Download presentation
Presentation is loading. Please wait.

1
Pulmonary Infections Pneumonia can result whenever these defense mechanisms are impaired or whenever the resistance of the host in general is lowered. – Loss or suppression of the cough reflex – Injury to the mucociliary apparatus – Interference with the phagocytic or bactericidal action of alveolar macrophages

2
Lung defense mechanisms.

3
PNEUMONIA Infection of the lung parenchyma is called pneumonia. It can be of two types. Community acquired Pneumonia Hospital acquired Pneumonia

4
Clinical features Fever with chills Productive cough and pleuritic chest pain

5
Pneumonia Etiological classification – Bacterial pneumonia – Viral pneumonia – Fungal pneumonia – etc. Anatomical classification – Lobar pneumonia – Lobular pneumonia(broncho pneumonia) – Interstitial pneumonia
 – Interstitial pneumonia.")
6
It may present as acute, fulminant clinical disease or as chronic disease with a more protracted course.

7
Community acquired Pneumonia is further divided into Typical and atypical pneumonia Typical pneumonia Intra alvolar exudates are present in typical pneumonia.

8
Community-Acquired Acute Pneumonia Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis Staphylococcus aureus Legionella pneumophila Enterobacteriaceae (Klebsiella pneumoniae) and Pseudomonas spp.
 and Pseudomonas spp.")
9
Streptococcus Pneumoniae The most common cause of community acquired pneumonia Streptococcus Pneumoniae.(50 to 70%) The presence of numerous neutrophils suggest the pneumococcal organsim and lancet shaped diplococci supports the diagnosis. Pneumococcal pneumonias respond readily to penicillin treatment.

10
Pneumococcal infections occur with increased frequency in three subsets of patients: (1) those with underlying chronic diseases such as CHF, COPD, or diabetes;
 those with underlying chronic diseases such as CHF, COPD, or diabetes;")
11
(2) those with either congenital or acquired immunoglobulin defects, acquired immune deficiency syndrome [AIDS]);
![(2) those with either congenital or acquired immunoglobulin defects, acquired immune deficiency syndrome [AIDS]);](http://images.slideplayer.com/33/10106723/slides/slide_11.jpg "(2) those with either congenital or acquired immunoglobulin defects, acquired immune deficiency syndrome [AIDS]);")
12
(3) those with decreased or absent splenic function sickle cell disease or after splenectomy
 those with decreased or absent splenic function sickle cell disease or after splenectomy")
13
Haemophilus Influenza pneumonia in children, In Adults with chronic pulmonary diseases such as chronic bronchitis, cystic fibrosis, and bronchiectasis. H. influenzae is the most common bacterial cause of acute exacerbation of COPD. Moraxella catarrhalis In the elderly people. It is the second most common bacterial cause of acute exacerbation of COPD.

14
Staphylococcus aureus in children and healthy adults after viral respiratory illnesses. Staphylococcal pneumonia is associated with a high incidence of complications, lung abscess and Empyema.

15
Pseudomonas pneumonia neutropenic, usually secondary to chemotherapy extensive burns; in patients requiring mechanical ventilation. Pseudomonas bacteremia is a fulminant disease,with death often occurring within a matter of days.

16
numerous neutrophils fill the alveoli acute bronchopneumonia in a patient with a high fever. Pseudomonas aeruginosa. Note the dilated capillaries in the alveolar walls from vasodilation with the acute inflammatory process.

17
Klebsiella pneumoniae K. pneumoniae is the most frequent cause of gramnegative bacterial pneumonia. Klebsiella- pneumonia frequently afflicts - debilitated, - malnourished persons, particularly chronic alcoholics.

18
Legionella pneumonia Transmission is either inhalation of aerosolized organisms or aspiration of contaminated drinking water. In patients with cardiac, renal, immunologic, hematologic disease. Organ transplant recipients are particularly susceptible.

