed. Moderate amounts in meats, milks, breads and vegetables (approximately 10% of sodium in the diet)
.")
53
© 2008 Thomson - Wadsworth

54
Sodium Sodium Deficiency Sodium and water must be replaced after vomiting, diarrhea or heavy sweating. Symptoms are muscle cramps, mental apathy, and loss of appetite. Salt tablets without water induce dehydration. Be careful of hyponatremia during ultra- endurance athletic activities. Sodium Toxicity and Excessive Intakes Edema and acute hypertension Prolonged high intake may contribute to hypertension.

55
© 2008 Thomson - Wadsworth Chloride Chloride in an essential nutrient that plays a role in fluid balance. It is associated with sodium and part of hydrochloric acid in the stomach. Chloride Roles in the Body Maintains normal fluid and electrolyte balance Part of hydrochloric acid found in the stomach Necessary for proper digestion

56
© 2008 Thomson - Wadsworth Chloride Chloride Recommendations and Intakes Recommendations Adequate Intake (2004) –For those 19-50 years of age, 2,300 mg/day –For those 51-70 years of age, 2,000 mg/day –For those older than 70 years of age, 1,800 mg/day Upper intake level is 3,600 mg/day Chloride Intakes Abundant in foods Abundant in processed foods
 –For those years of age, 2,300 mg/day –For those years of age, 2,000 mg/day –For those older than 70 years of age, 1,800 mg/day Upper intake level is 3,600 mg/day Chloride Intakes Abundant in foods Abundant in processed foods")
57
© 2008 Thomson - Wadsworth Chloride Chloride Deficiency and Toxicity Deficiency is rare. Losses can occur with vomiting, diarrhea or heavy sweating. Dehydration due to water deficiency can concentrate chloride to high levels. The toxicity symptom is vomiting.

58
© 2008 Thomson - Wadsworth Potassium Potassium is another electrolyte associated with fluid balance. It is associated with hypertension. It is found in fresh foods—mostly fruits and vegetables.

59
© 2008 Thomson - Wadsworth Potassium Potassium Roles in the Body Maintains normal fluid and electrolyte balance Facilitates many reactions Supports cell integrity Assists in nerve impulse transmission and muscle contractions Maintains the heartbeat

60
© 2008 Thomson - Wadsworth Potassium Potassium Recommendations and Intakes Adequate Intake (2004) For all adults, 4,700 mg/day Fresh foods are rich sources. Processed foods have less potassium.

61
© 2008 Thomson - Wadsworth

62
Potassium Potassium and Hypertension Low potassium intakes increase blood pressure. High potassium intakes prevent and correct hypertension.

63
© 2008 Thomson - Wadsworth Potassium Potassium Deficiency Symptoms include muscular weakness, paralysis, confusion, increased blood pressure, salt sensitivity, kidney stones, and bone turnover. Later signs include irregular heartbeats, muscle weakness, and glucose intolerance.

64
© 2008 Thomson - Wadsworth Potassium Potassium Toxicity Results from supplements or overconsumption of potassium salts Can occur with certain diseases or treatments Symptoms include muscular weakness and vomiting. If given into a vein, potassium can cause the heart to stop.

65
© 2008 Thomson - Wadsworth Calcium Most of calcium (99%) is found in the bones. The remaining calcium (1%) is found in the blood and has many functions. Bone and blood calcium are kept in balance with a system of hormones and vitamin D. Blood calcium remains in balance at the expense of bone calcium and at the risk of developing osteoporosis in later years.
 is found in the blood and has many functions. Bone and blood calcium are kept in balance with a system of hormones and vitamin D. Blood calcium remains in balance at the expense of bone calcium and at the risk of developing osteoporosis in later years..")
66
© 2008 Thomson - Wadsworth Calcium Calcium Roles in the Body Calcium in Bones Hydroxyapatite are crystals of calcium and phosphorus. Mineralization is the process whereby minerals crystallize on the collagen matrix of a growing bone, hardening of the bone. There is an ongoing process of remodeling constantly taking place.

67
© 2008 Thomson - Wadsworth Calcium Calcium Roles in the Body Calcium in Body Fluids Calmodulin is an inactive protein that becomes active when bound to calcium and serves as an interpreter for hormone and nerve-mediated messages. Ionized calcium has many functions.

68
© 2008 Thomson - Wadsworth Calcium Calcium Roles in the Body Calcium and Disease Prevention May protect against hypertension DASH diet that is rich in calcium, magnesium, and potassium May be protective relationship with blood cholesterol, diabetes, and colon cancer Calcium and Obesity Maintaining healthy body weight Calcium from dairy foods has better results than calcium from supplements. More research is needed.

69
© 2008 Thomson - Wadsworth Calcium Calcium Roles in the Body Calcium Balance Works with vitamin D Works with parathyroid hormone and calcitonin Calcium rigor develops when there are high blood calcium levels and causes the muscles to contract. Calcium tetany develops when there are low blood calcium levels and causes uncontrolled muscle contractions. Abnormalities are due to problems with hormone secretion or lack of vitamin D. Bones get robbed of calcium before blood concentrations get low.

70
© 2008 Thomson - Wadsworth

72
Calcium Calcium Roles in the Body Calcium Absorption Absorption rate for adults is 25% of calcium consumed. Calcium-binding protein is needed for calcium absorption.

73
© 2008 Thomson - Wadsworth Calcium Factors that enhance absorption Stomach acid Vitamin D Lactose Growth hormones Factors that inhibit absorption Lack of stomach acid Vitamin D deficiency High phosphorus intake High-fiber diet Phytates in seeds, nuts, and grains Oxalates in beet greens, rhubarb, and spinach

74
© 2008 Thomson - Wadsworth Calcium Calcium Recommendations and Sources Calcium Recommendations (1997 Adequate Intake) AI Adolescents: 1300 mg/day AI Adults: 1000 mg/day if 19-50 years of age AI Adults: 1200 mg/day if greater than 50 years of age Upper level for adults: 2500 mg/day Peak bone mass is the bone’s fullest potential in size and density developed in the first three decades of life.
 AI Adolescents: 1300 mg/day AI Adults: 1000 mg/day if years of age AI Adults: 1200 mg/day if greater than 50 years of age Upper level for adults: 2500 mg/day Peak bone mass is the bone’s fullest potential in size and density developed in the first three decades of life.")
75
© 2008 Thomson - Wadsworth Calcium Calcium Recommendations and Sources Calcium in Milk Products Drink milk. Eat yogurt and cheese. Add dry milk during food preparation.

76
© 2008 Thomson - Wadsworth

77
Calcium Calcium Recommendations and Sources Calcium in Other Foods Tofu, corn tortillas, some nuts and seeds Mustard and turnip greens, broccoli, bok choy, kale, parsley, watercress, and seaweed (nori) Legumes Oysters and small fish consumed with bones Mineral waters, calcium-fortified orange juice, fruit and vegetable juices, high-calcium milk Calcium-fortified cereals and breads
 Legumes Oysters and small fish consumed with bones Mineral waters, calcium-fortified orange juice, fruit and vegetable juices, high-calcium milk Calcium-fortified cereals and breads")
78
© 2008 Thomson - Wadsworth

79
Fig. 12-15, p. 420 Cauliflower, watercress, brussels sprouts, rutabaga, kale, mustard greens, bok choy, broccoli, turnip greens ≥ 50% absorbed ≈ 30% absorbed Milk, calcium-fortified soy milk, calcium-set tofu, cheese, yogurt, calcium- fortified foods and beverages ≈ 20% absorbed Almonds, sesame seeds, pinto beans, sweet potatoes ≤ 5% absorbed Spinach, rhubarb, Swiss chard Stepped Art

80
© 2008 Thomson - Wadsworth Calcium Calcium Deficiency Osteoporosis is the disease where the bones become porous and fragile due to mineral losses. No obvious symptoms of mineral loss in bones appear. It is silent. Deficiency in children can present as stunted growth. Toxicity symptoms include constipation, increased risk of urinary stone formation, kidney dysfunction, and interference with the absorption of other minerals.

