Download presentation
Presentation is loading. Please wait.

1
Foot and ankle Common injuries

2
Squeamish? Roll/twisted ankle: Breaking ankle:
Breaking ankle: Kevin Ware

3
Bones injuries S&S Pain Decreased ROM Swelling Bruising NWB
Obvious deformity

4
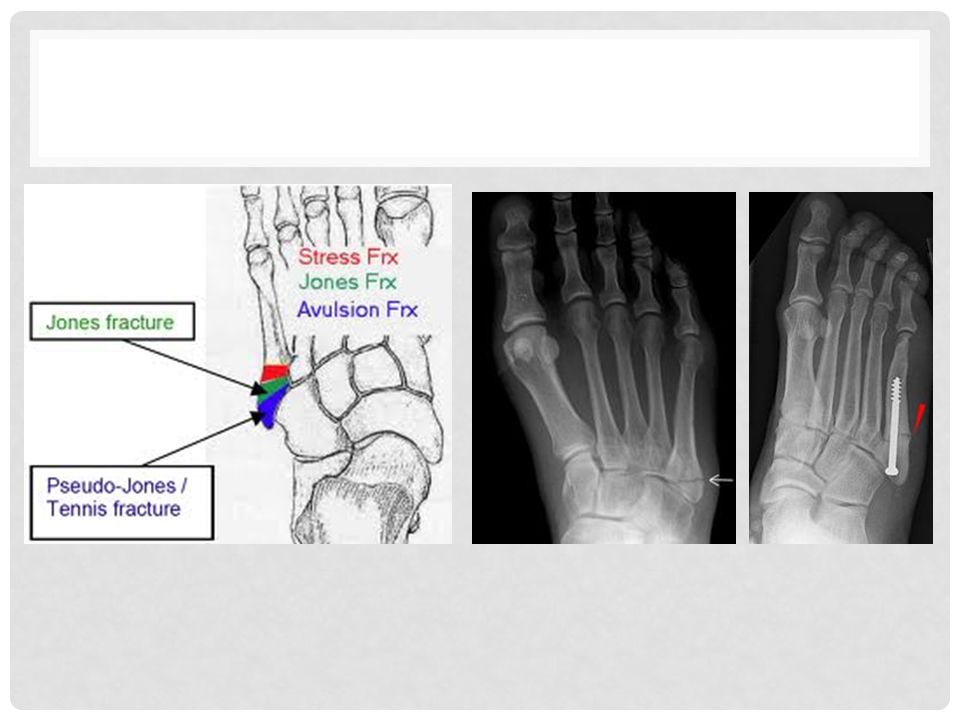
Any bone Epiphyseal Fx Jones Fx Acute fx Stress fx Avulsion fx
Fx to the growth plate (typically tib/fib) Plantarflexion and inversion Serious – potentially stunt growth Jones Fx Avulsion fx of the styloid process of the 5th Metatarsal Forcefull muscle contraction w/ ankle inversion Union vs non-union
 Plantarflexion and inversion. Serious – potentially stunt growth. Jones Fx. Avulsion fx of the styloid process of the 5th Metatarsal. Forcefull muscle contraction w/ ankle inversion. Union vs non-union.")
6
Non-Union

7
Knock-off Fx Stress Fx Fx to lateral malleolus
Forced dorsiflexion & inversion Stress Fx Most commonly tib/fib and MT Reptative stress (usually from running) Pain becomes more intense at night and following activity Usually diagnosed with bone scan
 Pain becomes more intense at night and following activity. Usually diagnosed with bone scan.")
8
Knock-off fx Bi-malleolar fx

9
Bone Scan

10
Grading system Ligament: bone to bone Tendon: muscle to bone
1+/-: stretched, but no tearing/fraying of fibers 2+/-: tearing, but incomplete 3: complete tear

11
Cont’d Signs & Symptoms: Pain Swelling Decreased ROM
Increased temp of skin Bruising NWB + laxity test

12
Ligament/tendon injuires
ATFL– Most commonly sprained MOI – “rolling ankle”, stepping in hole Accounts for 85% Deltoid Ligament Keep ankle from evertion; stronger than ATF MOI – Stepping in hole High Ankle Sprain – Syndesmotic Sprain MOI - Dorsiflexion and evertion Accounts for 15% Achilles Tendon Tendinitis/Rupture More commonly torn with age MOI – Forced Dorsiflexion with knee bent