19
Chronic Pneumonia Nocardia Actinomyces Granulomatous: Mycobacterium tuberculosis and atypical mycobacteria, Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatitidis Necrotizing Pneumonia and Lung Abscess Anaerobic bacteria (extremely common), with or without mixed aerobic infection S. aureus, K. pneumoniae, Streptococcus pyogenes, and type 3 pneumococcus (uncommon )
.")
20
Pneumonia in the Immunocompromised Host Cytomegalovirus Pneumocystis jiroveci Mycobacterium avium complex (MAC) Invasive aspergillosis Invasive candidiasis “Usual” bacterial, viral, and fungal organisms
 Invasive aspergillosis Invasive candidiasis Usual bacterial, viral, and fungal organisms")
21
Nosocomial Pneumonia Nosocomial, or hospital-acquired, pneumonias are defined as pulmonary infections acquired in the course of a hospital stay. high-risk group on mechanical ventilation ventilator-associated pneumonia. Gram- negative rods (Enterobacteriaceae (Klebsiella spp Serratia marcescens, Escherichia coli and Pseudomonas spp, S. aureus (usually methicillin-resistant)
.")
22
Aspiration Pneumonia Aspiration pneumonia occurs in markedly debilitated patients or who aspirate gastric contents either while unconscious (e.g., after a stroke) or during repeated vomiting. Abscess formation is a common complication Anaerobic oral flora (Bacteroides, Prevotella, Fusobacterium, Peptostreptococcus), admixed with aerobic bacteria (S. pneumoniae, S. aureus, H. influenzae, and Pseudomonas aeruginosa)
, admixed with aerobic bacteria (S. pneumoniae, S. aureus, H. influenzae, and Pseudomonas aeruginosa).")
23
Atypical pneumonia It is an acute febrile respiratory disease characterized by patchy inflammatory changes in the lungs, It is usually caused by the extracellular organsims. Inflammtion of the the alveolar septa and pulmonary interstitium. Absence of intraalveolar exudate, Mostly lymphocytic infiltration moderate amounts of sputum, absence of physical findings of consolidation, moderate elevation of white cell count, and lack of alveolar exudates.

24
Community-Acquired Atypical Pneumonia Most common Mycoplasma pneumoniae Chlamydia spp.—Chlamydia pneumoniae, Chlamydia psittaci, Chlamydia trachomatis--Newborns Coxiella burnetii (Q fever) Viruses: respiratory syncytial virus, human metapneumovirus, parainfluenza virus (children); influenza A and B (adults); Adenovirus (military recruits)
 Viruses: respiratory syncytial virus, human metapneumovirus, parainfluenza virus (children); influenza A and B (adults); Adenovirus (military recruits)")
25
Morphology Macroscopically, the affected areas are red-blue, congested, and subcrepitant. Histologically the inflammatory reaction is confined to the alveoliar walls. The septa are widened and edematous; they usually contain a mononuclear inflammatory infiltrate of lymphocytes, histiocytes, and, occasionally, plasma cells. free of cellular exudate.

26
Clinical features fever, headache, and malaise and, later, cough with minimal sputum. severe upper respiratory tract infection or "chest cold Treatment- macrolide antibiotic effective against Mycoplasma and Chlamydia pneumoniae,

27
Lobular Pneumonia or Bronchopneumonia Bronchopneumonia Patch consolidation in the lobe of lung Usually bilateral basal - due to gravitation of secretions. Affects extremes of age (Infants or old) Chest X-rays shows patchy opacification of the lobe.
 Chest X-rays shows patchy opacification of the lobe..")
28
Morphology Gross appearance- Consolidated areas of acute suppurative inflammation Patchy,Slightly elevated, dry, granular, gray-red to yellow, and poorly delimited at their margins Pleural involvement is less common than in lobar pneumonia. Histologically – Focal suppurative exudate that fills the bronchi, bronchioles, and adjacent alveolar spaces.

29
The cut surface of this lung demonstrates the typical appearance of a bronchopneumonia with areas of tan-yellow consolidation. Remaining lung is dark red because of marked pulmonary Congestion..

30
This radiograph demonstrates patchy infiltrates consistent with a bronchopneumonia from a bacterial infection

31
Bronchopneumonia. Gross section of lung showing patches of consolidation (arrows).
.")
32
At higher magnification, the pattern of patchy distribution of a bronchopneumonia is seen. The consolidated areas here very closely match the pattern of lung lobules (hence the term "lobular" pneumonia).
..")
33
pneumococcal pneumonia pneumococcal pneumonia evolved through four stages: congestion, red hepatization, gray hepatization, and resolution.

34
Stage of Congestion The lung is heavy, boggy, and red. It is characterized by vascular engorgement, intra-alveolar fluid with few neutrophils, and often the presence of numerous bacteria. Stage of Red Hepatization Massive confluent exudation with red cells (congestion), neutrophils, and fibrin filling the alveolar spaces. The lobe now appears distinctly red, firm, and airless, with a liver-like consistency,hence the term hepatization.
, neutrophils, and fibrin filling the alveolar spaces. The lobe now appears distinctly red, firm, and airless, with a liver-like consistency,hence the term hepatization..")
35
Stage of Gray Hepatization Progressive disintegration of red cells. The persistence of a fibrinosuppurative exudate. The gross appearance – A grayish brown, dry surface Lobar pneumonia-gray hepatization, gross photograph. The lowerl obe is uniformly Consolidated.

