Download presentation
Presentation is loading. Please wait.

1
EMS: Obstetric Emergencies Not Deliveries Dan O’Donnell Departments of Emergency Medicine IU School of Medicine

2
Importance You will see these patients daily on runs Stressful situations Treating two patients

3
Case #1 23 y/o pregnant white female with vaginal bleeding x 4 hours.

4
Case 1 Time and Severity Assess length of pregnancy Contributing factors -- Onset and # pads/ hour -- LNMP, fundal height, Ob hx -- Trauma, Abuse, Pain, Clots, Ob complications, Contractions, substance abuse

5
Case 1 VS: RR 20/ HR 120 / BP 90/50 afebrile Cool, Clammy and diaphoretic Prolonged cap refill Pt reports painless vaginal bleeding approx 10 pads/hour. No cramping or Contractions Unsure of dates: LNMP 5 months ago. Fundal height at umbilicus.

6
Treatment High Flow Oxygen Two Large bore IV’s with NS wide open Left Lateral Recumbent Position –if Gestational Age > 20 weeks. Transport Emergently –> 20 weeks gestational age or unstable pt.

7
Why Give Oxygen??? Anemia of Pregnancy –Physiologic Greater increase in plasma volume compared to red cell mass –Fe Deficiency Anemia Subjective Dyspnea –Elevation in Diaphragm Ascends approx. 4 cm –Progesterone-induced hyperventilation Breathing for two

8
Treatment High Flow Oxygen Two Large bore IV’s with NS wide open Left Lateral Recumbent Position –if Gestational Age > 20 weeks. Transport Emergently –> 20 weeks gestational age or unstable

9
Venous Access/Fluid Resuscitation Hard to Quantify Blood Loss Anemia of Pregnancy Hypotension in Mom = Massive Hypotension in Fetus –compensatory mechanisms: vasoconstriction, tachycardia to save mom.

10
Treatment High Flow Oxygen Two Large bore IV’s with NS wide open Left Lateral Recumbent Position –if Gestational Age > 20 weeks. Transport Emergently –> 20 weeks gestational age or unstable

11
Aorta Inferior Vena Cava

12
Left Lateral Recumbent Position Supine Hypotension Syndrome –Gravid Uterus Compressing IVC –Decreased Blood return to heart –Hypotension –More Common once GA > 20 weeks All vitals should be obtained in this position if possible –Trauma pt: Place wedge under right side of board.

13
Estimation of Gestational Age Fundal Height Estimation –12 weeks: top of fundus at symphysis pubis –20 weeks at umbilicus –add 1 week per cm above that. Fetus Viability at 23 weeks

15
Vaginal Bleeding in the Pregnant Patient 1st half of pregnancy 2nd half of pregnancy Postpartum hemorrhage -- Abortion (Most Common), Ectopic Pregnancy, GTD -- Placenta Previa, Abruptio Placenta, Preterm Labor, Bloody show -- Uterine Atony, Uterine Rupture, Retained Placenta Products, Uterine Inversion, Coagulopathy
, Ectopic Pregnancy, GTD -- Placenta Previa, Abruptio Placenta, Preterm Labor, Bloody show -- Uterine Atony, Uterine Rupture, Retained Placenta Products, Uterine Inversion, Coagulopathy")
16
Ectopic Fetus implanted somewhere other than uterus Risk Factors - IUD, PID, previous ectopic, race, infertility tx, smoking, tubal ligation Clinical features - Abdominal Pain, vaginal bleeding, syncope, hypotension Deadly

18
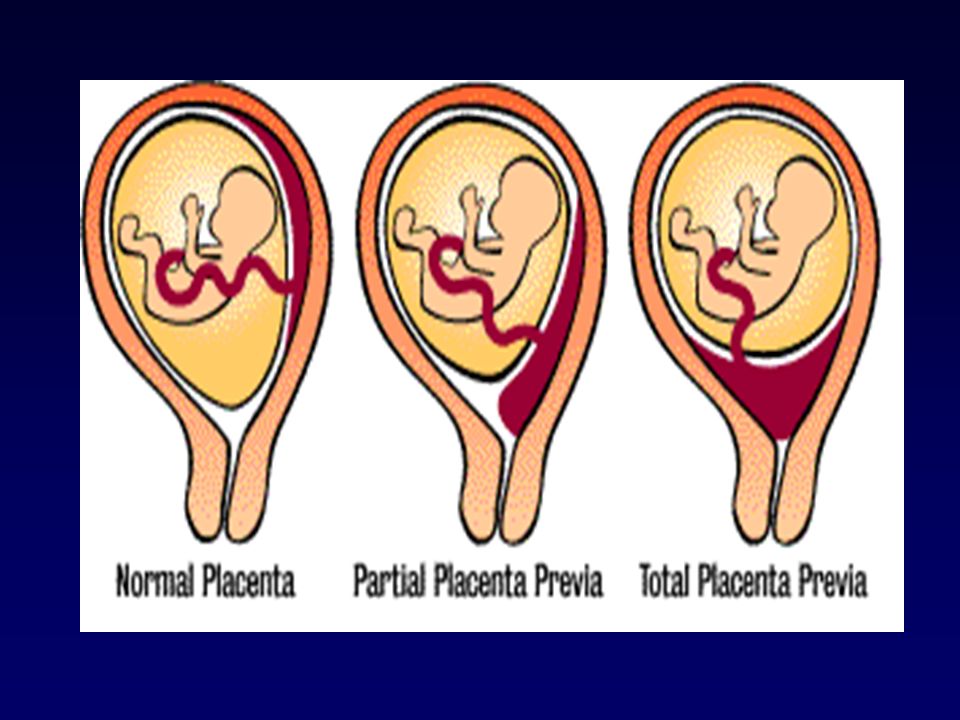
Placenta Previa Painless Bright Red Blood Per Vagina Placenta implantation over cervical os –as cervix shortens, placental vessels tear –Avoid digital or speculum exam Hx may be obtained from patient- increased risk with multiparity and prior c-section

