Download presentation
Presentation is loading. Please wait.

1
Preventing and Treating Emotional Abuse:
Getting it Right from the Start Jane Barlow Professor of Public Health in the Early Years

2
Structure of paper Emotional Abuse – what is it?
Why are the early years so important? What characterises ‘high risk’ parents? What should we be doing…?

3
What is emotional abuse?
A constant, repeated pattern of parental behaviour, (unaccompanied by physical abuse, sexual abuse or necessarily by physical neglect) that is likely to be interpreted by a child that she or he is unloved, unwanted, serves only instrumental purposes, and/or which severely undermines children’s development and socialisation
 that is likely to be interpreted by a child that she or he is unloved, unwanted, serves only instrumental purposes, and/or which severely undermines children’s development and socialisation.")
4
Emotional Abuse – the problem
Referrals for primary emotional abuse rose from 4,700 (13%) to 5,100 (20%) over past decade This equates to 4.7 per 10,000 children As many as 80% of children registered for physical abuse and neglect have also experienced emotional abuse
 to 5,100 (20%) over past decade. This equates to 4.7 per 10,000 children. As many as 80% of children registered for physical abuse and neglect have also experienced emotional abuse.")
5
Subjective Perceptions
Large-scale population-based study (involving 2,869 adults) in the UK 6% reported - frequent and severe psychological control and domination; - psycho/physical control and domination, humiliation, attacks on self-esteem - withdrawal of their primary carer’s attention/affection - antipathy, terrorising or threatening behaviours and proxy attacks
 in the UK. 6% reported. - frequent and severe psychological control and domination; - psycho/physical control and domination, humiliation, attacks on self-esteem. - withdrawal of their primary carer’s attention/affection. - antipathy, terrorising or threatening behaviours and proxy attacks.")
6
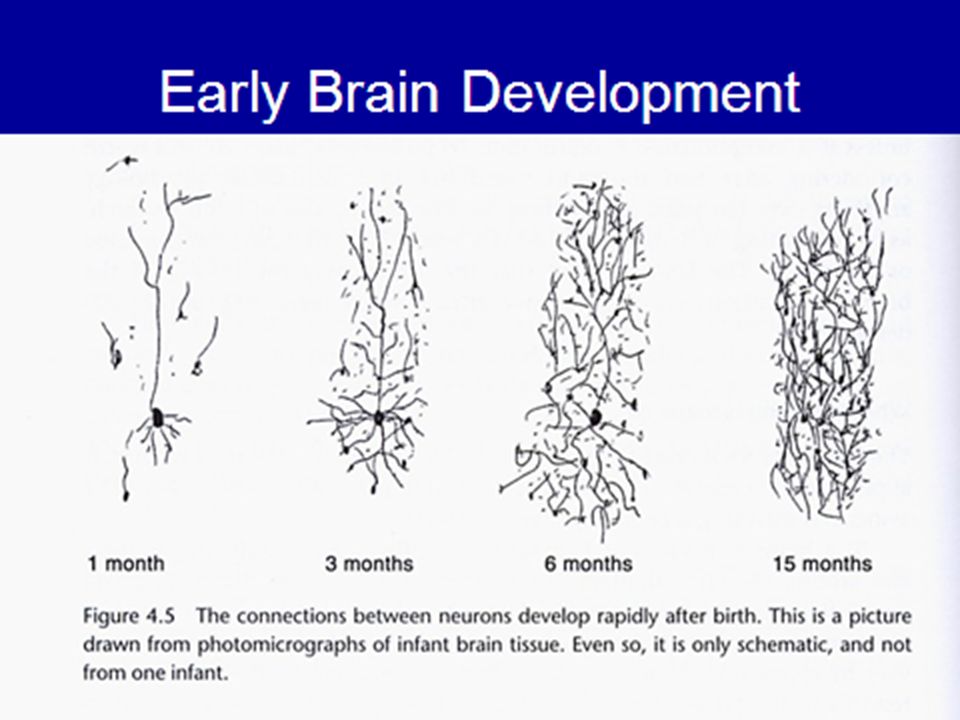
The first three years – why are they SO important?

