Download presentation
Presentation is loading. Please wait.

1
Carolyn A. Parry, MPH CDC Public Health Advisor Montana Immunization Program 2016 Regional Immunization Workshops

2
Pneumococcal o Background for the recommendations o Immunization Schedules Childhood Adult High-risk patients o Resources Meningococcal B o Background for the recommendations o Routine and Permissive recommendations o Vaccines

3
2014 National Immunization Survey (NIS) Data Healthy People 2020 objective
 Data Healthy People 2020 objective")
4
2014 Montana Behavioral Risk Factor Surveillance System (BRFSS) Healthy People 2020 objective
 Healthy People 2020 objective")
5
Streptococcus pneumoniae isolated in 1881 More than 80 serotypes described by 1940 Initial interest in developing a vaccine declined with advent of penicillin o Patients were still dying despite antibiotic treatment By 2011, 92 serotypes have been documented o 10 most common cause 62% of invasive disease worldwide Symptoms o Abrupt onset of fever, chills or rigors, chest pain, productive cough, shortness of breath, rapid breathing, rapid heart rate, malaise, weakness *Epidemiology and Prevention of Vaccine-Preventable Diseases, 13 th ed, pages 279-295

6
Pneumococcal pneumonia (lung infection) o 400,000 hospitalizations per year in U.S. o Up to 36% of adult community-acquired o Complication of influenza o Case-fatality rate 5%-7%, higher in elderly

7
Pneumococcal bacteremia (blood infection) o More than 12,000 cases per year in U.S. o Case-fatality rate ~20%; up to 60% among the elderly Pneumococcal meningitis o Pneumococci cause over 50% of all cases of bacterial meningitis in U.S. o Est. 3,000-6,000 cases per year in U.S. o Case-fatality rate 8% among children; 22% among adults

8
Certain conditions that increase risk: o Immunocompromising conditions, including HIV infection o Functional or anatomic asplenia, particularly sickle cell disease o Chronic heart, pulmonary, liver or renal disease (includes asthma in 19+) o Cigarette smoking (19+) o Cerebrospinal fluid leak (CSF) leaks o Cochlear implant o Child care attendance (children) o Alaska native, African American, American Indian (Navajo and White Mountain Apache) (children)
 o Cigarette smoking (19+) o Cerebrospinal fluid leak (CSF) leaks o Cochlear implant o Child care attendance (children) o Alaska native, African American, American Indian (Navajo and White Mountain Apache) (children)")
9
In children age 2 years and younger o Bacteremia without known site of infection - approximately 70% of invasive disease o Bacteremic pneumonia caused 12%-16% of invasive pneumococcal disease In children age 5 years and younger o S. pneumoniae leading cause of bacterial meningitis Pneumococci are a common cause of acute otitis media Before the conjugate vaccine: o children less that 1 year of age had the highest rates of pneumococcal meningitis (10 cases per 100,000) o 17,000 cases of invasive disease each year, 13,000 were bacteremia and 700 meningitis o 200 children died each year as a result of invasive disease o 5 million cases of otitis media
 o 17,000 cases of invasive disease each year, 13,000 were bacteremia and 700 meningitis o 200 children died each year as a result of invasive disease o 5 million cases of otitis media.")
10
In 2011, estimated 35,000 cases and more than 4,200 deaths from invasive disease o More than half these occurred in adults who were recommended to receive the PPSV23 vaccine Data suggests PCV has had an impact on invasive disease in young children o 99% decrease in 7 serotypes o some increases in disease by serotypes not included in PCV7 o In 2008, data indicated approximately 61% of invasive pneumococcal disease in children younger than 5 years due to serotypes included in PCV13 43% caused by serotype 19A (included in PCV13) Indirect effects from PCV13 use in children might effect disease incidence in adults.
 Indirect effects from PCV13 use in children might effect disease incidence in adults.")
11
YearVaccine 197714-valent polysaccharide vaccine licensed (no longer in U.S.) 198323-valent polysaccharide vaccine licensed (PPSV23) 20007-valent polysaccharide conjugate vaccine licensed (PCV7) 201013-valent PCV licensed (PCV13)
 valent polysaccharide vaccine licensed (PPSV23) valent polysaccharide conjugate vaccine licensed (PCV7) valent PCV licensed (PCV13)")
12
Children: Routinely administered PCV13 at 2, 4, 6, and 12-15 months

13
Doses administered before 12 months of age, the minimum spacing between doses is 4 weeks Doses administered on or after 12 months of age, the minimum spacing is 8 weeks

14
Healthy children aged 7-59 months who have not been vaccinated with PCV13 should receive 1-3 doses of PCV13, depending on when vaccination begins. o Infants 7-11 months – 3 doses o Children aged 12-23 months – 2 doses o Children 24 months and older Unvaccinated healthy children – 1 dose Age at first dose# of DosesBooster 7-11 months2 dosesYes 12-23 months2 dosesNo 24-59 months1 doseNo

