Download presentation
Presentation is loading. Please wait.

1
Kansas Speech and Hearing Association Conference September 29, 2012
A Multidimensional Approach to the Assessment and Treatment of School-Age Children Who Stutter Part I Kansas Speech and Hearing Association Conference September 29, 2012 E. Charles Healey, Ph.D. University of Nebraska-Lincoln 204 Barkley Memorial Center Lincoln, NE

2
A Conceptual Framework For Stuttering Assessment That Leads To Treatment
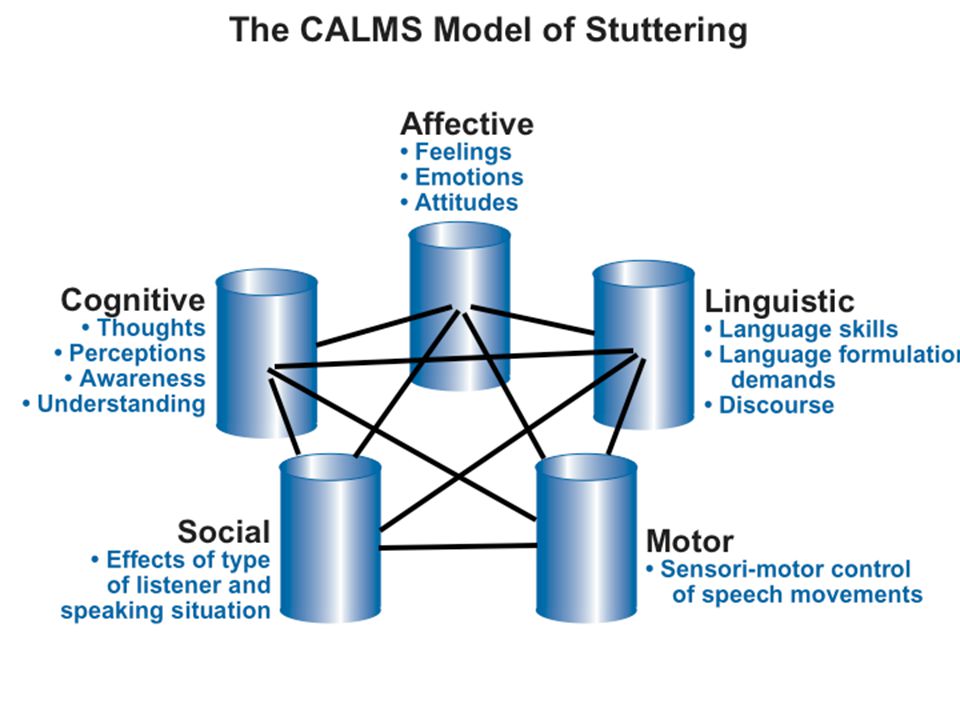
Stuttering is a multidimensional problem which suggests that many factors can contribute to each child’s stuttering in different ways, at different times, with different communicative partners. An assessment should be geared toward assessing multiple aspects of the child, not just his or her stuttering. What we discover from the assessment can provide some direction on what to address in treatment.

4
A Conceptual Framework for Stuttering Assessment and Treatment
Each child who stutters has a unique set of characteristics. No two children are alike so an assessment should discover these unique characteristics. The variability of the disorder is one of its most striking features, which means that improvements in speech might be slow. Children who stutter change across time and the focus of their treatment might need to change as well. Many factors have to be addressed and re-addressed in order for a child to effectively manage his/her stuttering.

5
What Standardized Measures Are Available For Assessing Stuttering in Children?
Stuttering Severity Instrument 4th- Edition (SSI-4; Riley, 2009) The Behavior Assessment Battery for School-Age Children Who Stutter (Brutten & Vanryckeghem, 2007) Included is the Communication Attitudes Test (CAT). Test of Childhood Stuttering (Gillam, Logan, & Pearson, 2009) Overall Assessment of the Speaker's Experience of Stuttering (OASES™) by Yaruss and Quesal (2010)
 The Behavior Assessment Battery for School-Age Children Who Stutter (Brutten & Vanryckeghem, 2007) Included is the Communication Attitudes Test (CAT). Test of Childhood Stuttering (Gillam, Logan, & Pearson, 2009) Overall Assessment of the Speaker s Experience of Stuttering (OASES™) by Yaruss and Quesal (2010)")
6
What are we trying to accomplish in the assessment?
Establish and verify that a child has a fluency disorder Determine the severity of the disorder Determine the variability of the disorder across different situations and settings Examine the emotional reactions a child has to his/her stuttering Determine adverse effect on academics, social-emotional functioning, independent functioning and overall communication. Use assessment data to plan treatment

7
What Measures Should We Obtain?
Traditional measures of stuttering include the frequency and duration of stuttering as well as evidence of secondary coping behaviors. We also need to examine thoughts, awareness, understanding, feelings, attitudes, reactions, and changes in stuttering based on what is said, who it is said to, and in what situation.

