Download presentation
Presentation is loading. Please wait.

1
Pancreatic Injuries Mamoun Nabri Trauma Fellow 11/24/2009

2
Pancreas – The pancreas was first identified by Herophilus (335-280 BC), a Greek anatomist and surgeon – Hundred years later,, another Greek anatomist, Ruphos, gave the pancreas its name. – The term "pancreas" is derived from the Greek pan, "all", and kreas, "flesh",

3
History 1827:an autopsy report, St Thomas Hospital, London, document the first pancreatic injury, PHBW of Sage coach, complete body transection.

4
History Laborderie in 1856 reported the first penetrating pancreatic injury in the literature. Kulenkampff in 1882 reported a patient that survived blunt injury to the pancreas with the development of a pseudocyst. Kocher, in 1903 described the surgical approach to the mobilization of the duodenum and head of the pancreas 1903: only 45 cases, 21 penetrating, 24 blunt 1905: Korte, pancreatic transection with fistula

5
Introduction Injuries are uncommon, protected deep in retroperitoneal diagnostic dilemma and delay When identified early, treatment is straightforward. Accounts for 10% to 12% of all abdominal injuries. Mortality rates 9%-34%; Morbidity 30%-60% Approximately 50% of the overall mortality due to associated major abdominal vascular injuries.

6
Introduction Major abdominal vascular injuries are present, 75% of cases of penetrating pancreatic trauma Sepsis and multiple organ failure account for most of the late deaths. The incidence of pancreatic-related mortality ranges from 2% to 5% in large urban trauma series. WW I, and in WWII only 62 cases of pancreatic trauma were reported (2% of abdominal injuries) with a 56% mortality Only nine cases of pancreatic injury were reported from the Korean War (22% mortality)
 with a 56% mortality Only nine cases of pancreatic injury were reported from the Korean War (22% mortality).")
7
Pancreas It is a combined endocrine and exocrine gland Divided into head, neck, body and tail Head lies within the curve of the duodenum Uncinate process projects from the head Superior mesenteric vessels separate the head from the body

11
Embryology

13
Blood Supply Two different sources; – Proximal to the 2nd part of the duodenum (forgut), gastroduodenal artery, superior pancreatoduodenal artery. – Distal to this point (the midgut) the arterial supply is from the superior mesenteric artery, inferior pancreatoduodenal artery supplies the 3rd and 4th sections. – The superior and inferior pancreatoduodenal form an anastomotic loop between the celiac trunk and the SMA Venous drainage is into the portal and superior mesenteric vein
 the arterial supply is from the superior mesenteric artery, inferior pancreatoduodenal artery supplies the 3rd and 4th sections. – The superior and inferior pancreatoduodenal form an anastomotic loop between the celiac trunk and the SMA Venous drainage is into the portal and superior mesenteric vein.")
19
Pancreas Pancreatic ducts has two ducts – Main pancreatic duct – Accessory pancreatic duct The main pancreatic duct begins in the tail Drains into the second part of the duodenum together with the common bile duct The main duct is also known as the Duct of Wirsung Accessory duct begins in the head The accessory duct is also known as the Duct of Santorini It usually drains into the main duct but can open separately into the duodenum

21
Histology/Physiology 80 – 90 % of the mass is composed of acinar cells These form the exocrine portion of the gland Secret alkaline juice, amylase, lipase.(1-1.2 L/day) Islets of Langerhans are dispersed within the gland They form islands of endocrine tissue The islets consist of Types A (20%), B (70%) and D (10%) cells – Type A cells produce glucagons – Type B produce insulin – Type D produce somatostatin
 Islets of Langerhans are dispersed within the gland They form islands of endocrine tissue The islets consist of Types A (20%), B (70%) and D (10%) cells – Type A cells produce glucagons – Type B produce insulin – Type D produce somatostatin")
24
Releations Tail extends into the lienorenal ligament along with the splenic artery Anterior relations include transverse mesocolon and stomach Posterior relations include inferior vena cava, aorta, portal vein, common bile duct and left kidney Superior relations include first part of duodenum and splenic artery

27
Posterior view of duodenum/pancreas

29
Associated Injuries 90-95% other injuries Liver 42-32% Spleen 25-40% Stomach 20-40% Major vessel 25-35% Thorax 22-31% Bowel 10-29% CNS 25% Duodenum 18%