15
Unvaccinated children 24-71 months with underlying medical conditions – 2 doses, 8 weeks apart o Chronic heart and lung disease o Diabetes o Anatomic or functional asplenia (including sickle cell disease); o Immunocompromising conditions such as HIV-infection, those resulting from disease or treatment of disease o Cochlear implant o Cerebrospinal fluid leak (CSF) leaks
; o Immunocompromising conditions such as HIV-infection, those resulting from disease or treatment of disease o Cochlear implant o Cerebrospinal fluid leak (CSF) leaks")
16
Administer 1 dose of 13-valent pneumococcal conjugate vaccine (PCV13) to children 6 years of age and older who have not received PCV13 previously and are at increased risk: o Anatomic or functional asplenia (including sickle cell disease); o Immunocompromising conditions such as HIV-infection o Cochlear implant; o Cerebrospinal fluid leak (CSF) leaks Administer PCV13 first, wait 8 weeks before administering PPSV23. For 24mo – 18 years: If PPSV23 has been administered, wait 8 weeks before administering PCV13. For 19 years+: If PPSV23 has been administered, wait 1 year before administering PCV13.

17
Children and adults 2 years of age and older with the following conditions should receive PPSV23: o Chronic illness Heart disease, lung disease, diabetes, alcoholism, chronic liver disease, cirrhosis, CSF leaks, cochlear implant o Anatomic or functional asplenia o Immunocompromised o Asthma and cigarette smoking (19 year of age and older)
")
18
A repeat dose at least 5 years after the first dose is recommended for those with: o Anatomic or functional asplenia o Immunocompromising conditions such as HIV-infection, leukemia, lymphoma, Hodgkin disease, multiple myeloma, generalized malignancy, chronic renal failure, nephrotic syndrome, transplant, treatment with immunosuppressive drugs Those receiving a 2 nd dose before 65 years of age should receive a 3 rd dose after 65 years of age (minimum spacing - 5 years).
.")
19
Adults: PCV13 (for PCV13 naïve adults) and PPSV23 are routinely administered to adults 65 years of age and older o PCV13 should be administered first o PPSV23 should be administered 1 year after PCV13
 and PPSV23 are routinely administered to adults 65 years of age and older o PCV13 should be administered first o PPSV23 should be administered 1 year after PCV13")
20
Notes: "For immunocompetent adults who previously received PPSV23 when aged <65 years and for whom an additional dose of PPSV23 is indicated when aged ≥65 years, this subsequent PPSV23 dose should be given ≥1 year after PCV13 and ≥5 years after the most recent dose of PPSV23. For adults aged ≥65 years with immunocompromising conditions, functional or anatomic asplenia, cerebrospinal fluid leaks, or cochlear implants, the recommended interval between PCV13 followed by PPSV23 is ≥8 weeks." Please refer to the footnotes in the respective schedules for further details about pneumococcal vaccination.

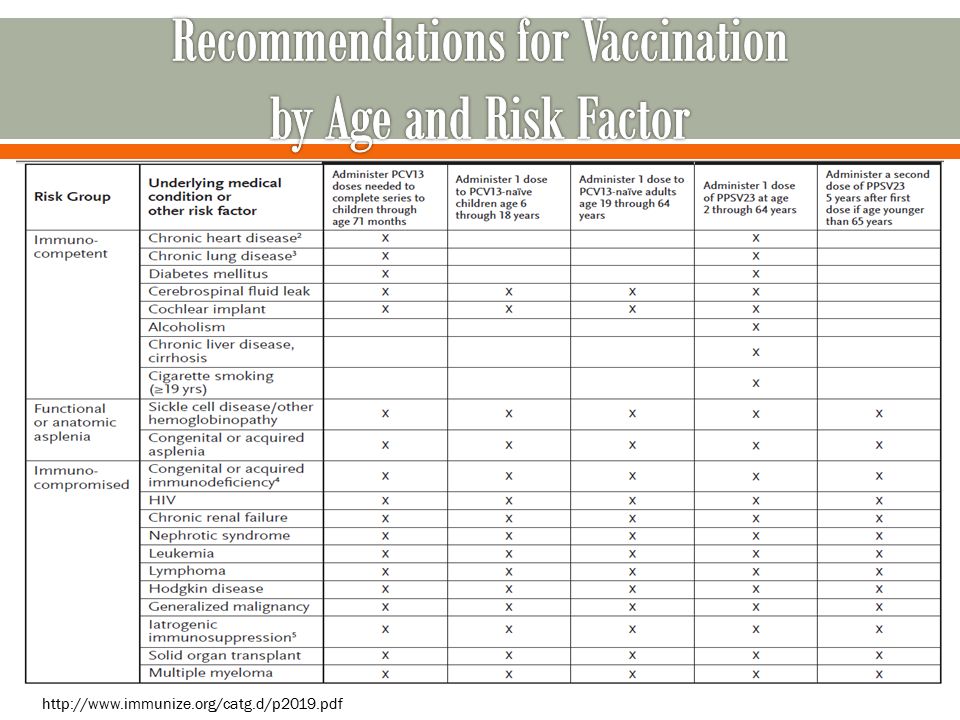
21
http://www.immunize.org/catg.d/p2019.pdf
22
http://www.cdc.gov/vaccines/schedules/downloads/child/job-aids/pneumococcal.pdf