8
Assessing awareness, knowledge, and understanding of stuttering
Have the child: Identify stuttering events while reading (% correct) Identify stuttering events while speaking spontaneously (% correct) Identify stuttering events produced from clinician model (% correct) (Awareness and self-monitoring assessment) Test a child’s knowledge of simple facts about stuttering (e.g., boy/girl ratio, % of people who stutter, causes of stuttering, etc.) Test a child’s knowledge and understanding of techniques or strategies that have been used in therapy. How well do they know and understand what they have been taught to do? And, does he/she use those techniques? If not, why?
 Identify stuttering events while speaking spontaneously (% correct) Identify stuttering events produced from clinician model (% correct) (Awareness and self-monitoring assessment) Test a child’s knowledge of simple facts about stuttering (e.g., boy/girl ratio, % of people who stutter, causes of stuttering, etc.) Test a child’s knowledge and understanding of techniques or strategies that have been used in therapy. How well do they know and understand what they have been taught to do And, does he/she use those techniques If not, why")
9
Assessing reactions, feelings, and attitudes toward stuttering
• Determine level of negative reactions the child might have as a result of being a child who stutters. Ask “how often” they feel certain ways (e.g.,feel bad about stuttering, being made fun of, talking to someone you don’t know, etc.) on a rating of “never, a little, sometimes, a lot, or always. • How often are emotional labels tied to stuttering ( e.g., worried, afraid, sad, mad, etc.) Use same ratings as above. • Presence or absence of negative attitudes a child feels about talking (Communication Attitudes. Simply yes or not questions like: I don’t like the way I talk, I’m afraid to speak, I have a hard time saying my name, talking is hard for me, mom and dad worry about how I talk, etc.)
 on a rating of never, a little, sometimes, a lot, or always. • How often are emotional labels tied to stuttering ( e.g., worried, afraid, sad, mad, etc.) Use same ratings as above. • Presence or absence of negative attitudes a child feels about talking (Communication Attitudes. Simply yes or not questions like: I don’t like the way I talk, I’m afraid to speak, I have a hard time saying my name, talking is hard for me, mom and dad worry about how I talk, etc.)")
10
Assessing the impact of speech and language skills on stuttering
• Test the impact of increasingly complex linguistic speech tasks on stuttering frequency. Use simple to complex speech contexts (Automatic speech, sentence repetition, picture description, picture sequence, story retell, script narrative, expository narrative) Stuttering is strongly linked to the length and complexity of the message (Bernstein Ratner & Sih, 1987) • Assess language function (formally or informally) • Assess speech sound production ability (formally or informally) Language and/or articulation disorders coexist with stuttering in about 1/3 of all children who stutter (Arndt & Healey, 2001)
 Stuttering is strongly linked to the length and complexity of the message (Bernstein Ratner & Sih, 1987) • Assess language function (formally or informally) • Assess speech sound production ability (formally or informally) Language and/or articulation disorders coexist with stuttering in about 1/3 of all children who stutter (Arndt & Healey, 2001)")
11
Assessing specific aspects of the stuttering behavior
Obtain measures of the: • Types of disfluencies • Average number of units per repetition • Tempo and regularity of repetitions • Degree of struggle and effort • Percentage of stuttering in spontaneous speech • Percentage of stuttering in reading (can also be used to assess adaptation and consistency effects) • Duration of a typical stuttering moment • Presence of secondary coping behaviors
 • Duration of a typical stuttering moment • Presence of secondary coping behaviors")
12
Assessing the social and situational variability of stuttering
• Determine how often stuttering leads to avoidance of people and words/events. Provide examples of people and situations (teachers and peers—certain words, talking in a group setting, etc.) • Determine how frequently the child stutters with various people and in various social situations (how stuttering is impacted by the type of listener and speaking situation-give examples) • Determine how often stuttering affects friendships and interactions with peers.
 • Determine how frequently the child stutters with various people and in various social situations (how stuttering is impacted by the type of listener and speaking situation-give examples) • Determine how often stuttering affects friendships and interactions with peers.")
14
A Multidimensional Approach to the Assessment and Treatment of School-Age Children Who Stutter Part II E. Charles Healey, Ph.D.