36
Stage of Resolution The consolidated exudate within the alveolar spaces undergoes progressive enzymatic digestion to produce a granular, semifluid, debris that is resorbed, ingested by macrophages, coughed up, or organized by fibroblasts growing into it.

37
At the left the alveoli are filled with a neutrophilic exudate that corresponds to the areas of consolidation seen grossly with the bronchopneumonia

38
Pyemic lung abscess in the center of section with complete destruction of underlying parenchyma within the focus of involvement.

39
The PMN's seen here are in alveoli, indicative of an acute bronchopneumonia of the lung. The PMN's form an exudate in the alveoli. This patient had a "productive“ cough because large amounts of purulent sputum were produced. The source, the neutrophilic alveolar exudate, is seen here.

40
There is a localized foreign body giant cell response to the aspirated material seen here at high magnification. Aspirated material may also produce inflammation from chemical irritation, as with gastric contents

41
Complications Abscess formation – tissue destruction and necrosis - Empyema – Suppurative material may accumulate in the pleural cavity - Fibrosis – Organization of the intra-alveolar exudate - Bacterial dissemination --Meningitis, arthritis, or infective endocarditis

42
Lobar Pneumonia The contiguous airspaces of part or all of a lobe are homogeneously filled with an exudate that can be visualized on radiographs as a lobar or segmental consolidation. Streptococcus pneumoniae is responsible for more than 90% of lobar pneumonias

43
Pathogenesis >90% S. pneumoniae The sudden onset Fibrinous exudates Morphology Four stages of the inflammatory response – Congestion – Red hepatization – Gray hepatization – Resolution

44
Chest x-ray demonstrating complete right upper lobe consolidation, consistent with a lobar pneumonia.

46
A, Acute pneumonia. The congested septal capillaries and extensive neutrophil exudation into alveoli corresponds to early red hepatization. Fibrin nets have not yet formed. B, Early organization of intra-alveolar exudate, seen in areas to be streaming through the pores of Kohn (arrow). C, Advanced organizing pneumonia (corresponding to gray hepatization), featuring transformation of exudates to fibromyxoid masses richly infiltrated by macrophages and fibroblasts.
. C, Advanced organizing pneumonia (corresponding to gray hepatization), featuring transformation of exudates to fibromyxoid masses richly infiltrated by macrophages and fibroblasts..")
47
Complications Carnification – Organization of intra alveolar fibrinous exudates instead of resorption may convert areas of the lung into solid fibrous tissue. Tissue destruction and necrosis Fibrinous or fibrinopurulent pleuritis

48
Seen here are two lung abscesses, one in the upper lobe and one in the lower lobe of this left lung. An abscess is a complication of severe pneumonia, most typically from virulent organisms such as S. aureus. Abscesses are complications of aspiration, where they appear more frequently in the right posterior lung.

49
Comparison of bronchopneumonia and lobar pneumonia.

51
Lab investigations Gram stain Examination of gram- stained sputum The presence of numerous neutrophils containing the typical gram-positive, lancet- shaped diplococci. Blood cultures is more specific.

52
Hypostatic pneumonia – The patient with pulmonary edema from cardiac failure or heavy uremia, et al, is particularly vulnerable.

53
Chronic pneumonia Chronic pneumonia most often is a localized lesion in an immunocompetent person, with or without regional lymph node involvement. There is typically granulomatous inflammation, which may be due to bacteria (e.g., M.tuberculosis) or fungi.
 or fungi..")
54
In immunocompromised patients, Pulmonary Infections debilitating illness, on immunosuppressiveregimens, with human immunodeficiency virus (HIV)
")
55
Influenza Infections The influenza virus is a single-stranded RNA virus, Influenza virus type—A, B, or C. The type A viruses infect humans, pigs, horses, and birds and are the major cause of pandemic and epidemic influenza infections

56
A particular subtype of avian influenza— “bird flu,” caused by strain H5N1—has caused massive outbreaks in domesticated poultry in parts of Southeast Asia. Influenza Virus Type A/H1N1 Infection In March 2009, a novel swine-origin influenza A virus, strain H1N1, was identified, which spread in the United States and worldwide, leading to a pandemic affecting more than half a million patients, with more than 6200 deaths by November 2009.

57
SARS 1 st appeared in China in 2002. Causative agent-Corona virus. Clinical features-fever,myalgia,malasie,dry cough. In some patients resolves but in some cases develop severe respiratory infection and failure.