81
© 2008 Thomson - Wadsworth

82
Phosphorus Most of the phosphorus is found in the bones and teeth. It is also important in energy metabolism, as part of phospholipids, and as part of genetic materials.

83
© 2008 Thomson - Wadsworth Phosphorus Phosphorus Roles in the Body Mineralization of bones and teeth Part of every cell Genetic material (DNA and RNA) Part of phospholipids Energy transfer Buffer systems that maintain acid- base balance
 Part of phospholipids Energy transfer Buffer systems that maintain acid- base balance")
84
© 2008 Thomson - Wadsworth Phosphorus Phosphorus Recommendations and Intakes (1997 RDA) RDA Adults: 700 mg/day for ages 19-70 years Upper intake level for those 19-70 years of age is 4,000 mg/day. Sources include all animal foods including meat, fish and poultry, milk and eggs Phosphorus toxicity symptoms include the calcification of nonskeletal tissues, especially the kidneys.

85
© 2008 Thomson - Wadsworth

86
Magnesium Magnesium supports bone mineralization, and is involved in energy systems and in heart functioning. It is widespread in foods.

87
© 2008 Thomson - Wadsworth Magnesium Magnesium Roles in the Body Bone mineralization Building of protein Enzyme action Normal muscle contraction Nerve impulse transmission Maintenance of teeth by preventing dental caries Functioning of the immune system Blood clotting

88
© 2008 Thomson - Wadsworth Magnesium Magnesium Intakes (1997 RDA) RDA Adult Men: 400 mg/day for 19-30 years of age RDA Adult Women: 310 mg/day for 19-30 years of age Upper level for adults: 350 mg nonfood magnesium/day Nuts and legumes, whole grains, dark green vegetables, seafood, chocolate and cocoa Hard water and some mineral waters
 RDA Adult Men: 400 mg/day for years of age RDA Adult Women: 310 mg/day for years of age Upper level for adults: 350 mg nonfood magnesium/day Nuts and legumes, whole grains, dark green vegetables, seafood, chocolate and cocoa Hard water and some mineral waters")
89
© 2008 Thomson - Wadsworth

90
Magnesium Magnesium Deficiency Deficiencies are rare. Symptoms Weakness and confusion Convulsions in extreme deficiency Bizarre muscle movements of the eye and face Hallucinations Difficulties in swallowing Growth failure in children Develops from alcohol abuse, protein malnutrition, kidney disorders and prolonged vomiting and diarrhea

91
© 2008 Thomson - Wadsworth Magnesium Magnesium and Hypertension Protects against heart disease and hypertension Low magnesium restricts walls of arteries and capillaries. Magnesium Toxicity Symptoms from nonfood magnesium are diarrhea, alkalosis, and dehydration.

92
© 2008 Thomson - Wadsworth Sulfate Sulfate requirements are met by consuming a varied diet. It is found in essential nutrients including protein. There is no recommended intake and there are no known deficiencies.

93
© 2008 Thomson - Wadsworth Osteoporosis and Calcium

94
© 2008 Thomson - Wadsworth Osteoporosis and Calcium Osteoporosis is one of the most prevalent diseases of aging. Strategies to reduce risks involve dietary calcium.

95
© 2008 Thomson - Wadsworth Bone Development and Disintegration Cortical bone is the outer shell compartment of bone. Creates the shell of long bones Creates the shell caps on the end of bones Releases calcium slower than trabecular bone Losses can begin in the 40s.

96
© 2008 Thomson - Wadsworth Bone Development and Disintegration Trabecular bone is the inner lacy matrix compartment of bone. Can be affected by hormones in the body signaling the release of calcium Provides a source for blood calcium when needed Losses can become significant in the 30s for men and women. Results in type I osteoporosis Can result in spine and wrist fractures and loss of teeth Women are affected 6 times as often as men.

97
© 2008 Thomson - Wadsworth

98
Bone Development and Disintegration Losses of both trabecular and cortical bone result in type II osteoporosis. Can result in compression fractures of the spine Hip fractures can develop. Twice as common in women as in men The diagnosis of osteoporosis is performed using bone density tests. Individual risk factors for osteoporosis are also considered.

99
© 2008 Thomson - Wadsworth

101
Age and Bone Calcium Maximizing Bone Mass Children and adolescents need to consume enough calcium and vitamin D to create denser bones. With a higher initial bone mass, the normal losses of bone density that occur with age will have less detrimental effects. Minimizing Bone Loss Ensuring adequate intakes of vitamin D and calcium are consumed Hormonal changes can increase calcium losses.

102
© 2008 Thomson - Wadsworth

103
Gender and Hormones Men at lower risk than women Hormonal changes Rapid bone loss in nonmenstruating women Medications can be used that inhibit osteoclasts or stimulate osteoblasts. Soy offers some protection.

104
© 2008 Thomson - Wadsworth Genetics and Ethnicity Genes may play a role. Environment also – diet and calcium Physical activity, body weight, alcohol, and smoking have a role.

105
© 2008 Thomson - Wadsworth Physical Activity and Body Weight Muscle strength and bone strength go together. Heavy body weights and weight gains place a stress on bones and promote bone density.

106
© 2008 Thomson - Wadsworth Smoking and Alcohol Smokers Less dense bones Damage can be reversed when smoking stops. Alcohol abuse Enhances fluid excretion, thus increases calcium losses Upsets hormonal balance for healthy bones Slows bone formation Stimulates bone breakdown Increases risks of falling

107
© 2008 Thomson - Wadsworth Nutrients Dietary Calcium – the key to prevention Other Nutrients Adequate protein Adequate vitamin D Vitamin K protects against hip fractures. Magnesium and potassium help to maintain bone mineral density. Vitamin A Omega-3 fatty acids Fruits and vegetables Reduce salt

108
© 2008 Thomson - Wadsworth A Perspective on Supplements Calcium-rich foods are best. Supplements may be needed when requirements are not met through foods. Types of supplements Antacids contain calcium carbonate. Bone meal or powdered bone, oyster shell or dolomite are calcium supplements. Contain lead?? Small doses are better absorbed. Different absorption rates from different types of calcium supplements

109
© 2008 Thomson - Wadsworth Some Closing Thoughts Age, gender and genetics are beyond control. There are effective strategies for prevention that include adequate calcium and vitamin D intake, physical activity, moderation of alcohol, abstaining from cigarettes, and supplementation if needed.

110
© 2008 Thomson - Wadsworth Chapter 13 The Trace Minerals

111
© 2008 Thomson - Wadsworth The Trace Minerals--An Overview Trace minerals are needed in very small quantities in the human body. They perform many essential functions important to health. Toxic levels can easily be reached with the use of supplements. Humans can get the amounts of trace minerals needed by consuming a wide variety of foods.

112
© 2008 Thomson - Wadsworth The Trace Minerals--An Overview Food Sources Depends on soil and water composition Depends on processing Bioavailability Wide variety of unprocessed foods

113
© 2008 Thomson - Wadsworth The Trace Minerals--An Overview Deficiencies Severe deficiencies of some minerals are easy to recognize, while others can be difficult to diagnose. Mild deficiencies are easily overlooked. Deficiencies have wide-reaching effects. Deficiencies affect all ages, but in children, they can affect growth.

114
© 2008 Thomson - Wadsworth The Trace Minerals--An Overview Toxicities Do not exceed Tolerable Upper Intake Levels. FDA does not limit amounts in supplements. Do not exceed 100% Daily Values. Interactions Common and coordinated to meet body needs Can lead to nutrient imbalances

115
© 2008 Thomson - Wadsworth Iron Iron is an essential nutrient found in the body as a part of hemoglobin and myoglobin. Iron is used for energy metabolism and enzyme activity. Special proteins assist with iron absorption, transport, and storage. Both iron deficiency and iron toxicity cause damage so balance is important. Heme iron is better absorbed but nonheme iron absorption can be enhanced.