7
Sensitised nervous system as brain adapts to emotional environment
Trauma in infancy: attachment system compromised Sensitised nervous system as brain adapts to emotional environment Stress in child reminders & experiences of trauma, life events, etc. Unbearably painful emotional states Retreat: isolation dissociation depression Self-destructive actions: substance abuse eating disorders deliberate self-harm suicidal actions Destructive actions: aggression violence rage (Robin Balbernie 2011)
")
8
Aspects of Early Development
Emotional/ social development Intellectual Development Behavioural development Infancy Trust/attachment Alertness/curiosity Impulse control Toddlerhood Empathy Communication/ mastery motivation Coping Childhood Social Relationships Reasoning/problem solving Goal-directed behaviour Adolescence Supportive social network Learning ability/achievement Social responsibility AFFECT REGULATION

11
The Social Baby In first 15 hours baby’s distinguish the voice, smell and face of their mother They connect what they do with what happens immediately after Babies have a sophisticated understanding of facial expressions – distinguish between surprise, fear, sadness, anger and delight By 10- months babies seek emotional information from others to help them interpret things around them By 10-months baby’s brain has developed according to the type of emotions to which they have been exposed (Beebe and Lachman, 2004)
")
12
Important aspects of early parenting
Sensitivity/attunement and contingent interaction Reflective function

13
Contingent Interaction

14
Contingent Interaction
By two months the mothers face is the primary source of visuo-affective communication Face-to-face interactions emerge which are high arousing, affect-laden and expose infants to high levels of cognitive and social information and stimulation To regulate this infant and mothers regulate the intensity of these interactions – ‘affect synchrony’ and repairs to ruptures Absolutely fundamental to healthy emotional development – prolonged negative states are ‘toxic’ to infants 14

15
‘Attuned mutual co-ordination between mother and infant occurs when the infant’s squeal of delight is matched by the mother’s excited clapping and sparkling eyes. The baby then becomes overstimulated, arches its back and looks away from the mother. A disruption has occurred and there is a mis-coordination: the mother, still excited, is leaning forward, while the baby, now serious, pulls away. However, the mother then picks up the cue and begins the repair: she stops laughing and, with a little sigh, quietens down. The baby comes back and makes eye contact again. Mother and baby gently smile. They are back in sync again, in attunement with each other (Fosha, 2003 in Walker 2008, p. 6).
..")
16
Reflective Function

17
Reflective Function Capacity to understand the infant’s behaviour in terms of internal states/feelings A key determinant of self-organization which is acquired in the context of the child's early social relationships (Fonagy, 1997) Development of self-organization is dependent on the caregiver's ability to communicate understanding of the child's intentional stance via ‘marked mirroring’ Lack of parental RF plays a key role in pathological functioning
 Development of self-organization is dependent on the caregiver s ability to communicate understanding of the child s intentional stance via ‘marked mirroring’ Lack of parental RF plays a key role in pathological functioning.")
18
Videoclip 1 .

19
Attachment What is it:? What is its function?:
- Affective bond between infant and caregiver (Bowlby, 1969) What is its function?: - Dyadic regulation of infant emotion and arousal (Sroufe, 1996) Antecedants of attachment: Sensitive, emotionally responsive care during first year – secure attachment Insensitive, inconsistent or unresponsive care – insecure/disorganised attachment
 What is its function : - Dyadic regulation of infant emotion and arousal (Sroufe, 1996) Antecedants of attachment: Sensitive, emotionally responsive care during first year – secure attachment. Insensitive, inconsistent or unresponsive care – insecure/disorganised attachment.")
20
Who is securely attached?
Secure (Group B) – able to use caregiver as a secure base in times of stress and to obtain comfort (55-65%) Insecure Anxious/resistant (Group C) – up-regulates in times of stress to maintain closeness (8-10%) Avoidant (Group A) - down-regulates in times of stress to maintain closeness (10-15%) Disorganised (Group D) – unable to establish a regular behavioural strategy (up to 15% in population sample; 80% in abused sample) (Carlson, Cicchetti et al 1989) 20
 – able to use caregiver as a secure base in times of stress and to obtain comfort (55-65%) Insecure. Anxious/resistant (Group C) – up-regulates in times of stress to maintain closeness (8-10%) Avoidant (Group A) - down-regulates in times of stress to maintain closeness (10-15%) Disorganised (Group D) – unable to establish a regular behavioural strategy (up to 15% in population sample; 80% in abused sample) (Carlson, Cicchetti et al 1989) 20.")
21
Child abuse and attachment
Up to 80% of children who are abused have a ‘disorganised attachment’ In maltreating families parent-child interactions characterised by hostility; low levels of reciprocity, engagement and synchrony, unpredictability (ignoring plus intrusive hostility) Disorganised attachment predicts very poor outcomes including a range of social and cognitive difficulties, and psychopathology Safeguarding practitioners MUST have this developmental model at the core of their practice 21
 Disorganised attachment predicts very poor outcomes including a range of social and cognitive difficulties, and psychopathology. Safeguarding practitioners MUST have this developmental model at the core of their practice. 21.")
22
Disorganised/Controlling Attachment
Caregivers – unpredictable and rejecting; source of comfort also source of distress Self represented as unlovable, unworthy, capable of causing others to become angry, violent and uncaring Others – frightening, dangerous, unavailable Predominant feelings – fear and anger Little time for exploration or social learning