58
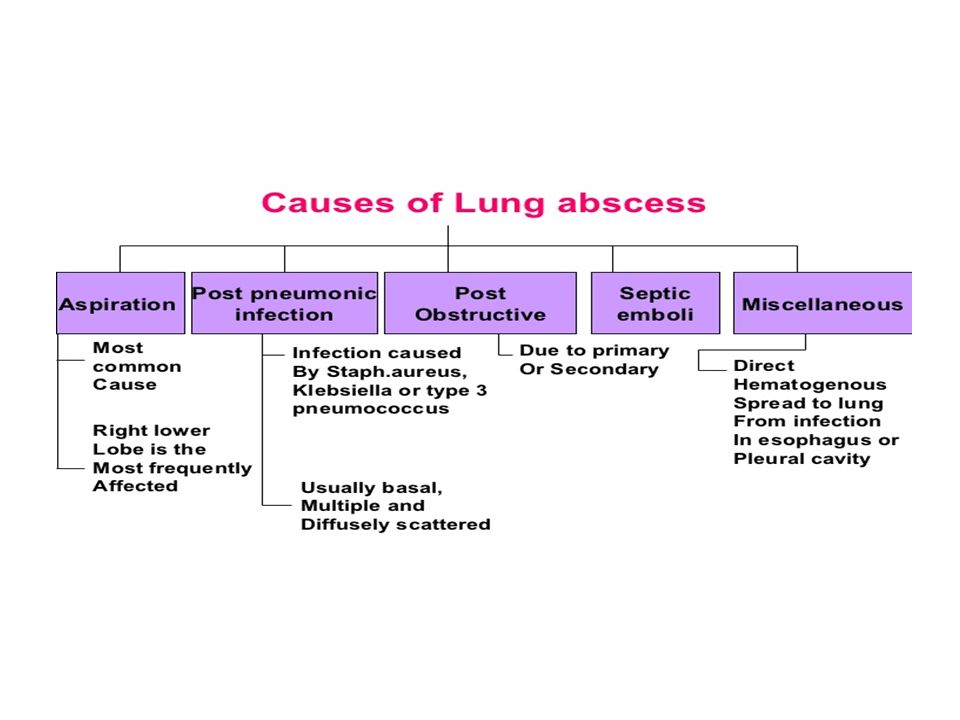
Lung Abscess Lung abscess is a localized area of suppurative necrosis within the pulmonary parenchyma, resulting in the formation of one or more large cavities.

60
From Aspiration of infective material carious teeth infected sinuses or tonsils, during oral surgery, anesthesia, coma, alcoholic intoxication and in debilitated patients with depressed cough reflexes. Aspiration of gastric contents, usually accompanied by infectious organisms from the oropharynx. complication of necrotizing bacterial pneumonias S. aureus, Streptococcus pyogenes, K. pneumoniae, Pseudomonas spp., and, rarely, type 3 pneumococci.

61
Mycotic infections and bronchiectasis Septic embolism hematogenous spread of bacteria in disseminated pyo.genic infection

62
Clinical features fever, productive cough with large amount of sputum, chest pain, weight loss and presence of clubbing of the fingers and toes. Characteristic histologic feature: Suppurative destruction of lung parenchyma within the central area of cavitation. Complication include empyema, brain abscess or meningitis, pulmonary hemorrhage and secondary amyloidosis.

63
TUBERCULOSIS (KOCH’S DISEASE) Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. – mycolic acid in its cell wall making it acid fast.

65
Increased risk of tuberculosis diabetes mellitus, Hodgkin’s lymphoma, chronic lung disease (particularly siliocosis), chronic renal failure, Malnutrition, alcoholism and immunosuppression.
, chronic renal failure, Malnutrition, alcoholism and immunosuppression.")
66
Infection is the presence of organisms, which may or may not cause clinically significant disease. In most of the people, primary tuberculosis is asymptomatic. Infection with M. tuberculosis typically leads to the development of delayed hypersensitivity to M. tuberculosis antigens, which can be detected by the tuberculin (Mantoux) test.
 test..")
67
A positive tuberculin test(PPD) result signifies cell-mediated hypersensitivity to tubercular antigens. It is a screening test. (Cannot specify whether it is active or inactive disease process)
.")
68
False- negative Mantoux test – Sarcoidosis – Malnutrition – Hodgkin disease – Immunosuppression – Fulminant tuberculosis False-positive Mantoux test – infection by atypical mycobacteria – Previous vaccination with BCG

69
Pathogenesis – Macrophages are the primary cells infected by M.tuberculosis. – The bacteria enter macrophages by endocytosis. – The bacterial cell wall glycolipid a protien cord factor blocks the fusion of the phagosome and lysosome. This is followed by bacterial multiplication inside the macrophages.