116
© 2008 Thomson - Wadsworth Iron Iron Roles in the Body Ferrous iron is reduced and has a net positive charge of two. Ferric iron is oxidized and has a net positive charge of three. Cofactor in oxidation-reduction reactions Utilization of energy in cell metabolism Part of the protein hemoglobin which carries oxygen in the blood Part of the protein myoglobin in the muscles which makes oxygen available for muscle contractions

117
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Iron Absorption The protein ferritin stores iron in the mucosal cells lining the digestive tract. Transfers iron to mucosal transferrin. Transfers iron to blood transferrin Transports iron to the cells Excreted and replaced as needed

118
© 2008 Thomson - Wadsworth

119
Fig. 13-1, p. 443 If the body does not need iron Iron is not absorbed and is excreted in shed intestinal cells instead. Thus, iron absorption is reduced when the body does not need iron. If the body needs iron Stepped Art Mucosal cells in the intestine store excess iron in mucosal ferritin (a storage protein). Iron in food Mucosal ferritin releases iron to mucosal transferrin (a transport protein), which hands off iron to another transferrin that travels through the blood to the rest of the body.
. Iron in food Mucosal ferritin releases iron to mucosal transferrin (a transport protein), which hands off iron to another transferrin that travels through the blood to the rest of the body..")
120
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Heme and Nonheme Iron Heme iron –Found in foods that are from the flesh of animals (meat, poultry, and fish) –Represents only 10% of a days iron consumption, but has an absorption rate of 25% Nonheme iron –Found in plant-derived and animal-derived foods –Has an absorption rate of 17%
 –Represents only 10% of a days iron consumption, but has an absorption rate of 25% Nonheme iron –Found in plant-derived and animal-derived foods –Has an absorption rate of 17%")
121
© 2008 Thomson - Wadsworth

122
Heme accounts for about 10% of the average daily iron intake, but it is well absorbed (about 25%). Nonheme iron accounts for the remaining 90%, but it is less well absorbed (about 17%). Fig. 13-2, p. 444 Only foods derived from animal flesh provide heme, but they also contain nonheme iron. All of the iron in foods derived from plants is nonheme iron. Key: Heme Nonheme Stepped Art
. Fig. 13-2, p. 444 Only foods derived from animal flesh provide heme, but they also contain nonheme iron. All of the iron in foods derived from plants is nonheme iron. Key: Heme Nonheme Stepped Art.")
123
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Absorption-Enhancing Factors –MFP factor enhances the absorption of nonheme iron. –When nonheme iron is consumed with vitamin C at the same meal, absorption of iron increases. –Citric acid and lactic acid from foods, HCl from the stomach, and sugars enhance nonheme iron absorption.

124
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Absorption-Inhibiting Factors Phytates and fibers from legumes, grains, and rice Vegetable proteins in soybeans, legumes, and nuts Calcium in milk Tannic acid and other polyphenols in tea, coffee, grains, oregano, and red wine Dietary Factors Combined Difficult to assess iron absorption with meal consumption Most relevant factors are MFP factor and vitamin C in enhancing absorption and phytates in inhibiting absorption

125
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Individual Variation Dietary factors Health status Stage in life cycle Iron status

126
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Iron Transport and Storage Surplus is stored in bone marrow, spleen, and liver Hemosiderin is a storage protein used when concentrations of iron are extremely high. Storing excess iron is a protective measure because iron can act as a free radical.

127
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Iron Recycling The liver and spleen dismantle red blood cells and package iron into transferrin. Transferrin carries iron in the blood. Bone marrow incorporates iron into hemoglobin and stores iron as ferritin. Iron-containing hemoglobin carries oxygen in the blood. Iron is lost when bleeding occurs and through the GI tract.

128
© 2008 Thomson - Wadsworth

129
Some iron delivered to myoglobin of muscle cells Some losses if bleeding occurs Iron-containing hemoglobin in red blood cells carries oxygen. Transferrin carries iron in blood. Fig. 13-3, p. 445 Some losses via sweat, skin, and urine Stepped Art Bone marrow incorporates iron into hemoglobin of red blood cells and stores excess iron in ferritin (and hemosiderin). Liver (and spleen) dismantles red blood cells, packages iron into transferrin, and stores excess iron in ferritin (and hemosiderin).
. Liver (and spleen) dismantles red blood cells, packages iron into transferrin, and stores excess iron in ferritin (and hemosiderin)..")
130
© 2008 Thomson - Wadsworth Iron Iron Absorption and Metabolism Iron Balance The absorption, transport, storage, recycling, and loss of iron must be regulated in order to maintain iron balance. Hepcidin is a hormone that inhibits the absorption and transport of iron to keep blood levels within normal ranges.

131
© 2008 Thomson - Wadsworth Iron Iron deficiency is the most common nutrient deficiency. Iron-deficiency anemia can affect individuals in many stages of life. Vulnerable Stages of Life Women in reproductive years due to menstruation Pregnant women due to the needs of the infant, increases in blood volume, and loss of blood during the birthing process Infants and young children due to rapid growth Teenagers due to rapid growth in males and menstruation in females

132
© 2008 Thomson - Wadsworth

133
Iron Iron Deficiency Blood Losses Can be from non-obvious sources such as a bleeding ulcer Malaria and parasites Giving a pint of blood results in a loss of about 2.5 mg iron. Menstruation

134
© 2008 Thomson - Wadsworth Iron Iron Deficiency Assessment of Iron Deficiency Stage 1 – Iron stores diminish; measured by serum ferritin Stage 2 – Transport iron decreases; measured by transferrin saturation Stage 3 – Hemoglobin production declines; erythrocyte protoporphyrin accumulates and hematocrit declines. Hemoglobin and hematocrit are late indicators of iron status.

135
© 2008 Thomson - Wadsworth Iron Iron Deficiency Iron Deficiency and Anemia Iron deficiency is when there is depletion of the body’s iron stores. Iron-deficiency anemia is the severe depletion of iron stores. Also called microcytic (small) hypochromic (pale) anemia. Symptoms include fatigue, weakness, headaches, apathy, pallor and poor resistance to cold temperatures.
 hypochromic (pale) anemia. Symptoms include fatigue, weakness, headaches, apathy, pallor and poor resistance to cold temperatures..")
136
© 2008 Thomson - Wadsworth Iron Iron Deficiency Iron Deficiency and Behavior Energy metabolism is impaired. Neurotransmitter synthesis is reduced. Physical work capacity and mental productivity are reduced. Symptoms of a deficiency may be confused with behavioral issues. Iron Deficiency and Pica Generally found in women and children from low- income groups Eating ice, clay, paste, and other nonfood substances Eating nonfood substances will not correct the deficiency.

137
© 2008 Thomson - Wadsworth Iron Iron Toxicity Iron Overload Hemochromatosis is generally a genetic disorder that enhances iron absorption and may be caused by a lack of hepcidin. Iron overload can also be caused by: –Repeated blood transfusions –Massive doses of supplemental iron –Rare metabolic disorders

138
© 2008 Thomson - Wadsworth Iron Iron Overload Hemosiderosis may develop from excessive iron where there are large deposits of hemosiderin in the liver, heart, joints, and other tissues. Symptoms of iron overload include apathy, lethargy, and fatigue. Problems include liver tissue damage and infections. Higher risk of diabetes, liver cancer, heart disease, and arthritis More common in men then in women

139
© 2008 Thomson - Wadsworth Iron Iron Toxicity Iron and Heart Disease – may be a link to high iron stores Iron and Cancer – may be a link with free radical activity resulting in damage to DNA Iron Poisoning UL for adults: 45 mg/day Accidental supplement poisoning in children Symptoms include nausea, vomiting, diarrhea, constipation, rapid heartbeat, weak pulse, dizziness, shock, and confusion

140
© 2008 Thomson - Wadsworth Iron Iron Recommendations and Sources Recommended Iron Intakes (2001 RDA) RDA Men: 8 mg/day for adults 19-50 years of age RDA Women: 18 mg/day for adults 19-50 years of age RDA Women: 8 mg/day for adults over 51 years of age Vegetarians need 1.8 times as much iron because of low bioavailability.
 RDA Men: 8 mg/day for adults years of age RDA Women: 18 mg/day for adults years of age RDA Women: 8 mg/day for adults over 51 years of age Vegetarians need 1.8 times as much iron because of low bioavailability.")
141
© 2008 Thomson - Wadsworth Iron Iron Recommendations and Sources Iron in Foods Red meats, fish, poultry, and shellfish Eggs Legumes Grain products (whole-grain, enriched, and fortified breads and cereals) Dark greens and dried fruits Iron-Enriched Foods Often added to grain foods Not absorbed as well
 Dark greens and dried fruits Iron-Enriched Foods Often added to grain foods Not absorbed as well")
142
© 2008 Thomson - Wadsworth

