Download presentation
Presentation is loading. Please wait.

1
Jessie Stewart Morning Report July 09
VENOUS INSUFFICIENCY Jessie Stewart Morning Report July 09

2
Vasodilatory Edema Biggest culprit drugs are arteriolar smooth muscle relaxers. Minoxidil (7%): opens K channels, preventing smooth muscle contraction. Hydralazine (?%): prevents Ca accumulation, may protect nitric oxide.
: opens K channels, preventing smooth muscle contraction. Hydralazine ( %): prevents Ca accumulation, may protect nitric oxide.")
3
CCB also guilty Amlodipine (2-15%, dose related). Blocks calcium transport. NEJM Volume 341: November 4, Calcium-Antagonist Drugs. Darrell R. Abernethy, M.D., Ph.D., and Janice B. Schwartz, M.D.

4
Vasodilatory edema caused by:
1. Increased intracapillary pressure. 2. Activation of the Renin-Angiotensin System Can diminish edema by concomitant use of ACE inhibitor. Image at:

5
Venous Insufficiency 7 million Americans with VI.
1 in 1000 with a venous ulcer Internists, vascular surgeons, plastic surgeons, dermatologists. $1 billion/ year in USA. $40,000 per person

6
Veins: Hold 75% of the blood volume
Are organized into superficial and deep veins connected by perforating veins Have valves for unidirectional flow Are low pressure systems (10-15mmHg) Have thin walls (superficial veins have thicker walls than deep veins.)
 Have thin walls (superficial veins have thicker walls than deep veins.)")
7
Venous Insufficiency is…
Valvular incompetence and venous obstruction. Symptoms worsen as more sites are involved. Iliac veins as especially susceptible. Injured by crossing arteries Venous hypertension leads to ? Dilation of capillary beds, fibrinogen leak, formation of a fibrin cuff that then stops delivery oxygen, nutrients, growth factors. WBC entrapment in the capillary wall, setting up an inflammatory reaction, injuring the vein and valves.

8
Risk factors? Age Obesity Family history Pregnancy Female Gender
Heart failure, hypertension, renal disease H/o Leg injury (fx, burn, crush, penetrating injury), phlebitis, DVT Previous varicose vein surgery Long hours standing, or sitting.
, phlebitis, DVT. Previous varicose vein surgery. Long hours standing, or sitting.")
9
Symptoms and Signs Nocturnal pain, restless legs Orthostatic pain
Edema, Varicosity, Hyperpigmentation, ulceration

10
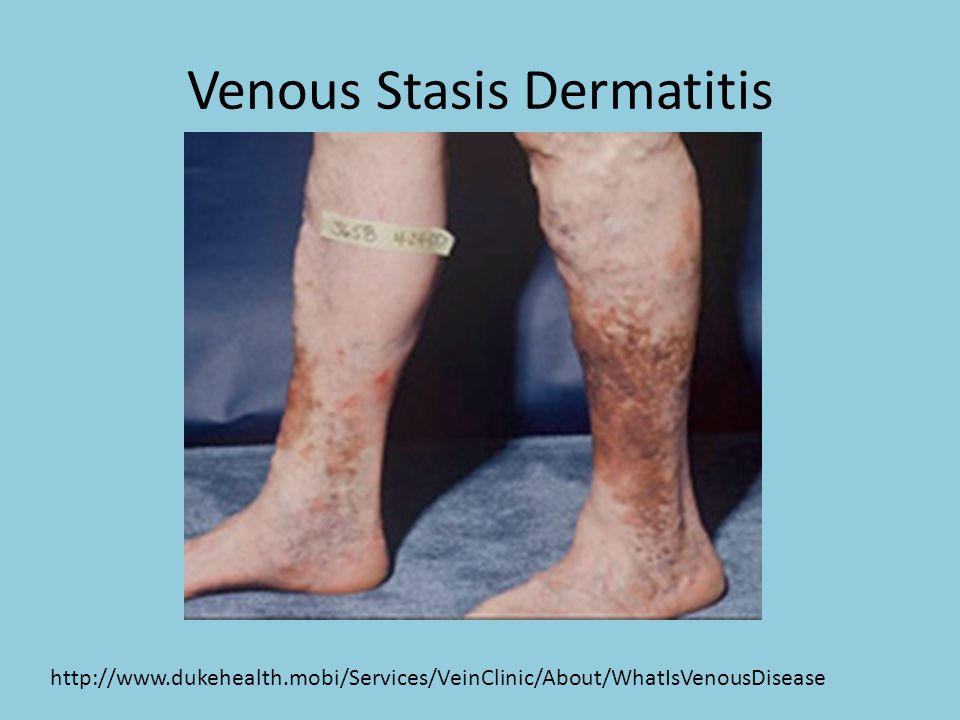
Venous Stasis Dermatitis
11
Stasis Eczema