23
Date of Birth – 02/25/2014 PCV #1 – 10/31/2014 PCV #2 – 03/15/2015 When is the next dose due? How many more doses are needed?

24
Date of Birth – 04/10/2013 PCV #1 – 08/13/2014 When is the next dose due? How many more doses are needed?

25
A 16 year old with an immunocompromising condition presents in your clinic. Pneumococcal vaccine is recommended. The adolescent received 4 doses of PCV7 as a child. What should this individual receive and when?

26
A 65 year old who smokes occasionally is in your clinic today for vaccinations. At age 63 years (2 years ago) a PPSV23 was administered. What should this individual receive and when?
 a PPSV23 was administered. What should this individual receive and when .")
27
Meningococcal disease is an acute, potentially severe bacterial illness caused by Neisseria meningitidis. Disease was first reported in the 16 th century Neisseria meningitidis is the leading cause of bacterial meningitis and sepsis in U.S. Epidemic in sub-Saharan Africa Almost all invasive disease is caused by serogroups A, B, C, Y, and W U.S. is experiencing a historic low in meningococcal disease incidence -.18 per 100,000 *Epidemiology and Prevention of Vaccine-Preventable Diseases, 13 th ed, pages 231-245

28
Disease o Abrupt onset of fever, headache, stiff neck, nausea, vomiting, sensitivity to light, confusion, rash o Incubation period is 3 to 4 days, with a range of 2 to 10 days o Case-fatality rate 10%-15% Meningococcal meningitis o Most common presentation of invasive disease Meningococcemia (bloodstream infection) o May occur with or without meningitis o Case-fatality rate up to 40% o Up to 20% of survivors have permanent sequelae including hearing loss, neurologic damage, or loss of limb.
 o May occur with or without meningitis o Case-fatality rate up to 40% o Up to 20% of survivors have permanent sequelae including hearing loss, neurologic damage, or loss of limb.")
29
Certain medical conditions are at highest risk: o Deficiencies in the terminal common complement pathway o Functional or anatomic asplenia o Certain genetic factors Environmental factors o Preceding viral infection o Household crowding o Active and passive smoking o Microbiologists - occupational

30
Annually 50 to 60 cases and 5 to 10 deaths o 80% of these cases occur in 16-23 year olds Since 2009, seven outbreaks have occurred on college campuses resulting in 41 cases and three deaths o 40-70% of cases in 18-23 year olds occur in college students Meningococcal B disease incidence in college students aged 18-23 years -.09 per 100,000 Meningococcal B disease incidence in non-college students aged 18- 23 years-.21 per 100,000

31
Vaccine will protect against most strains of serogroup B No concerning patterns of adverse events following vaccination Data not yet available on effectiveness against clinical disease endpoints or duration of protection Potential impact on carriage and herd protection is inconclusive

32
Considered vaccinating all adolescents o Concluded that vaccinating at 16-18 years would probably provide protection during the highest risk period o Determined insufficient evidence to make a routine recommendation for all adolescents Category and

34
Routine Recommendation: Persons 10 years of age and older who are at increased risk for meningococcal disease should receive Men B vaccine o Persons with persistent complement component deficiencies o Persons with anatomic or functional asplenia o Microbiologists routinely exposed to isolates of Neisseria meningitidis o Persons identified at increased risk because of a serogroup B meningococcal disease outbreak. Permissive Recommendation: One of the Meningococcal B vaccines may be administered to adolescents and young adults aged 16-23 years to provide short term protection against most strains of serogroup B meningococcal disease. The preferred age for vaccination is 16-18 years

35
MenB-4C (Bexsero ® ) Novartis o 2 doses administered at 0 and > 1 month schedule o Licensed in the U.S. on January 23, 2015 MenB-FHbp (Trumenba ™ ) Pfizer o 3 doses administered at 0, 2, 6-month schedule o Licensed in the U.S. on October 29, 2014 The MenB vaccines are not interchangeable.
 Pfizer o 3 doses administered at 0, 2, 6-month schedule o Licensed in the U.S. on October 29, 2014 The MenB vaccines are not interchangeable..")
Similar presentations




>")












 Primary infection results in varicella (chickenpox) Recurrent infection results in herpes zoster (shingles) Short.>")


