Download presentation
Presentation is loading. Please wait.

1
Anna Drinkwater UHNS

5
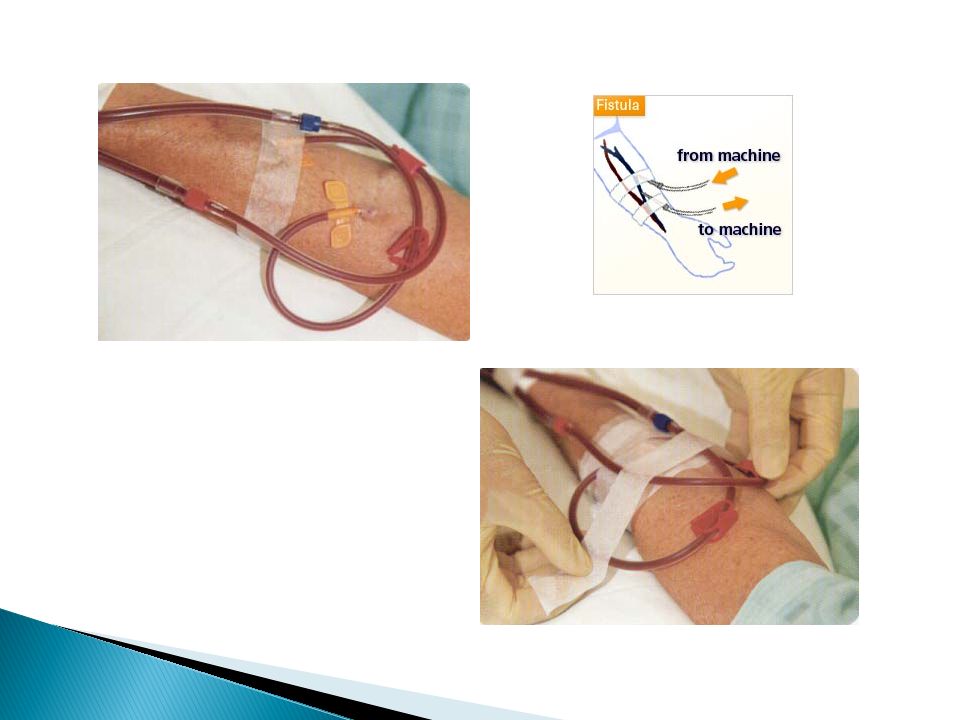
Dialysis at least 3 x weekly Vascular access ◦ 80% HDx patients should dialyse via arteriovenous fistula Serum PO4 <1.8mmol/l BP: Pre HDx systolic <140mmHG diastolic <80mmHG Maintaining Hb 11-12 Renal Association Standards

7
Brachial: ◦ Elbow ◦ 90% success rate ◦ Steal syndrome more common ◦ Not usually done first Radial: ◦ Wrist ◦ 60% success rate ◦ Usually done first

8
Vascular access

9
Usually inserted into jugular vein or femoral Try to avoid subclavian as high risk of venous stenosis Temporary lines limited duration Permanent lines are usually cuffed and tunnelled