143
Iron Iron Recommendations and Sources Maximizing Iron Absorption Bioavailability is high in meats, fish, and poultry. Bioavailability is intermediate in grains and legumes. Bioavailability is low in vegetables. Combined effect of enhancing and inhibiting factors

144
© 2008 Thomson - Wadsworth Iron Iron Contamination and Supplementation Contamination Iron Iron cookware takes up iron salts. Acidic foods and long cooking times increase uptake of iron salts. Iron Supplements Best absorbable form is ferrous sulfate or an iron chelate Take on empty stomach and with liquids other than milk, tea, or coffee Vitamin C enhances food iron absorption, not supplement absorption. Side effect of constipation

145
© 2008 Thomson - Wadsworth Zinc Zinc is important in a multitude of chemical reactions in the body. The best sources of dietary zinc are protein- rich foods. Zinc from pancreatic secretions is also available for absorption. Phytates and fiber can bind zinc, therefore limiting absorption. A special binding protein monitors the absorption of zinc. Zinc deficiency symptoms include growth retardation and sexual immaturity.

146
© 2008 Thomson - Wadsworth Zinc Zinc Roles in the Body Supports the work of metalloenzymes Helps to make parts of DNA and RNA Manufactures heme for hemoglobin Assists in essential fatty acid metabolism Releases vitamin A from liver stores Metabolizes carbohydrates Synthesizes proteins Metabolizes alcohol Disposes of damaging free radicals

147
© 2008 Thomson - Wadsworth Zinc Zinc Roles in the Body Involved in growth, development, and immune function Affects platelets in blood clotting and wound healing Needed to produce the retinal form of vitamin A Affects thyroid hormone function Influences behavior and learning performance Taste perception Wound healing Sperm development Fetal development

148
© 2008 Thomson - Wadsworth Zinc Zinc Absorption and Metabolism Zinc Absorption Rate of absorption depends on zinc status; when more is needed, more will be absorbed. Phytates and fiber bind zinc and reduce absorption. Metallothionein is a special protein that holds zinc in storage.

149
© 2008 Thomson - Wadsworth Zinc Zinc Absorption and Metabolism Zinc Recycling Enteropancreatic circulation – travels from the pancreas to the intestines and back Losses occur in the feces, urine, shedding of skin, hair, sweat, menstrual fluids, and semen.

150
© 2008 Thomson - Wadsworth

151
If the body needs zinc If the body does not need zinc Mucosal cells in the intestine store excess zinc in metallothionein. Zinc is not absorbed and is excreted in shed intestinal cells instead. Thus, zinc absorption is reduced when the body does not need zinc. Metallothionein releases zinc to albumin and transferrin for transport to the rest of the body. Zinc in food The pancreas uses zinc to make digestive enzymes and secretes them into the intestine. Fig. 13-6, p. 453 Stepped Art

152
© 2008 Thomson - Wadsworth Zinc Zinc Absorption and Metabolism Zinc Transport Transported by the protein albumin Binds to transferrin Excessive iron and copper can lead to a zinc deficiency and excessive zinc can lead to an iron and copper deficiency.

153
© 2008 Thomson - Wadsworth Zinc Zinc Deficiency Not widespread Occurs in pregnant women, young children, the elderly, and the poor Symptoms of deficiency Growth retardation Delayed sexual maturation Impaired immune function Hair loss, eye and skin lesions Altered taste, loss of appetite, and delayed wound healing

154
© 2008 Thomson - Wadsworth

155
Zinc Zinc Toxicity UL for Adults: 40 mg/day Symptoms Loss of appetite Impaired immunity Low HDL Copper and iron deficiencies Vomiting and diarrhea Exhaustion Headaches

156
© 2008 Thomson - Wadsworth Zinc Zinc Recommendations and Sources Recommended intakes (2001 RDA) RDA Men: 11 mg/day RDA Women: 8 mg/day Zinc in foods Shellfish, meats, poultry, milk, and cheese Whole grains and legumes Zinc Supplementation Developing countries use zinc to reduce incidence of disease and diarrhea. Zinc lozenges for the common cold are controversial and inconclusive.

157
© 2008 Thomson - Wadsworth

158
Iodine Iodide is an essential component of the thyroid hormone that helps to regulate metabolism. Iodine deficiency can cause simple goiter and cretinism. The iodization of salt has greatly reduced iodine deficiency in the United States and Canada.

159
© 2008 Thomson - Wadsworth Iodine Iodide Roles in the Body Component of two thyroid hormones (T 3 and T 4 ) Regulates body temperature, growth, development, metabolic rate, nerve and muscle function, reproduction, and blood cell production.
 Regulates body temperature, growth, development, metabolic rate, nerve and muscle function, reproduction, and blood cell production.")
160
© 2008 Thomson - Wadsworth Iodine Iodine Deficiency Simple goiter is the enlargement of the thyroid gland caused by iodine deficiency. Goiter is enlargement of the thyroid gland due to malfunction of the gland, iodine deficiency or overconsumption of goitrogens. Goitrogen (antithyroid) overconsumption – naturally occurring in cabbage, spinach, radishes, rutabaga, soybeans, peanuts, peaches, and strawberries. Cretinism is a congenital disease characterized by mental and physical retardation and commonly caused by maternal iodine deficiency during pregnancy.
 overconsumption – naturally occurring in cabbage, spinach, radishes, rutabaga, soybeans, peanuts, peaches, and strawberries. Cretinism is a congenital disease characterized by mental and physical retardation and commonly caused by maternal iodine deficiency during pregnancy..")
161
© 2008 Thomson - Wadsworth

162
Iodine Iodine Toxicity UL 1100 μg/day Symptoms include underactive thyroid gland, elevated TSH, and goiter. Supplement use, medications, and excessive iodine from foods

163
© 2008 Thomson - Wadsworth Iodine Iodine Recommendations and Sources Recommendations (2001 RDA) – Adults: 150 μg/day Sources Iodized salt Seafood Bread and dairy products Plants grown in iodine-rich soils Animals that feed on plants grown in iodine-rich soils
 – Adults: 150 μg/day Sources Iodized salt Seafood Bread and dairy products Plants grown in iodine-rich soils Animals that feed on plants grown in iodine-rich soils")
164
© 2008 Thomson - Wadsworth Selenium Selenium is an antioxidant nutrient associated with protein foods. It may provide some protection against certain types of cancer. Selenium Roles in the Body Defends against oxidation Regulates thyroid hormone

165
© 2008 Thomson - Wadsworth Selenium Selenium Deficiency Keshan disease – a pre-disposition to heart disease where a virus causes the cardiac tissue to become fibrous Prevalent in regions of China because the soil is low in selenium

166
© 2008 Thomson - Wadsworth Selenium Selenium and Cancer May protect against certain forms of cancer Inconclusive evidence and more research is needed Food sources are better than supplements.

167
© 2008 Thomson - Wadsworth Selenium Selenium Recommendations and Sources Recommendations (2000 RDA) – Adults: 55 μg/day Sources include seafood, meat, whole grains, and vegetables (depends on soil content).
 – Adults: 55 μg/day Sources include seafood, meat, whole grains, and vegetables (depends on soil content).")
168
© 2008 Thomson - Wadsworth Selenium Selenium Toxicity UL for Adults: 400 μg/day Symptoms Loss and brittleness of hair and nails Skin rash, fatigue, irritability, and nervous system disorders Garlic breath odor

169
© 2008 Thomson - Wadsworth Copper Copper is a component of several enzymes associated with oxygen or oxidation. Copper deficiency is rare. There are some diseases associated with excessive intakes. Food sources of copper include legumes, whole grains, and seafood.