30
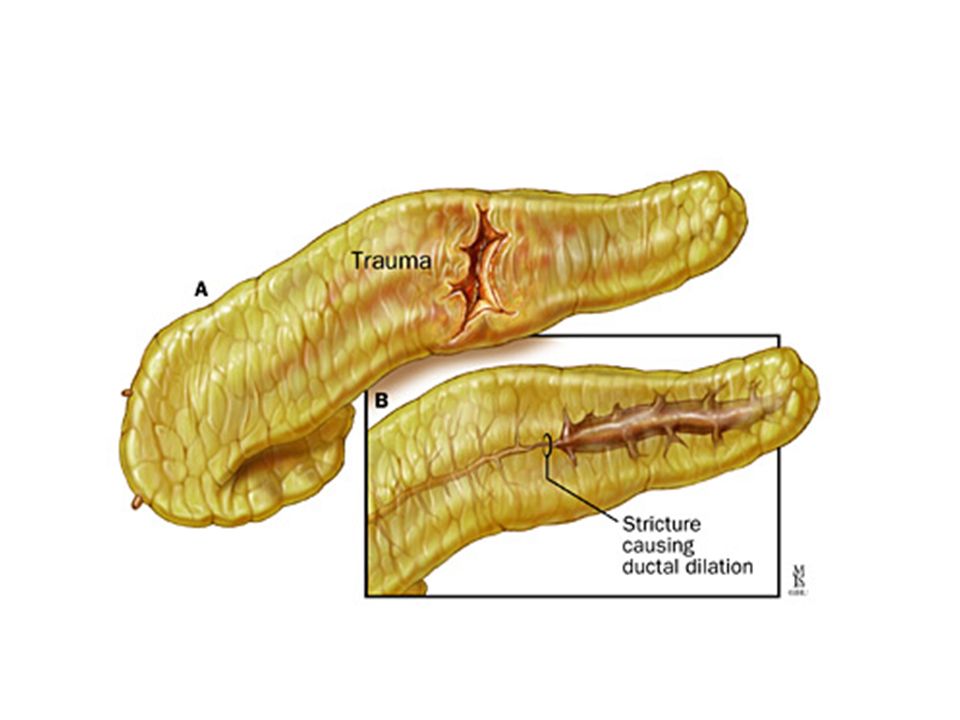
Etiology The great majority of such injuries are caused by penetrating mechanisms and are often associated with significant injuries involving other intra-abdominal organs. Blunt trauma to the abdomen caused by a direct blow or seat belt injury may compress the pancreas over the vertebral column and result in pancreatic disruption

31
Diagnosis Ductal injury, determine outcome High index of suspicion H & PE Mechanism of injury Pancreatic injury can be diagnosed at laparotomy Serum amylase, NPV 95% CT, sensitivity and specifity more than 80% CT ERCP, eval. duct, plan surgery, stents ERCP MR, MRCP, evaluate the duct injury Intraoperative pancreatography

33
Early, irregularity of the neck of the pancreas (arrow), peripancreatic fluid, and intrahepatic hematoma (H).
, peripancreatic fluid, and intrahepatic hematoma (H).")
39
Classification of Injury

41
Surgical Management The primary operative goal of abdominal trauma to control the hemorrhage and gastrointestinal contamination. Proper exposure. Evaluation of pancreas require complete exposure of the gland. Intra-operative pancreatography. Normal endocrine and exocrine function has been reported after 90% pancreatectomy, leave at least 20%.

42
Transection of gastrocoloic ligament, body and tail

43
Kocher maneuver; head and uncinate process

44
Divide peritoneum lateral to spleen and colon; posterior ( Aird’s maneuver)
")
45
60% of pancreatic injuries, minor contusion, hematoma and capsular laceration, Grade I

46
20% of injuries, parenchyma laceration without ductal disruption, Grade II

47
Surgical Management These injuries, grade I & II, require only hemostasis and external drainage Resist temptation to repair capsular laceration External close drainage, for 10 days Nutritional support, elemental diets

49
Distal pancreatic transection, with duct injury, treated with distal pancreatectomy, Grade III

50
Surgical Management Distal pancreatectomy: Grade III – Transected duct, closed U, figure of 8, non- absorbable – Full thickness interlocking U-stitch – TA, stapler – Omental patch – Close suction drainage – Feeding jejunostomy – With or without splenctomy

52
TA Stapler, distal pancreatectomy, ligate splenic vessels

53
Spleen preservation distal pancreatectmy

54
Surgical Management Pancreatic head injury: Grade IV – Define ducal anatomy – Intraoperative pancreatography – Wide external drainage with postoperative ERCP Ductal anatomy not clear Hemodynamically unstability – Patton and colleague, reported, effectiveness of drainage alone for proximal injuries, with 37 patients, only 13.5%, fistula or abscess