13
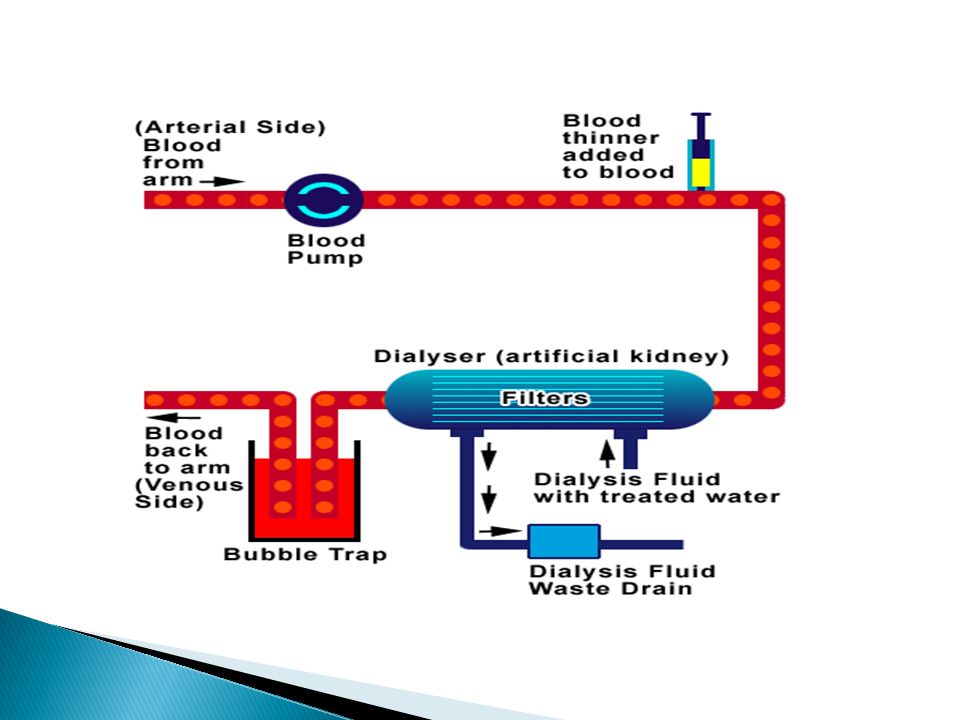
Filtered through a reverse osmosis system to remove aluminium, bacteria and other potential endotoxins Water supplier limits aluminium, calcium, chloramines, nitrates, sodium, sulphates, zinc and copper

14
Heparin Low Molecular Weight Heparin - Clexane Fragmin Innohep Epoprostenol Lepirudin Danaparoid

15
Urea Reduction Ratio (URR) [aim for URR > 65%] Kt/v [aim for Kt/V > 1.2]
![ Urea Reduction Ratio (URR) [aim for URR > 65%] Kt/v [aim for Kt/V > 1.2]](http://images.slideplayer.com/34/10174512/slides/slide_15.jpg " Urea Reduction Ratio (URR) [aim for URR > 65%] Kt/v [aim for Kt/V > 1.2]")
16
K:Urea clearance (per minute) t:Time on dialysis V:How much urea is to be cleared (volume of body water which urea is distributed in)
 t:Time on dialysis V:How much urea is to be cleared (volume of body water which urea is distributed in)")
17
Pre & post weight Blood flow Time on dialysis Size of dialyser Dry weight Pre & post biochemistry & haematology Problems with the dialysis session

18
Kt/V Protein Catabolic Rate Nutritional status Residual Renal Function

19
Higher blood flow rate Increasing the dialysate flow rate Increasing size/surface area of the dialyser Longer time on dialysis Changing from haemodialysis to haemodiafiltration

20
Hypotension Too much fluid being removed too quickly Bolus of NaCl 0.9% Omit BP tabs Reduce rate of fluid removal Stop them eating CrampsHypotension Fluid removal Carnitine deficiency NaCl 0.9% or Glucose 50% Quinine tablets Assess weight Carnitine, Vit E supplements Chest & back pain Complement activation Exclude angina More biocompatible dialyser Paracetamol

21
Pruritis Dry skin High Phosphate Allergic reaction Antihistamines Moisturising lotions Different dialyser Infections Skin penetration usually at fistula or permcath sites Impaired immune response Low threshold for starting anti- staphylococcal agents Anaemia Blood loss, inadequate dialysis, excessive bleeding post dialysis, iron or EPO deficiency EpoIron Reduce heparin dose

22
Air embolism Dysrrhythmias Clotting + blocked lines Haemorrhage

23
First phase euphoria Second phase depressive reaction Third phase realistic adjustment Abram HS (1970) Survival by machine; the psychological stress of chronic haemodialysis. Psychiatric Medicine, 1: 37

24
Anaemia Osteodystrophy Cardiac problems Uraemia

25
May be done in intensive care Much less aggressive than haemodialysis Tends to be done over a longer time e.g. continual Usually a short term treatment in the acute situation Higher removal rate of large molecular weight substances e.g. ß 2 microglobulin and less of small molecular weight ones e.g. Potassium and urea

26
Can remove excess fluid easily to create “space” for e.g. TPN Reduces risk of disequilibrium syndrome Improves patient tolerability i.e. Reduces dialysis symptoms – hypotension, nausea and vomiting, headaches