170
© 2008 Thomson - Wadsworth Copper Copper Roles in the Body Absorption and use of iron in the formation of hemoglobin Part of several enzymes Some copper-containing enzymes are antioxidants. Required for many metabolic reactions

171
© 2008 Thomson - Wadsworth Copper Copper Deficiency and Toxicity Deficiency is rare in the U.S.; however, symptoms include anemia and bone abnormalities. In Menkes disease, copper cannot be released into the circulation. Toxicity UL for Adults: 10,000 μg/day (10 mg/day) In Wilson’s disease, copper builds up in the liver and brain. Excessive intake from supplements can cause liver damage.
 In Wilson’s disease, copper builds up in the liver and brain. Excessive intake from supplements can cause liver damage..")
172
© 2008 Thomson - Wadsworth Copper Copper Recommendations and Sources Recommendations (2001 RDA) – Adults: 900 μg/day Sources Seafood, nuts, seeds and legumes Whole grains In houses with copper plumbing, water can be a source.
 – Adults: 900 μg/day Sources Seafood, nuts, seeds and legumes Whole grains In houses with copper plumbing, water can be a source.")
173
© 2008 Thomson - Wadsworth Manganese Manganese is a cofactor for several enzymes involved in bone formation and various metabolic processes. Deficiencies are rare and toxicities are associated with environmental contamination. Manganese is found in many foods. Manganese Roles in the Body Cofactor for several enzymes Assists in bone formation Pyruvate conversion

174
© 2008 Thomson - Wadsworth Manganese Manganese Deficiency and Toxicity Deficiency symptoms are rare. Phytates, calcium and iron limit absorption. Toxicity occurs with environmental contamination. UL for Adults: 11 mg/day Toxicity symptoms include nervous system disorders.

175
© 2008 Thomson - Wadsworth Manganese Manganese Recommendations and Sources Recommendations (2001 AI) AI Men: 2.3 mg/day AI Women: 1.8 mg/day Sources Nuts Whole grains Leafy vegetables Tea
 AI Men: 2.3 mg/day AI Women: 1.8 mg/day Sources Nuts Whole grains Leafy vegetables Tea")
176
© 2008 Thomson - Wadsworth Fluoride Fluoride makes bones stronger and teeth more resistant to decay. The use of fluoridated water can reduce dental caries. Excess fluoride causes fluorosis—the pitting and discoloration of teeth.

177
© 2008 Thomson - Wadsworth Fluoride Fluoride Roles in the Body Formation of teeth and bones Helps to make teeth resistant to decay Fluorapatite is the stabilized form of bone and tooth crystals Fluoride and Dental Caries Widespread health problem Leads to nutritional problems due to issues with chewing

178
© 2008 Thomson - Wadsworth

179
Fluoride Fluoride and Toxicity Tooth damage called fluorosis – irreversible pitting and discoloration of the teeth UL for Adults: 10 mg/day Prevention of fluorosis Monitor fluoride content of local water supply. Supervise toddlers during tooth brushing. Watch quantity of toothpaste used (pea size) for toddlers. Use fluoride supplements only if prescribed by a physician.
 for toddlers. Use fluoride supplements only if prescribed by a physician..")
180
© 2008 Thomson - Wadsworth

181
Fluoride Fluoride Recommendations and Sources Recommendations (1997 AI) AI Men: 3.8 mg/day AI Women: 3.1 mg/day Sources Fluoridated drinking water Seafood and tea
 AI Men: 3.8 mg/day AI Women: 3.1 mg/day Sources Fluoridated drinking water Seafood and tea")
182
© 2008 Thomson - Wadsworth Chromium Chromium is an essential nutrient that enhances insulin’s action. It is widely available in unrefined foods. Chromium Roles in the Body Enhances insulin action Low chromium levels can result in elevated blood sugar levels. Glucose tolerance factors (GTF) are small organic compounds that enhance insulin’s action and some contain chromium.
 are small organic compounds that enhance insulin’s action and some contain chromium..")
183
© 2008 Thomson - Wadsworth Chromium Chromium Recommendations and Sources Recommendations (2001 AI) AI Men: 35 μg/day AI Women: 25 μg/day Sources Meat, especially liver Whole grains Brewer’s yeast Chromium Supplements Claims about reducing body fat and improving muscle strength remain controversial.
 AI Men: 35 μg/day AI Women: 25 μg/day Sources Meat, especially liver Whole grains Brewer’s yeast Chromium Supplements Claims about reducing body fat and improving muscle strength remain controversial.")
184
© 2008 Thomson - Wadsworth Molybdenum Molybdenum is a cofactor in several enzymes. It is needed in minuscule amounts. It is available in legumes, grains, and organ meats. Molybdenum functions as a cofactor for several enzymes. No deficiency symptoms No reported toxicity symptoms in humans

185
© 2008 Thomson - Wadsworth Molybdenum Recommendations (2001 RDA) Adults: 45 μg/day UL Adults: 2 mg/day Food sources include legumes, grains, and organ meats.
 Adults: 45 μg/day UL Adults: 2 mg/day Food sources include legumes, grains, and organ meats.")
186
© 2008 Thomson - Wadsworth Other Trace Minerals Much of the research on other trace minerals is from animal studies. Humans need very small amounts. Determining exact needs, functions, deficiencies, and toxicities is difficult. Some key roles of these other trace minerals have been identified.

187
© 2008 Thomson - Wadsworth Other Trace Minerals Nickel is a cofactor for certain enzymes. Silicon is used in bone and collagen formation. Vanadium is for growth, development, and normal reproduction. Cobalt is a key component of vitamin B 12. Boron may be key in brain activities. Arsenic is useful in some types of leukemia.

188
© 2008 Thomson - Wadsworth

189
Contaminant Minerals Contaminate minerals are also called heavy metals. These include mercury, lead, and cadmium. These minerals enter the food supply through soil, water, and air pollution. They disrupt body processes and impair nutrition status.

190
© 2008 Thomson - Wadsworth Contaminant Minerals Lead toxicity symptoms in children Learning disabilities in children Low IQ Behavior problems Slow growth Dental caries Iron-deficiency anemia Sleep disturbances like night walking, restlessness, and head banging Nervous system disorders and seizures Slow reaction time and poor coordination Impaired hearing

191
© 2008 Thomson - Wadsworth Contaminant Minerals Lead toxicity symptoms in adults Hypertension Reproductive complications Kidney failure

192
© 2008 Thomson - Wadsworth Phytochemicals and Functional Foods

193
© 2008 Thomson - Wadsworth Phytochemicals and Functional Foods Phytochemicals are nonnutrient compounds. Only a few of the thousands of phytochemicals have been researched. There are many questions and few answers about their role in human health. Foods that provide health benefits beyond those of nutrients are now called functional foods. Some have an identified role in disease prevention.

194
© 2008 Thomson - Wadsworth The Phytochemicals The phytochemicals give foods taste, aroma, color, and other characteristics. Defending against Cancer Phytoestrogens mimic estrogen Found in soybeans, legumes, flaxseeds, whole grains, fruits and vegetables Antioxidant activity Slow the growth of breast and prostrate cancer Supplements may stimulate the growth of cancers that depend upon estrogen.

195
© 2008 Thomson - Wadsworth The Phytochemicals Defending against Cancer Lycopene Powerful antioxidant Inhibits the growth of cancer cells Found in tomatoes and cooked tomato products, apricots, guava, papaya, pink grapefruits, and watermelon Five servings of fruits and vegetables are recommended every day.

196
© 2008 Thomson - Wadsworth The Phytochemicals Defending against Heart Disease Flavonoids in foods Powerful antioxidants Protect against LDL cholesterol oxidation and reduce blood platelet stickiness Lowers risk of chronic diseases Found in whole grains, legumes, soy, vegetables, fruits, herbs, spices, teas, chocolate, nuts, olive oil, and red wines

197
© 2008 Thomson - Wadsworth The Phytochemicals Defending against Heart Disease Carotenoids in foods especially lutein and lycopene Lower risk of heart disease Found in fruits and vegetables Phytosterols May protect against heart disease Inhibit cholesterol absorption Lower blood pressure Act as antioxidants Found in soybeans and other vegetables Lignans, found in flax seed, are converted to phytosterols by intestinal bacteria.