23
Arousal in traumatic attachments
Hyper-arousal (aggression, impulsive behaviour, children emotional and behavioural problems – ‘Fight or flight’ response) Window Of Tolerance Hypo-arousal (dissociation, depression, self harm etc)
 Window. Of. Tolerance. Hypo-arousal (dissociation, depression, self harm etc)")
24
Compulsive Strategies
Compulsive compliance (where parent is threatening) – watchful; vigilant and compliant Compulsive caregiving (where parent is needy) – role reversal; parentification; children deny own developmental needs Coercive – combination of threatening and placatory behaviours Controlling strategies (abusive and neglectful) – self is strong and powerful but also dangerous and bad; avoidance and aggression; completely ‘out of control’ and ‘fearless’
 – watchful; vigilant and compliant. Compulsive caregiving (where parent is needy) – role reversal; parentification; children deny own developmental needs. Coercive – combination of threatening and placatory behaviours. Controlling strategies (abusive and neglectful) – self is strong and powerful but also dangerous and bad; avoidance and aggression; completely ‘out of control’ and ‘fearless’")
25
Compulsive caregiving
‘Caroline is 18 months old. She lives with her mother, who is chronically depressed. The mother describes the household as ‘noxious to the soul’. She cannot tolerate the idea that her depression is affecting Caroline. She says: “Caroline is the only one who makes me laugh.” It is observed that Caroline silently enacts the role of a clown. She disappears into her room and comes out wearing increasingly more preposterous costumes. Caroline makes her mother laugh, but she herself never laughs…’ (Howe, 1999) .’
 .’")
26
Vulnerable Parents

27
Affect synchrony in the face of parental problems
Infant’s emotional states can trigger profound discomfort in the parent (e.g. where there is unresolved loss/trauma, mental health problems, drug/alcohol abuse, or where there is domestic violence etc) Interaction becomes characterized by: - withdrawal, distancing or neglect (i.e. omission) - intrusion in the form of blaming, shaming, punishing and attacking (i.e. commission)
 Interaction becomes characterized by: - withdrawal, distancing or neglect (i.e. omission) - intrusion in the form of blaming, shaming, punishing and attacking (i.e. commission)")
28
Unresolved/disorganised parents
Unresolved loss; abuse; or trauma and in ‘continuing state of fear’ Fr-Behaviour - frightened and frightening; hostile and helpless Atypical Maternal Behaviors – affective communication errors; disorientation; negative-intrusive behaviours; 53% of parents with unresolved states of mind had infants classified as disorganized (van IJzendoorn, 1995) .
 .")
29
Videoclip – Severely suboptimal M-I interaction
.

30
Getting it right first time…
Identify high risk families during pregnancy – pre-birth assessments; Ideally intervention is offered ante-natally - FNP Assess parent-infant interaction Provide time-limited EB intervention and clear goals to be achieved; re-assess interaction Remove infants where there is insufficient improvement before 6 months ideally, end of first year at worst

31
Standardised Scales PIR-GAS – Parent Infant Relationship Global Assessment Scale (Zero to Three 1994) KIPS – Keys to Interactive Parenting Scale NCAST – Nursing Child Assessment Satellite Training (Kelly and Barnard 2000; Barnard 1994) ADBS - Alarm Distress Baby Scale (Guedeney and Fermanian 2001) CARE-Index (Crittenden 1984) PIRAT - Parent-Infant Relational Assessment Tool (Broughton 2010) EAS - Emotional Availability Scales (Biringen 2010)
 ADBS - Alarm Distress Baby Scale (Guedeney and Fermanian 2001) CARE-Index (Crittenden 1984) PIRAT - Parent-Infant Relational Assessment Tool (Broughton 2010) EAS - Emotional Availability Scales (Biringen 2010)")
32
Evidence-Based Interventions
Sensitivity/attachment-based: Interaction Guidance; FNP Psychotherapeutic: Parent-infant psychotherapy Parenting programmes – Parents under Pressure; Parent-Child Interaction Therapy Mentalisation: Minding the Baby

33
Commonalities ‘Dyadic’ - focus on parent-child interaction with emphasis on the child’s attachment; parental sensitivity; parental reflective function etc Underpinned by a clear mechanism for change Emphasis on relationship between therapist/provider and parent

34
Video-Interaction Guidance
Practitioners videotapes parent-infant interactions and shares Video jointly reviewed by practitioner and parent using micro-moments of successful contact with the aim of reflecting on strengths in the parent’s ability to attune Reflective discussion involves support and information about how to enhance their relationship with their child as well as activating the parent to reflect on their child and themselves and their relationship.