29
Combination of haemodialysis and Haemofiltration Best treatment option as removes both low and high molecular weight molecules Reduces long term dialysis complications Need ultra pure water High flux dialysers but watch albumin removal

31
The blood is diluted by the substitution fluid before going through the dialyser and was the original form of HDF

32
Advantages ◦ Better tolerated than post-dilution ◦ Less heparin required ◦ Blood less likely to clot in patients with good HB or access problems Disadvantages ◦ Small solute clearance reduced ◦ Reduced 2- microglobulin clearance ◦ Approximately twice as much substitution fluid compared with post dilution HDF is need i.e. Higher dialysate flow rates

33
The more traditional method now: blood is diluted by substitution fluid after going through the dialyser

34
Advantages ◦ Smaller volumes of fluid required ◦ Most efficient as get the best removal of small and large solutes Disadvantages ◦ Good blood flow required ◦ More anticoagulation required ◦ Problems with lines clotting and efficiency if HB too high and blood too viscous ◦ Longer duration of treatment, small molecule clearance not as good

35
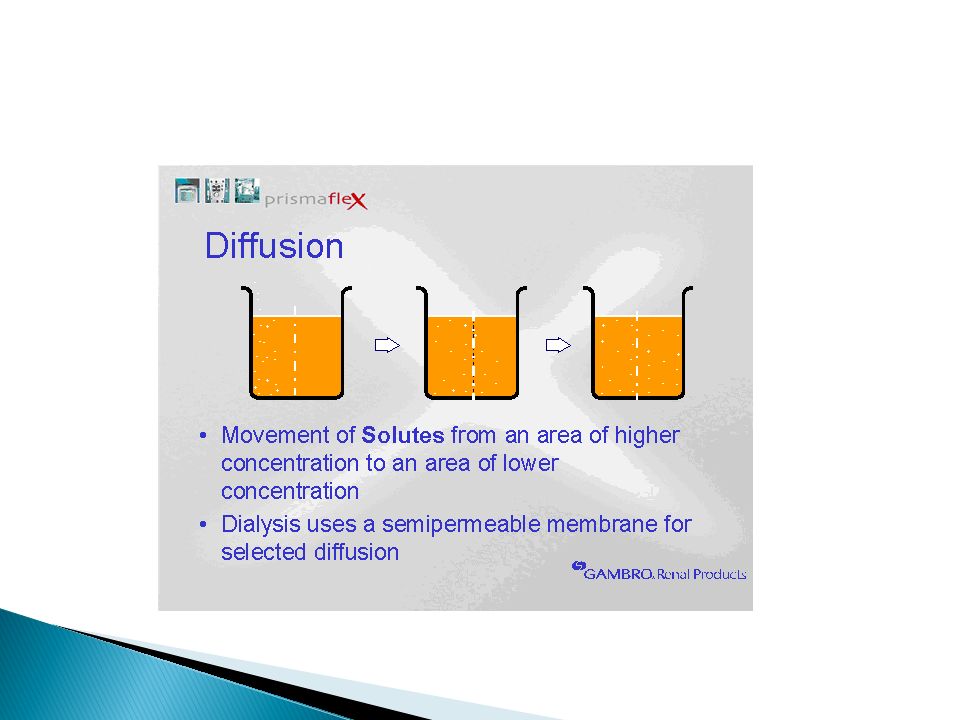
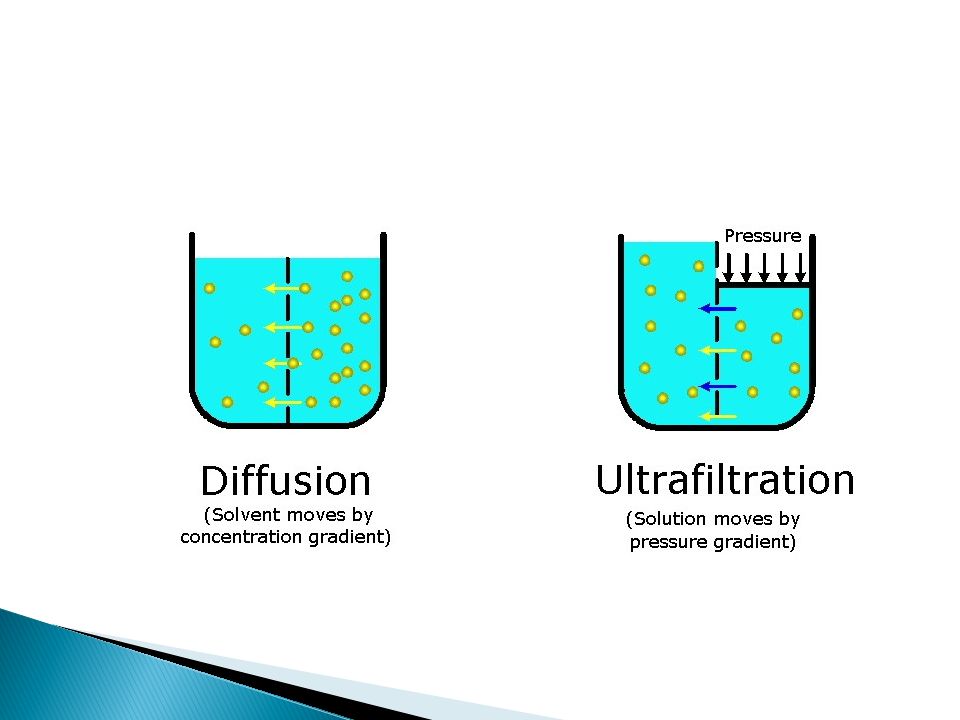
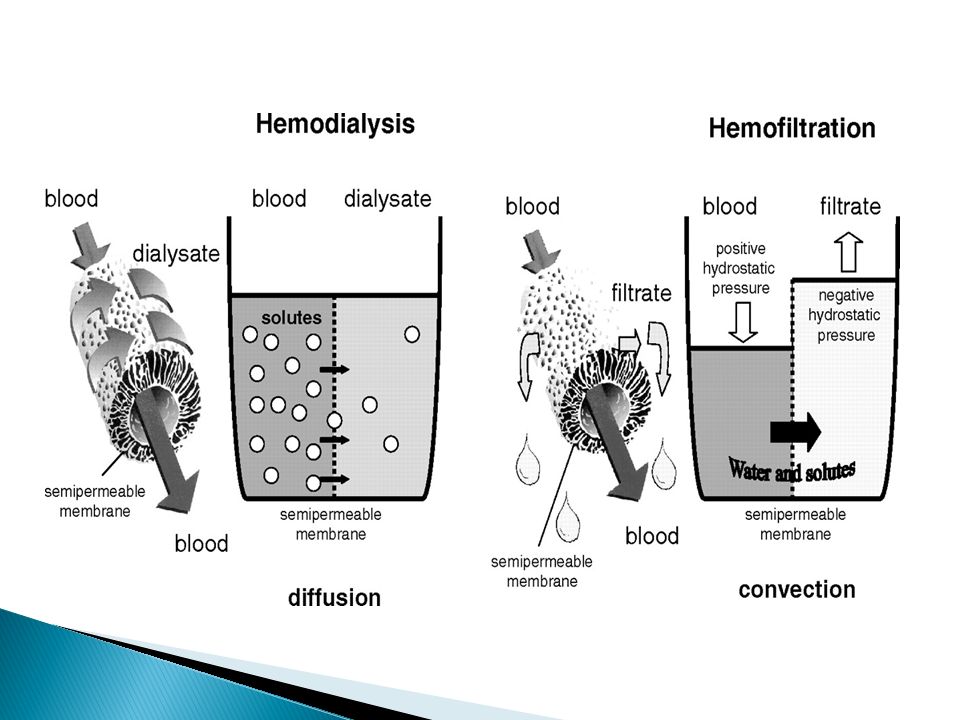
TreatmentMolecular transport AdvantagesDisadvantages HDDiffusion Ultrafiltration Good removal of small solutes Cheapest method Poor removal of middle molecules unless high flux dialyser used HFUltrafiltration Convection Good removal or middle molecules Reduces hypotensive episodes No dedicated water supply or drainage needed Less efficient removal of small molecules Expensive HDFDiffusion Ultrafiltration Convection Good removal of all solutes Good control of hypertension and hypotension Expensive unless on-line

Similar presentations


















.>")