198
© 2008 Thomson - Wadsworth

199
The Phytochemicals The Phytochemicals in Perspective Difficult to assess one food and its benefits alone Actions of phytochemicals are complementary and overlapping

200
© 2008 Thomson - Wadsworth Functional Foods Foods as Pharmacy Margarine enhanced with a phytosterol may lower cholesterol. May be more useful in prevention and mild cases of disease. Drugs are used for severe cases of disease.

201
© 2008 Thomson - Wadsworth Functional Foods Unanswered Questions Research is lagging behind food manufacturers. Consumer questions to ask Does it work? How much does it contain? Is it safe? Is it healthy?

202
© 2008 Thomson - Wadsworth Functional Foods Future Foods Use of gene research Can we design foods to meet exact health needs of each individual? Can farmers grow the “perfect” foods?

203
© 2008 Thomson - Wadsworth Chapter 18 Diet and Health

204
© 2008 Thomson - Wadsworth Nutrition and Infectious Diseases Personal strategies to prevent infectious disease are important. Nutrition intervention can help prevent malnutrition and minimize the wasting that accompanies AIDS. There are new threats of the spread of disease-causing microorganisms due to bioterrorism.

205
© 2008 Thomson - Wadsworth Nutrition and Infectious Diseases The Immune System Organs of the immune system fight antigens Spleen Lymph nodes Thymus Phagocytes Engulf and digest invaders; a process is called phagocytosis Secrete special proteins called cytokins that activate a metabolic and immune response

206
© 2008 Thomson - Wadsworth Nutrition and Infectious Diseases The Immune System Lymphocytes: B-cells Produce antibodies that react selectively, part of a class of proteins called immunoglobulins Retain memory to react faster with the same foreign organism Resistance to infection Lymphocytes: T-cells Release powerful chemicals to destroy foreign particles Highly specific, attacking only one antigen Defend against fungi, viruses, parasites, some bacteria, and cancer cells Participate in the rejection of transplanted tissue

207
© 2008 Thomson - Wadsworth Nutrition and Infectious Diseases Nutrition and Immunity Malnutrition compromises immunity. Immunity and infectious disease increase nutrient needs and lower food intake. The synergistic downward cycle of disease and malnutrition must be broken for recovery to occur. Opportunistic infections develop when the immune system is suppressed.

208
© 2008 Thomson - Wadsworth

209
Nutrition and Infectious Diseases HIV and AIDS HIV (human immunodeficiency virus) is the infection that attacks the immune system and disables the body’s defenses. AIDS (acquired immune deficiency syndrome) is the infectious disease that destroys health and life. Epidemic Early detection and early intervention are critical.
 is the infectious disease that destroys health and life. Epidemic Early detection and early intervention are critical..")
210
© 2008 Thomson - Wadsworth

212
Nutrition and Chronic Diseases Four of the top ten causes of death are related to diet. There are also genetic and lifestyle risk factors that are important and related to chronic disease. Many of the nutritional factors in the treatment of chronic disease are interrelated.

213
© 2008 Thomson - Wadsworth

214
Cardiovascular Disease Atherosclerotic plaques can raise blood pressure, cause abnormal blood clotting, and cause heart attacks and strokes. There are many recommendations for prevention and treatment including dietary interventions, quitting smoking and engaging in regular physical activity. The most common form of CVD is coronary heart disease (CHD), which develops due to atherosclerosis in the coronary arteries.
, which develops due to atherosclerosis in the coronary arteries..")
215
© 2008 Thomson - Wadsworth Cardiovascular Disease How Atherosclerosis Develops Atheromatous plaque builds on artery walls and leads to inflammation. Causes of Atherosclerosis Cells lining the blood vessels incur damage. Inflammatory response using macrophages that become the cells of plaque Blood clots form and minerals harden the plaque. Fibrous connective tissue C-reactive protein (CRP) is a sign of inflammation of the artery walls.
 is a sign of inflammation of the artery walls..")
216
© 2008 Thomson - Wadsworth Cardiovascular Disease How Atherosclerosis Develops Plaques Fibrous coating can be torn away with a surge in blood pressure Blood Clots Platelets cover the damaged area and form a clot. Thrombosis is a blood clot that sticks to an artery and grows large enough to restrict or close off a blood vessel. Embolism is when a blood clot breaks free, travels, and lodges in a small artery and shuts off blood flow to tissues. Platelets are under the control of eicosanoids, made from omega-3 and omega-6 fatty acids.

217
© 2008 Thomson - Wadsworth Cardiovascular Disease How Atherosclerosis Develops Blood Pressure and Atherosclerosis Arteries are narrowed due to plaque, clots, or both. The heart must generate more pressure to deliver blood to the tissues. Higher blood pressure results in further damages. The Result: Heart Attacks and Strokes Angina – pain or pressure feeling around the area of the heart Heart attack – restricted blood flow to the heart Transient ischemic attack or stroke – restricted blood flow to the brain

218
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Diet and physical activity are modifiable risk factors. Age, Gender, and Family History Cannot change these factors Men higher risk than women Men older than 45 years of age Women older than 55 years of age Immediate family history of premature heart disease

219
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease High LDL and Low HDL Cholesterol LDL –Excess LDL (low-density lipoproteins) become available for oxidation, high risk –Risk factors for LDL cholesterol »Desirable: <100 mg/dL »Above optimum level: 100-129 mg/dL »Borderline: 130-159 mg/dL »High: 160-189 mg/dL »Very High: >190 mg/dL
 become available for oxidation, high risk –Risk factors for LDL cholesterol »Desirable: <100 mg/dL »Above optimum level: mg/dL »Borderline: mg/dL »High: mg/dL »Very High: >190 mg/dL")
220
© 2008 Thomson - Wadsworth Cardiovascular Disease High LDL and Low HDL Cholesterol HDL HDL (high-density lipoproteins) represent cholesterol being carried back to the liver, reduced risk Risk factors for HDL cholesterol –Desirable: ≥60 mg/dL –Borderline: 59-40 mg/dL –High: <40 mg/dL
 represent cholesterol being carried back to the liver, reduced risk Risk factors for HDL cholesterol –Desirable: ≥60 mg/dL –Borderline: mg/dL –High: <40 mg/dL")
221
© 2008 Thomson - Wadsworth Cardiovascular Disease High LDL and Low HDL Cholesterol Total cholesterol Desirable levels at < 200 mg/dL Borderline levels at 200-239 mg/dL High levels at ≥ 240 mg/dL

222
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease High Blood Pressure (Hypertension) Injures artery walls and accelerates plaque formation which in turn increases blood pressure Blood pressure (systolic and/or diastolic pressure) –Desirable: <120/<80 –Borderline: 120-139/80-89 (prehypertension) –High: ≥140/≥90 – stage one hypertension –Stage two hypertension: ≥160/≥100
 Injures artery walls and accelerates plaque formation which in turn increases blood pressure Blood pressure (systolic and/or diastolic pressure) –Desirable: <120/<80 –Borderline: /80-89 (prehypertension) –High: ≥140/≥90 – stage one hypertension –Stage two hypertension: ≥160/≥100")
223
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Diabetes Risk similar to people with established CHD CHD risk equivalents

224
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Obesity and Physical Inactivity Obesity, especially abdominal obesity, and physical inactivity increase risk Body mass index –Desirable: 18.5-24.9 –Borderline: 25-29.9 –High: ≥30 Weight loss and regular physical activity are protective.

225
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Cigarette Smoking Powerful increased risk Increases blood pressure and the workload of the heart Atherogenic Diet A diet high in saturated fats, trans fats, and cholesterol and low in fruits and vegetables elevates LDL cholesterol. Antioxidants and omega-3 fatty acids lower the risk of CHD.