70
The initial stages of primary tuberculosis (<3 weeks) in a no sensitized individual is characterized by bacterial multiplication in the pulmonary alveolar macrophages and airspaces, with resulting bacteremia and spread to multiple sites in the body.
 in a no sensitized individual is characterized by bacterial multiplication in the pulmonary alveolar macrophages and airspaces, with resulting bacteremia and spread to multiple sites in the body.")
71
After about 3 weeks of infection, TH1 cells are stimulated by mycobacterial antigens, become mature TH1 cells by the action of IL-12.

72
The mature TH1 cells in the lymph nodes and lungs produce IFN- which stimulates formation of phagolysosome in infected macrophages and causes nitric oxide induced oxidative damage to the cell wall and DNA of the mycobacteria.

73
Activated macrophages, stimulated by IFN- produce TNF Recruit macrophages “epithelioid histiocytes”, a characteristic feature of granulomatous inflammation..

74
Clinical Features Primary tuberculosis Develops in a previously unexposed and un sensitized individual. The source of the organism is usually exogenous. The majority of the patient with primary tuberculosis develop latent disease while a minority develops progressive infection.

75
Primary tuberculosis Begins in the lungs Site-lower part of the upper lobe or the upper part of the lower lobe due to most of the inspired air being distributed here and form a subpleural lesion. Ghon foci-Caseous necrosis in the periphery.

76
This subpleural lesion along with the draining lymphatics and the lymph nodes is called as Ghon’s complex. During the first few weeks, there is also lymphatic and hematogenous dissemination to other part of the body. In majority of the people, development of cell-mediated immunity control the infection. The Gohn’s complex undergoes progressive fibrosis and calcification (detected radiologically and called as Ranke complex)
.")
77
Secondary tuberculosis Secondary tuberculosis is the pattern of disease that arises in a previously sensitized host. It usually result from a reactivation of latent primary lesion after many yrs of an initial infection, particularly when host immunity is decreased or uncommonly may follow primary tuberculosis. Secondary pulmonary tuberculosis is classically localized to the apex of the upper lobes of the lung (right lung affected more commonly as compared to left) because of high oxygen tension in the apices.
 because of high oxygen tension in the apices..")
79
The preexistence of hypersensitivity contributes to an immediate and marked tissue response leading to localization of the infection (the regional lymph nodes are less prominently involved in secondary tuberculosis) and cavitation followed by erosion into an airway (leading to spread of bacilli during coughing).
 and cavitation followed by erosion into an airway (leading to spread of bacilli during coughing).")
80
Histologically, the active lesion show characteristic tubercles composed of epithelioid cells and Langhans cells with central caseation. The lesion of secondary pulmonary tuberculosis may heal with fibrosis either by itself or after therapy, or it my progress along the following several different pathways

81
Progressive pulmonary tuberculosis is elderly and immunosuppressed individuals. The apical lesion enlarges with increase in the area of caseation. The erosion of blood vessels bronchial artery hemoptysis.. The pleural cavity is associated with pleural effusion or empyema.

82
Miliary disease occurs when organism drain through lymphatics and blood vessels to the different organs of the body resulting in small yellow- white consolidated lesion Miliary tuberculosis is most prominent in the liver, bone marrow spleen, adrenal, meninges, kidneys, fallopian, and epididymis.

83
Note: the most frequent form of extra- pulmonary tuberculosis is lymphadenitis usually in the carvical region and is knows as “ scrofula”. When the vertebrae are affected it is known as pott’s disease. Pott's Disease Abscess

84
Clinical features low grade remittent fever, night sweats, productive cough, weight loss, hemoptysis, dyspnea and pleural effusion. Investigations lymphocytosis and Increased ESR chest X-ray-- hilar lymphadenopathy and pleural effusion, Sputum or gastric lavage contents for Acid fast bacilli with Ziehl Nielson staining.

85
Treatment Isoniazid+Ripampicin+pyrazinamide Multidrug resistance (MDR), defined as resistance of mycobacteria to two or more of the primary drugs used for treatment of tuberculosis, is now seen more commonly.
, defined as resistance of mycobacteria to two or more of the primary drugs used for treatment of tuberculosis, is now seen more commonly.")
Similar presentations









 Environmental.>")






, and the parenchyma.>")



, calor (heat), tumor (swelling), dolor (pain), and loss of function.>")