35
Evidence Video feedback interventions effective improving parenting behaviour; parenting attitudes; and children’s behaviour (Fukkink 2008) Includes children of all ages VIG effective in reducing disorganised attachment in abused children (Moss et al 2011)
")
36
Parent-Infant Psychotherapy
Watch, Wait and Wonder (Cohen et al 2001) Infant led parent-infant psychotherapy Mother observes her infant’s self-initiated activity whilst being physically accessible to infant Discussion of these experiences with therapist as a way of examining the mother’s internal working models of herself in relation to her infant
 Infant led parent-infant psychotherapy. Mother observes her infant’s self-initiated activity whilst being physically accessible to infant. Discussion of these experiences with therapist as a way of examining the mother’s internal working models of herself in relation to her infant.")
37
Evidence of Effectiveness
Evidence from rigorous studies highlighting the benefits of parent-child psychotherapy for: - children exposed to severely compromised or traumatising (e.g. DV) environments (Lieberman et al 2008; 2004; - parents who are emotionally abusive (Cicchetti et al 2006) or who have major depressive disorder (Toth et al 2006); - preliminary clinical studies have also examined the value of this approach with parents with Borderline Personality Disorder (Newman & Stevenson 2008)
 environments (Lieberman et al 2008; 2004; - parents who are emotionally abusive (Cicchetti et al 2006) or who have major depressive disorder (Toth et al 2006); - preliminary clinical studies have also examined the value of this approach with parents with Borderline Personality Disorder (Newman & Stevenson 2008)")
38
PUP Programme PUP comprises an intensive, manualized, home-based intervention of ten modules conducted in the family home over 10 to 12 weeks, each session lasting between one and two hours PUP is underpinned by an ecological model of child development and targets multiple domains of family functioning, including the psychological functioning of individuals in the family, parent–child relationships, and social contextual factors. Incorporates ‘mindfulness’ skills that are aimed at improving parental affect regulation;

39
PUP evaluation Parents Under Pressure
RCT with substance abusing parents of children aged 2-8 years (Dawe and Harnett 2007) Compared PUP with standard parenting programme Significant reductions in parental stress; methadone dose and child abuse potential (significant worsening in the child abuse potential of parents receiving standard care); improved child behaviour problems
 Compared PUP with standard parenting programme. Significant reductions in parental stress; methadone dose and child abuse potential (significant worsening in the child abuse potential of parents receiving standard care); improved child behaviour problems.")
40
Parent-Child Interaction Therapy
PCIT is a short-term, parent training programme Based on both attachment and social learning theory It is directed at families with 2- to 6-yr-old children experiencing behavioral, emotional, or family problems Rigorous research evidence about its effectiveness with physically abusive parents (Hakman et al 2009; Chaffin et al2004)
")
41
Manualised programme; assessment driven (i. e
Manualised programme; assessment driven (i.e. parents have mastered the skills) not time-limited; Two phases – Child Directed Interaction (CDI); Parent Directed Interaction (PDI) Emphasis throughout on interaction between parent and child; CDI concentrates on strengthening parent-child attachment as a foundation for PDI, which emphasizes a structured and consistent approach to discipline
 not time-limited; Two phases – Child Directed Interaction (CDI); Parent Directed Interaction (PDI) Emphasis throughout on interaction between parent and child; CDI concentrates on strengthening parent-child attachment as a foundation for PDI, which emphasizes a structured and consistent approach to discipline.")
42
Mentalisation-based approaches
Emerging model of intervention that builds on both parent-infant psychotherapy and recent advances in advances in attachment theory Minding the Baby is an interdisciplinary, relationship based home visiting program for young, at-risk new mothers Delivered by a team that includes a nurse practitioner and clinical social worker- uses a mentalisation-based approach that involves working with mothers and babies in a variety of ways to develop mothers' reflective capacities It aims at addressing relationship disruptions that stem from mothers' early trauma and derailed attachment history Only case-study evidence available (Slade et al., 2005)
")
43
Summary Importance of identifying high risk families and conducting pre-birth assessment Intervention should begin ante-natally if possible; Post-natal assessment should include parent-infant interaction Time-limited intervention with clear goals A range of evidence-based universal and targeted interventions to support parent-child interaction;

44
Publications Barlow J, Scott J (2010). Safeguarding in the 21st Century: Where to Now? Dartington: Research in Practice. Barlow J, Schrader-McMillan A (2010). Safeguarding Children from Emotional Abuse: What Works? London: Jessica Kingsley.
. Safeguarding Children from Emotional Abuse: What Works London: Jessica Kingsley.")
Similar presentations