226
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Other Risk Factors Emerging risk factors and predictions Elevated triglycerides are a marker for other risk factors and being studied in relation to CHD –Desirable levels of fasting triglycerides: <150 mg/dL –Borderline levels of fasting triglycerides: 150-199 mg/dL –High levels of fasting triglycerides: 200-499 mg/dL –Very high levels of fasting triglycerides: ≥ 500 mg/dL Diabetes and overweight

227
© 2008 Thomson - Wadsworth Cardiovascular Disease Risk Factors for Coronary Heart Disease Metabolic Syndrome Also called Syndrome X or insulin resistance syndrome Insulin resistance is a risk factor

228
© 2008 Thomson - Wadsworth Cardiovascular Disease Metabolic Syndrome Any three of the following factors Abdominal obesity –Men: Waist circumference >40 inches –Women: waist circumference >35 inches Triglycerides: ≥150 mg/dL HDL: <40 mg/dL in men, <50 mg/dL in women Blood pressure: ≥130/85 mm Hg Fasting glucose: ≥100 mg/dL

229
© 2008 Thomson - Wadsworth Cardiovascular Disease Recommendations for Reducing Coronary Heart Disease Risk Cholesterol Screening – at least two times at least one week apart Lifestyle Changes Balance energy intake with energy needs. Include lean meats, vegetables, and low-fat milk products. Limit foods with high concentrations of saturated fatty acids (< 7% of total kcalories) and trans- fatty acids (< 1% of total kcalories). Limit foods with a high content of cholesterol (< 300 mg/day). Choose foods high in soluble fiber: vegetables, fruits, and whole grains.
 and trans- fatty acids (< 1% of total kcalories). Limit foods with a high content of cholesterol (< 300 mg/day). Choose foods high in soluble fiber: vegetables, fruits, and whole grains..")
230
© 2008 Thomson - Wadsworth Cardiovascular Disease Lifestyle Changes High-potassium, low-sodium foods Limit sodium to 2,300 mg/day. Limit intake of added sugar. Consume fatty fish at least twice a week for omega- 3 fatty acids. Consume foods with plant sterols or stanols added. Use soy products in place of animal foods that are high in saturated fat and cholesterol. Limit alcohol consumption to 1 drink/day for women or 2 drinks/day for men. Exercise at least 30 minutes most days of the week to expend 2,000 kcalories weekly. Reduce exposure to tobacco smoke.

231
© 2008 Thomson - Wadsworth Hypertension Hypertension with accompanying atherosclerosis can cause heart attacks and strokes. Weight control is the most effective dietary strategy for treating hypertension.

232
© 2008 Thomson - Wadsworth Hypertension How Hypertension Develops Blood flow to the kidneys is reduced so the kidneys expand blood volume and constrict peripheral blood vessels, resulting in peripheral resistance and thus raising blood pressure. Cardiac output increases, increasing the work of the heart.

233
© 2008 Thomson - Wadsworth

234
Hypertension Risk Factors for Hypertension Age – risk increases with age Genetics – family history, African- American Obesity – 60% of those with hypertension are obese Salt sensitivity Alcohol may raise blood pressure and is associated with strokes.

235
© 2008 Thomson - Wadsworth Hypertension Treatment of Hypertension Weight control is the one of the most effective treatments. Physical activity will help – moderate aerobic for 30-60 minutes most days The DASH Diet – Dietary Approaches to Stop Hypertension

236
© 2008 Thomson - Wadsworth Hypertension The DASH Diet Grains: 6-8 ounces Vegetables: 2-2 ½ cups Fruits: 2-2 ½ cups Milk (low-fat or fat-free): 2-3 cups Meat (lean): 6 ounces or less Nuts, seeds, legumes: 4-5 ounces per week 2000 kcalories
: 2-3 cups Meat (lean): 6 ounces or less Nuts, seeds, legumes: 4-5 ounces per week 2000 kcalories")
237
© 2008 Thomson - Wadsworth Hypertension Treatment of Hypertension Drug Therapy Diuretics and antihypertensive agents Watch potassium

238
© 2008 Thomson - Wadsworth Diabetes Mellitus Diabetes is characterized by high blood glucose (hyperglycemia) and either insufficient insulin, ineffective insulin, or both. Diabetes treatment involves the coordination of diet and/or drugs and physical activity to control blood glucose fluctuations and control or lose weight.

239
© 2008 Thomson - Wadsworth

240
Diabetes Mellitus How Diabetes Develops Impaired glucose tolerance or prediabetes Type 1 Diabetes 5-10% prevalence in diabetic population Autoimmune disorder Usually diagnosed in childhood or adolescence Relatively severe symptoms Associated with viral infection and heredity Insulin is required

241
© 2008 Thomson - Wadsworth Diabetes Mellitus How Diabetes Develops Type 2 Diabetes 90-95% prevalence in diabetic population Occurring in children and adults Relatively moderate symptoms Cells are resistant to insulin Associated with obesity, heredity, and aging Sometimes insulin is required

242
© 2008 Thomson - Wadsworth

243
Diabetes Mellitus Complications of Diabetes Diseases of the Large Blood Vessels Atherosclerosis tends to develop early and is more severe. Long-term, intensive intervention targeting multiple factors can reduce risk. Diseases of the Small Blood Vessels Microangiopathies Affect kidney function and retinal degeneration

244
© 2008 Thomson - Wadsworth Diabetes Mellitus Complications of Diabetes Diseases of the Nerves Hands and feet Careful of injuries and infections Gangrene may develop and amputation may be required.

245
© 2008 Thomson - Wadsworth Diabetes Mellitus Recommendations for Diabetes Total Carbohydrate Intake Consistent intake helps to regulate blood sugar. Too little carbohydrate consumption can lead to hypoglycemia. Carbohydrate Sources Glycemic effect of a food needs to be considered. Avoid foods and beverages with added sugar.

246
© 2008 Thomson - Wadsworth Diabetes Mellitus Recommendations for Diabetes Dietary Fat Saturate fat: <7% of total kcalories Cholesterol: <200 mg/day Protein No need to modify intake as long as there is normal kidney function 15-20% of total kcalories Alcohol Use in Diabetes Alcohol should be used in moderation. One drink/day for women two drinks/day for men

247
© 2008 Thomson - Wadsworth Diabetes Mellitus Recommendations for Diabetes Recommendations for Type 1 Diabetes Adjust insulin doses Optimal nutrition status –Control blood glucose with consistent carbohydrate intake at meals and snacks. –Achieve desirable blood lipids. –Control blood pressure. –Prevent and treat complications. Physical activity –Be careful of hypoglycemia. –Monitor blood glucose.

248
© 2008 Thomson - Wadsworth Diabetes Mellitus Recommendations for Diabetes Recommendations for Type 2 Diabetes Moderate weight loss is helpful (10-20 pounds). Regular, long-term physical activity

249
© 2008 Thomson - Wadsworth Cancer Cancer is the growth of malignant tissue. Dietary factors that initiate cancer development include alcohol and heavily smoked foods. Dietary factors that promote cancer once it has started include saturated fat and trans fat. Dietary factors that serve as antipromoters—that is, protect against the development of cancer—include fiber, antioxidant nutrients, and phytochemicals. Eating a variety of healthful foods and adapting a physically active lifestyle is the best advice to lower cancer risk.

250
© 2008 Thomson - Wadsworth Cancer How Cancer Develops Carcinogenesis is the development of cancer from mutated cells and can result in the formation of an abnormal mass, or tumor. Tumors can metastasize, or spread to other areas of the body. Carcinogens are substance an individual is exposed to that can lead to cancer.

251
© 2008 Thomson - Wadsworth

252
Fig. 18-7, p. 643 Normal cells Mutagens alter the DNA in a cell and induce abnormal cell division. Promoters enhance the development of abnormal cells, resulting in formation of a tumor. The cancerous tumor releases cells into the bloodstream or lymphatic system (metastasis). Malignant cells Normal cells Stepped Art InitiationPromotion Further tumor development
. Malignant cells Normal cells Stepped Art InitiationPromotion Further tumor development.")
253
© 2008 Thomson - Wadsworth Cancer How Cancer Develops Environmental Factors Exposure to radiation and sun, water and air pollution, and smoking are known to cause cancer. Physical activity may protect against certain types of cancer. Obesity increases risk for cancer.