20
Abruptio Placenta Painful, Dark Vaginal Bleeding Premature Separation of Placenta from Uterus Uterine tenderness/contractility

22
Abruptio Placenta Risk Factors –Trauma and hypertension are greatest risks, also increased maternal age, cocaine, smoking, prior history Must also be considered in patients with abdominal pain but no vaginal bleeding High risk to fetus if sufficient compromise to placental blood and oxygen flow

23
Postpartum Hemorrhage Uterine Atony most common cause –lacerations, rupture, retained placenta products Massage the uterus until firm –Check fundus every 5 minutes for firmness and repeat massage as necessary Ask about delivery of Placenta –bring placenta if present

24
Case 2 25 y/o BF in active Labor.

25
Case 2 Due Date Frequency of Contractions Hx of Pregnancies: Preterm or Postterm Sensation of the need to move bowels –delivery imminent Presence of crowning –delivery imminent Rupture of Membranes –Gush of fluid

26
Case 2 VS: RR 20 / HR 110/ BP 110/70 “water has broke but I think I’m way early” Contractions every 5 minutes: painful Fundal Height: few(4-5) cm above umbilicus I feel something coming out………...
 cm above umbilicus I feel something coming out………...")
28
Prolapsed Umbilical Cord Prematurity and Breech are greatest risk factors Umbilical Cord presents before fetus –compression of cord and fetal distress Oxygen and IV

29
Prolapsed Umbilical Cord Place mother in Trendelenburg position Knee to Chest Elevate presenting part off of umbilical cord –Keep elevated until relieved by doctor –never try to replace cord

30
Case 4 Called for a woman who has just given birth Delivery performed by new midwife Upon Arrival patient is pail and the bed is soaked in blood

31
Case 4 Continued P 165, BP 80/p, R 32, SaO 98% on NRB Severe lower abdominal pain and cramping Continuous hemorrhage noted as you move her to the bed

32
Postpartum Hemorrhage Caused by atony of the uterus after placental delivery Can be caused by retained placenta High flow 02 Massage the fundus of the placenta until firm 2 large bore IVs

33
Case 4 21 y/o pregnant BF with complaint of abdominal pain and malaise

34
Case 4 Generalized abdominal pain and blurry vision over the last couple of days No prenatal Care First pregnancy

35
Case 4 VS: RR 20/ BP 160/90 / HR 100 Edema to hands and face Fundal Height above the umbilicus Pt looks very “jittery”

36
Preeclampsia Pregnancy induced hypertension, proteinuria, and pathologic edema ( hands and face, persisting throughout the day) Occurs 20 weeks GA to 2-4 weeks postpartum Risk Factors –Females less than 20, primigravidas, high cholesterol, cigarette smoking, family history, twin or molar pregnancies Only real treatment is delivery
 Occurs 20 weeks GA to 2-4 weeks postpartum Risk Factors –Females less than 20, primigravidas, high cholesterol, cigarette smoking, family history, twin or molar pregnancies Only real treatment is delivery")
37
Preeclampsia O2 and IV Left lateral recumbent position No lights or sirens, darkened ambulance En Route patient begins to have generalized tonic clonic seizure………….

38
Eclampsia Preeclampsia with seizure Warning signs— headache, nausea and vomiting, visual disturbances, MAP > 161, hyperreflexic Routine seizure protocols should be followed –diazepam(Valium) is safe in pregnant pts. –Check blood sugar First line Treatment is Magnesium Sulfate 4-6 grams IV/ 15 minutes.

39
Case 5 26 y/o pregnant female involved in low speed MVA where she was rear-ended Did have mild abdominal pain but now resolved Refusing transport Should we encourage her to seek medical care?

40
Minor Trauma in Pregnancy Even Minor trauma can cause major complications

42
Minor Trauma in Pregnancy Less than 20 weeks –Can do TVUS to test for viability –If there is injury there is little that can be done Greater than 20 weeks –Will admit for 4 hour tocofetal monitoring Rec transport of all pregnant women even with minor trauma –At least OB F/U

43
Take Home Points Left Lateral Recumbent Position Estimate Gestational Age by using Fundal Height Oxygen and Fluids in pregnant patient Recommend transport of all pregnant trauma patients

Similar presentations