55
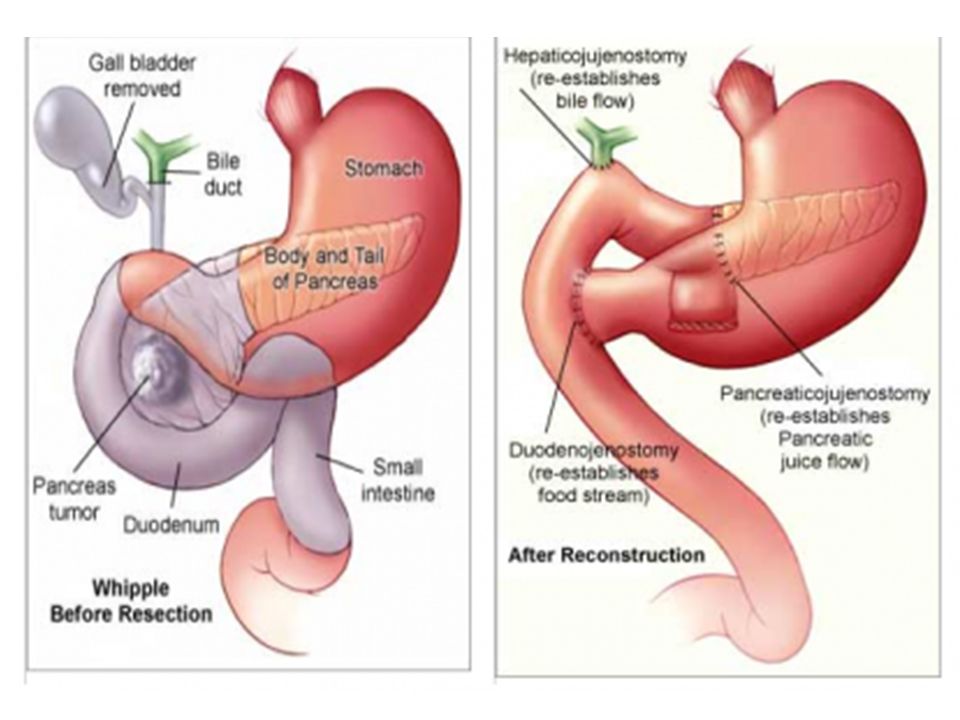
For injuries of the pancreatic head that involve the pancreatic duct but spare the common bile duct, central pancreatic resection with Roux-en-Y pancreaticojejunostomy

56
Surgical Management Combined pancreatic head and duodenal: G V – Rare, caused by penetrating injuries – Determine distal CBD and ampulla integrity, IOC – Associated vascular injuries – Whipple resection remains, the preferred option – Harborview MC, Seattle, 6 years, 10 of 117, underwent Whipple, 4 abscess, 2 pancreatitis, 1 fistula, all 10 patients survived.

59
pancreas duodenum

62
A. Pyloric exclusion is used to treat combined injuries of the duodenum and the head of the pancreas as well as isolated duodenal injuries when the duodenal repair is less than optimal. B and C. The pylorus is over sewn through a gastrotomy, which is subsequently used to create a gastrojejunostomy. The authors frequently use needle-catheter jejunostomy tube feedings for these patients.

63
Complications Most complications are self-limiting and/or treatable Sepsis, MOF: nearly result in 30% of deaths Fistula: most common, incidence 7-20% – < 200ml/d, resolve with adequate drainage – > 700ml/d, external drainage, nutrition – Somatostatin, few data support its use in post- traumatic fistulae

64
Complications Abscess: – 10-25% – Subfascial or peripancreatic – Require drainage, percutaneous or open – The mortality is 25% Pancreatitis: – 8-18% – Usually treated conservatively – Hemorrhagic pancreatitis, occurring in less than 2%

67
Complications Secondary hemorrhage: – 5-10% – Require re-exploration or angioembolization Pseudocyst: – Unrecognized pancreatic injury – Intra-duct, percutaneous drainage – Injured duct, definitive therapy – ERCP before drainage Exocrine, endocrine insufficiency, – uncommon, – only 10-20% of normal pancreatic tissue is needed for normal function

70
Conclusion Traumatic pancreatic injuries are uncommon They are easily missed Attention to details that is required to identify and treat complications Diagnosis require high index of suspicion, pre/intraoperativily, and tests performed in a timely fashion.

71
Whatever happens, don’t loose your head

72
References Current Therapy of Trauma and Surgical Critical Care, Juan A. Asensio, Donald D. Trunkey Trauma, David V. Feliciano, Kenneth L. Mattox, Ernest E. Moore Poole H: Wounds of the pancreas. In Coates JJ, DeBakey M, eds. Surgery in World War II: General Surgery. vol II. Washington DC: Office of Surgeon General, 1955. Culotta R, Howard J, Jordan GJ: Traumatic injuries to the pancreas. Surgery 40:320, 1956. [PubMed: 13352116] PANCREATIC AND DUODENAL INJURIES COMPLEX AND LETHAL, J. A. Asensio, P. Petrone, G. Roldán, R. Pak-art, A. Salim, Scandinavian Journal of Surgery 91: 81–86

73
False Positive

Similar presentations

































.>")














: joins the CBD at ampulla of Vater enters 2 nd part.>")