15
Bridging the Gap Between Assessment and Treatment
An analysis of the data collected during the assessment can produce a profile of skills/deficits that can assist the clinician in knowing where to focus attention in treatment. Treatment goals are accomplished by developing activities that include cognitive, affective, linguistic, motor, and social factors as much as possible.

17
Possible treatment Goals Relative to the Sample Assessment Profile
Increase identification, awareness, and understanding of fluency and stuttering. Increase understanding of previously learned speech strategies. Decrease negative emotional reactions to and attitudes toward stuttering and being a person who stutters (Desensitization and stuttering openly)
")
18
Treatment Goals (con’t)
• Increase management of stuttering through the use of the “Big 5” strategies (easy onsets, light contacts, slowed rate, pullouts, and cancellations) • Increase self-management of stuttering through the manipulation of linguistic length and complexity of utterances. • Learn self management skills—problem solving, self monitoring and willingness to practice strategies outside of therapy. • Increase use of new speech skills in a variety of realistic speaking situations.
 • Increase self-management of stuttering through the manipulation of linguistic length and complexity of utterances. • Learn self management skills—problem solving, self monitoring and willingness to practice strategies outside of therapy. • Increase use of new speech skills in a variety of realistic speaking situations.")
19
Examples of Treatment Goals and Activities
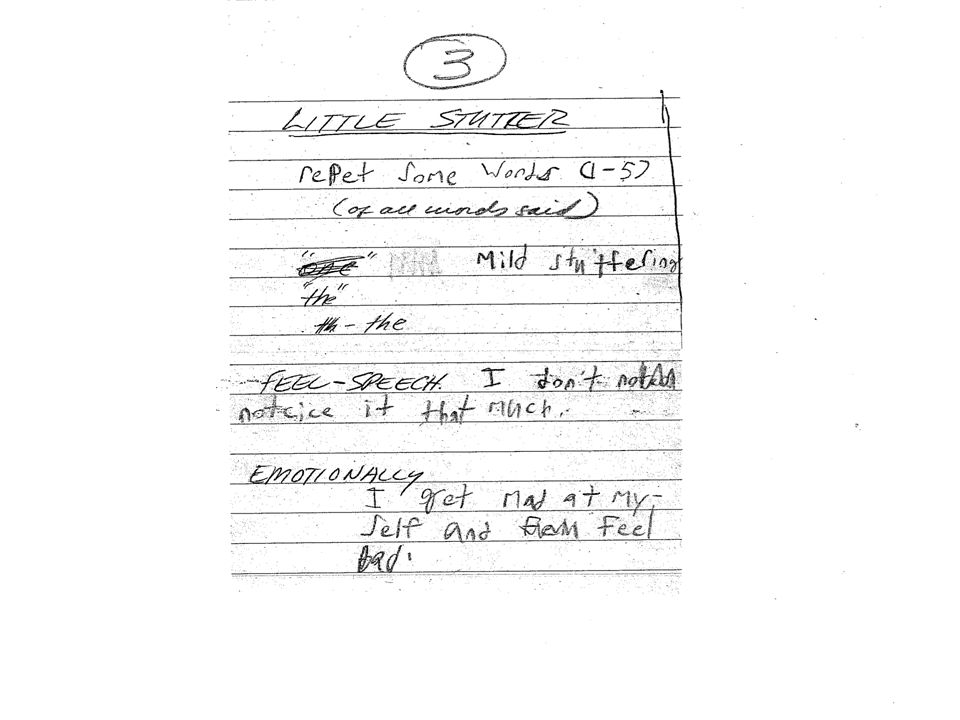
Goal #1: Increase awareness and understanding of stuttering Activity 1: Explore and discuss the differences between normal fluency, normal nonfluencies, little stutters and big stutters by using a piece of paper divided into 4 sections Discuss feelings associated with each. Use voluntary stuttering that mirrors the child’s stuttering pattern. Use simple linguistic contexts for this task. Question for each category of speech, 1. What is happening with your air (breath), voice, tongue and lip movements? 2. How do you feel when you talk that way? 3. How hard to do have to think or work to speak when talking that way?
, voice, tongue and lip movements 2. How do you feel when you talk that way 3. How hard to do have to think or work to speak when talking that way")
24
Treatment Activities for Goal #1 (continued)
Activity 2: Practice using Voluntary Stuttering/Pseudostuttering-- learning and feeling what it’s like to stutter on purpose without tension or struggle. Can also help desensitize the child to the fear of stuttering or covering it up. Convey to the child that “Its OK to Stutter!” so let’s learn about what you do when you stutter. Identify stuttering moments and learn what is happening when you stutter. Learn to stutter in different ways (real vs faked and versions of each). Discuss feelings that go along with the purposeful stuttering as well as the speech changes (motor skills) that are taking place between real and faked stuttering. Hold on to the stutter and slowly release it. Stutter purposefully with a variety of listeners (Desensitization).
. Discuss feelings that go along with the purposeful stuttering as well as the speech changes (motor skills) that are taking place between real and faked stuttering. Hold on to the stutter and slowly release it. Stutter purposefully with a variety of listeners (Desensitization).")
25
Treatment Activity for Goal #1 (continued)