254
© 2008 Thomson - Wadsworth Cancer How Cancer Develops Dietary Factors – Cancer Initiators Additives and pesticides Minimize carcinogens when cooking – use foil on grill, do not burn foods, and marinate meat beforehand Alcohol and smoking High red meat intake and colon cancer Acrylamide is produced when starches are cooked at high temperatures – french fries and potato chips

255
© 2008 Thomson - Wadsworth Cancer How Cancer Develops Dietary Factors – Cancer Promoters High-fat diets correlate with high cancer rates but inconclusive High-kcalorie diets correlate with high cancer rates High-saturated fat and high-trans fat diets correlate with high cancer rates Omega-3 may protect

256
© 2008 Thomson - Wadsworth Cancer How Cancer Develops Dietary Factors – Antipromoters Fruits and vegetables and low incidence of cancer Fiber-rich diets might protect against colon cancer Phytochemicals found in cruciferous vegetables activate enzymes that destroy carcinogens. Antioxidant nutrients are effective – vitamin C, vitamin E, and beta-carotene

257
© 2008 Thomson - Wadsworth Cancer Recommendations for reducing cancer risk Healthy body weight Eat a variety of healthy foods. Five or more cups of fruits and vegetables Limit red meats. Limit consumption of alcoholic beverages. Adopt a physically active lifestyle.

258
© 2008 Thomson - Wadsworth Cancer Classifications of cancers Adenomas – glandular tissues Carcinomas – epithelial tissues Gliomas – glial cells of the central nervous system Leukemias – white blood cells Lymphomas – lymph system Melanomas – pigmented skin cells Sarcomas – muscle, bone or connective tissues

259
© 2008 Thomson - Wadsworth

260
Recommendations for Chronic Diseases Recommendations for the Population Make dietary changes to forestall or prevent disease is the preventive or population approach Recommendations for Individuals Urge dietary changes for people who need them is the medical or individual approach Recommendations for Each Individual Genomics may allow for individual nutritional recommendations.

261
© 2008 Thomson - Wadsworth Complementary and Alternative Medicine

262
© 2008 Thomson - Wadsworth Complementary and Alternative Medicine Alternative therapies come in many different practices and products. Benefits and risks may be great, small or nonexistent. Wise consumers and health care professionals accept the beneficial effects that have been confirmed by research to be safe and effective. They reject those practices that cause harm. Making healthful choices requires understanding and seeking out reliable sources of information.

263
© 2008 Thomson - Wadsworth Defining Complementary and Alternative Medicine Complementary and alternative medicine: diverse medical and health care systems, practices, and products that are not currently considered part of conventional medicine Conventional medicine: diagnosis and treatment of diseases as practiced by medical doctors, doctors of osteopathy, and allied health professionals Integrative medicine is an approach that incorporates alternative therapies into the practice of conventional medicine.

264
© 2008 Thomson - Wadsworth Examples Acupuncture – uses long, thin needles to relieve pain or illness Aroma therapy – uses plant or flower oil extracts to enhance health Ayurveda – uses herbs, diet, meditation, message, and yoga to prevent and treat disease Bioelectromagnetic medical applications – uses electrical or magnetic energy to increase healing Biofeedback – allows individuals to learn how to control body functions

265
© 2008 Thomson - Wadsworth Examples Biofield therapeutics – uses a healing force Cartilage therapy – uses connective tissue to increase health Chelation therapy – removes toxic substances from the body Chiropractic – manipulation of the spine Faith healing – use of divine intervention in healing Herbal medicine – uses plants to treat disease Homeopathy – belief that substances can help relieve symptoms

266
© 2008 Thomson - Wadsworth Examples Hydrotherapy – use of water to heal and relax Hypnotherapy – uses power of suggestion Imagery – guided visual relaxation Iridology – study of the eye and how it is related to disease Macrobiotic diets – a restricted diet of grains and vegetables Massage therapy – manipulation of the muscles to promote healing

267
© 2008 Thomson - Wadsworth Examples Meditation – calming and relaxation of the mind Naturopathic medicine – includes several natural healing practices Orthomolecular medicine – use of large doses of vitamins to treat disease Ozone therapy – use of ozone gas to boost the immune system Qi gong – uses movement, meditation, and breathing to change energy flow in the body

268
© 2008 Thomson - Wadsworth Sound Research, Loud Controversy Little research – folklore, tradition, and testimonials Placebo effect can bring about a healing effect in people who believe they are receiving treatment Risks versus Benefits There are herbal remedies that are safe and reasonably effective. Some therapies are not hazardous or costly but help mood and reduce stress. Some are dangerous, posing great risks. Some are dangerous but have some benefits.

269
© 2008 Thomson - Wadsworth

270
Nutrition-Related Alternative Therapies Foods Potential health benefits of soy in relation to heart disease are documented. More research is needed on phytoestrogens of soy to manage symptoms of menopause Vitamin and Mineral Supplements Research on some vitamins and minerals might be appropriate in preventive care. Safety and effectiveness issues

271
© 2008 Thomson - Wadsworth Nutrition-Related Alternative Therapies Herbal Remedies Used throughout history Benefits Synthesized medicines contain exact doses Herbal preparations can vary from batch to batch

272
© 2008 Thomson - Wadsworth

273
Nutrition-Related Alternative Therapies Herbal Precautions “Natural” does not mean beneficial or safe. Herbs are not drugs; they are dietary supplements. Lack of information and discrepancies True identification of herbs Purity of herbal preparations Appropriate uses and contraindications of herbs Effectiveness of herbs Variability of herbs Accuracy of labels Safe dosages of herbs Interactions of herbs with medicines and other herbs Adverse reactions and toxicity levels of herbs

274
© 2008 Thomson - Wadsworth Internet Precautions Advertising and marketing of their own products Quotations from researchers and physicians may be taken out of context. Increased access to products

275
© 2008 Thomson - Wadsworth The Consumer’s Perspective Seek alternative medicine because it is more in line with their beliefs about health and life Use alternate therapies in addition to conventional therapies Selecting reliable practitioners means checking out training, qualifications and licenses. Keep physicians informed.

Similar presentations
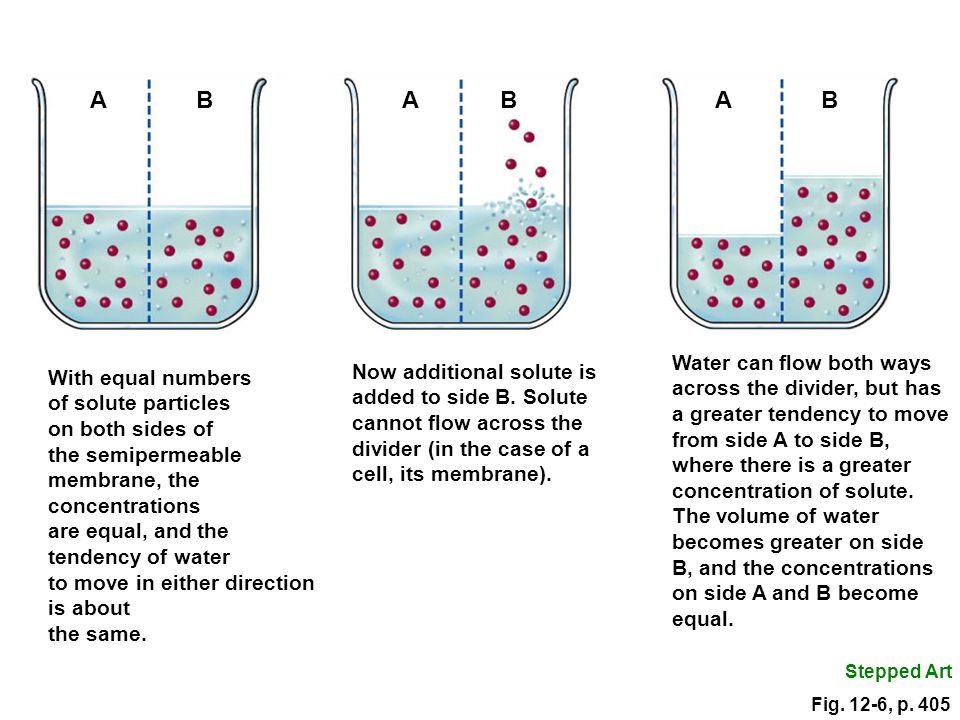


 Potassium (K + )>")











>")