13
Great-Toe Sprain Arch Sprain Plantar Faciitis Forced Flexion/Extension
“Turf Toe” Arch Sprain Repetative stress, running on hard surface, or improper footwear Pain with running and swelling over affected arch Plantar Faciitis Inflammation of the thick connective tissue

15
Muscle Injuries Strain Common muscles affected: Grade 1, 2, 3
Peroneals Calf Tibialis Anterior

16
“shin Splints” If left un-treated can cause: Caused by:
Medial tibial stress syndrome (MTSS) Irritated and swollen muscles, often from overuse, ramping up workout intensity, changing the surface, improper/old footwear Caused by: Over-pronation or ''flat feet" -- when the impact of a step makes your foot's arch collapses If left un-treated can cause: Stress fractures, which are tiny breaks in the lower leg bones
 Irritated and swollen muscles, often from overuse, ramping up workout intensity, changing the surface, improper/old footwear. Caused by: Over-pronation or flat feet -- when the impact of a step makes your foot s arch collapses. If left un-treated can cause: Stress fractures, which are tiny breaks in the lower leg bones.")
17
Tx: Rest your body. It needs time to heal.
Ice your shin to ease pain and swelling. Do it for 20’ every 3 to 4 hours for 2 to 3 days, or until the pain is gone. Anti-inflammatory painkillers. NSAIDs Arch supports for your shoes. Orthotics -- which can be custom-made or bought off the shelf -- may help with flat feet. Range-of-motion exercises Neoprene sleeve for support. Physical therapy to strengthen the muscles in your shins.

18
You know it’s healed when..
Your injured leg is as flexible as your other leg. Your injured leg feels as strong as your other leg. Your can jog, sprint, and jump without pain. Your X-rays are normal or show healed stress fx. There's no way to say exactly when your shin splints will go away. It depends on what's causing them. People also heal at different rates; 3 to 6 months is not unusual.

19
Misc Injuries Ankle dislocation Contusion Toe Abnormalities
Hammertoe Middle Phalanyx flexed while Distal and Proximal are hyperextended Ingrown Toenail Nail grows into surrounding soft tissue often result of poor trimming May need to be surgically excised

20
Diagnosis Process HOPS: History Observation
Palpation – Provides a reference for the comparison of bilateral symmetry of bones, alignment, tissue temperature, or other deformity as well as the presence of increased tenderness Joint and Muscle Functional Assessment – impairment due to ROM, Strength, P with movement Joint Stability Tests – reference for laxity, gapping, hypo/hypermobility, end-feel Special Test

21
Manual Muscle Testing Patient position: Muscle tested must be against gravity Examiner position: stabilize proximal to the joint being tested and provide resistance to the distal joint “Break test” Positive test: weakness and/or pain compared contralateral

22
Grading 5/5 Normal: can resist max pressure with no pain
4/5 Good: can resist moderate pressure 3/5 Fair: Can move body part against gravity thru full ROM 2/5 poor: Can move body part in gravity-eliminated position thru full ROM 1/5 Trace: cannot produce movement, but muscle contraction is palpable 0/5 Zero: No contraction is felt

23
End-Feel (Normal) Soft: soft tissue approximation (ex: knee flexion)
Firm: Muscular stretch/Capsular Stretch/Ligamentous Stretch (ex: MCP extension) Hard: bone to bone ex: Elbow ext
 Hard: bone to bone ex: Elbow ext.")
24
End-feel (pathological)
Soft: occurs sooner or later in ROM than normal in a joint that normally has a firm or hard end-feel ex: edema/synovitis Firm: occurs sooner or later in ROM than normal in a joint that normally has soft or hard end-feel ex: Capsular/muscular/ligamentous shortening Hard: occurs sooner or later in ROM than normal in a joint that normally has soft or firm end-feel; feels like a bony block ex: Loose bodies in joint/myositis ossificans/fx Spasm: Joint motion is stopped involuntarily or voluntary muscle spasm ex: inflammation/strain/joint instability Empty: no end-feel bc end of ROM is never reached; no resistance felt (except for patient’s protective muscle splinting or muscle spams called “muscle guarding”)
")
25
Homework Pages 4 and 5 in coloring packet

Similar presentations