12
Corona Phlebectasica

13
Lipodermatosclerosis (LDS)
Induration, Fibrosis, the shape of an inverted bottle

14
Venous Ulcer Medial Malleolus Shallow Irregular borders
Base with granulation tissue Surrounding white scar (atrophie blanche) Surrounding hemosiderin deposition Surrounding Edema 80% of LE ulcers $40,000 Venous Ulcer. A. Khachemoune & C. L. Kauffman : Diagnosis Of Leg Ulcers . The Internet Journal of Dermatology Volume 1 Number 2
 Surrounding hemosiderin deposition. Surrounding Edema. 80% of LE ulcers. $40,000. Venous Ulcer. A. Khachemoune & C. L. Kauffman : Diagnosis Of Leg Ulcers . The Internet Journal of Dermatology Volume 1 Number 2.")
15
Clinical Aspects of the Most Common Types of Ulcers of the Lower Limbs
de Araujo, T. et. al. Ann Intern Med 2003;138:

16
Arterial Ulcer

17
Evaluation VI (valvular incompetence, dilated veins) evaluated by duplex ultrasonograhy. AI evaluated by ABI Check rest and stress 0.9 adequate <0.5 severe Compressive tx not helpful

18
Duplex ultrasonography

19
http://www. urgomedical. com/uploaded-files/img/images/schema-ceap-02

20
CEAP A patient has painful swelling of the leg, and varicose veins, lipodermatosclerosis, and active ulceration. Duplex scanning on May 17, 2004, showed axial reflux of the great saphenous vein above and below the knee, incompetent calf perforator veins, and axial reflux in the femoral and popliteal veins. There are no signs of postthrombotic obstruction. Classification according to basic CEAP: C6,S, Ep,As,p,d, Pr. Classification according to advanced CEAP: C2,3,4b,6,S, Ep,As,p,d, Pr2,3,18,13,14 ( , L II). Revision of the CEAP classification for chronic venous disorders: Consensus statement. Journal of Vascular Surgery Volume 40, Issue 6, December 2004, Pages
. Revision of the CEAP classification for chronic venous disorders: Consensus statement. Journal of Vascular Surgery Volume 40, Issue 6, December 2004, Pages")
21
Treatment Compression is the cornerstone of treatment.
At least 40mmHg at the ankle is the goal. Range of 10-60mmHg (TED hose 18mmHg) Knee-High as good as Thigh-High. Open or closed toe per pt preference. Either graduated stockings and wraps Caution with CHF, invasive infection, arterial insufficiency. Compliance very difficult. Replace every 6 months. Size S, M, L, XL based on ankle, calf circum.
 Knee-High as good as Thigh-High. Open or closed toe per pt preference. Either graduated stockings and wraps. Caution with CHF, invasive infection, arterial insufficiency. Compliance very difficult. Replace every 6 months. Size S, M, L, XL based on ankle, calf circum.")
22
Compression Therapy is Key!
Unna Jobst $6 $60

23
Compression Plus… Leg Elevation. Above heart-level for 30 minutes 3 times per day. Diuretics. May help but can’t do much alone. Pentoxifylline. May improve oxygen delivery, inhibit WBC activation. Shown to accelerate ulcer healing mg tid. Aspirin may help some.

24
Surgical Treatment UNC Vascular Surgery Wound Healing Clinic
Vein Center William Marston, MD Grand Rounds 2/19/09

25
Other References Managing the Patient with Venous Ulcers. Tami de Araujo, MD; Isabel Valencia, MD; Daniel G. Federman, MD; and Robert S. Kirsner, MD. 18 February 2003 | Volume 138 Issue 4 | Pages State-of-the-Art Treatment of Chronic Venous Disease. Michael S. Weingarten. Clinical Infectious Diseases, Vol. 32, No. 6 (Mar. 15, 2001), pp Jull AB, Waters J, Arroll B. Pentoxifylline for treating venous leg ulcers. Cochrane Database Syst Rev Wiersema-Bryant LA. Management of edema. In: Sussman C, Bates-Jensen BM, eds. Wound Care: A Collaborative Practice Manual for Physical Therapists and Nurses. Gaithersburg, MD: Aspen; 1998:
, pp Jull AB, Waters J, Arroll B. Pentoxifylline for treating venous leg ulcers. Cochrane Database Syst Rev Wiersema-Bryant LA. Management of edema. In: Sussman C, Bates-Jensen BM, eds. Wound Care: A Collaborative Practice Manual for Physical Therapists and Nurses. Gaithersburg, MD: Aspen; 1998:")
Similar presentations



