Activity 3: Understand how the speech mechanism works- focus on how physiology of speech is impacted by thoughts and feelings. Diagram of speech system – normal function Note which part of the system is disrupted when negative emotions occur c) How does the speech mechanism function change when you feel anxious, nervous, etc ? (with certain people and/or speaking situations)
 How does the speech mechanism function change when you feel anxious, nervous, etc (with certain people and/or speaking situations)")
26
Goal #2: Decrease negative emotional reactions to and attitudes toward stuttering and being a person who stutters (Desensitization and stuttering openly) Activity 1: Use visual materials to represent stutters and emotional reactions Develop a concrete representation of stuttering through drawings. What does the stuttering “look like to you?” (see next two slides) Have child create clay or play dough figures of to represent stutters and create a play dough “stutter monster.” Create play dough figures that represent emotions that are attached to the “monster.” Write word about a feeling or an emotion connected to stuttering on a piece of paper. Toss paper at target to release feeling or emotion. Could also use clay representations of stuttering and related emotions.
 Have child create clay or play dough figures of to represent stutters and create a play dough stutter monster. Create play dough figures that represent emotions that are attached to the monster. Write word about a feeling or an emotion connected to stuttering on a piece of paper. Toss paper at target to release feeling or emotion. Could also use clay representations of stuttering and related emotions.")
29
Activity #2: Changing Negative Self Talk to Positive Self Talk
Treatment Activity for Goal #2 (continued) Activity #2: Changing Negative Self Talk to Positive Self Talk I’m not stupid, stuttering is just something I do. I have friends who don’t seem to care that I stutter. Stuttering is not my fault and there is nothing wrong with me. I am learning how to talk in an easier way and sometimes what I do doesn’t work but I’m still trying. People think I’m stupid because I stutter. Nobody likes me because I stutter. I stutter so I must be doing something wrong. I wish I could stop stuttering.
 Activity #2: Changing Negative Self Talk to Positive Self Talk. I’m not stupid, stuttering is just something I do. I have friends who don’t seem to care that I stutter. Stuttering is not my fault and there is nothing wrong with me. I am learning how to talk in an easier way and sometimes what I do doesn’t work but I’m still trying. People think I’m stupid because I stutter. Nobody likes me because I stutter. I stutter so I must be doing something wrong. I wish I could stop stuttering.")
30
Goal #3: Strategies for Improving Fluency/Modifying Stuttering
Activity 1: Ways of making talking easier--less stuttered and/or more fluent There are a few ways to make talking easier that can reduce effort, force and tension as well as improve timing, coordination, and rate of speech

31
Ways to make talking easier
Five Key Strategies (The “Big 5”) 1. Easy onsets of phonation 2. Light articulatory contacts 3. Slowed speech rate through continuous phonation 4. Pullouts 5. Cancellations “Easy onsets”, “easy starts”, “easy voice”, “easy on” or “easing in” Two ways to create an easy onset or easy start emphasize increased airflow or gradual voicing onset (e.g., hhhheeeeach or eeeeeach) Draw a “hill or mountain” to represent breathing & voice pattern
 1. Easy onsets of phonation. 2. Light articulatory contacts. 3. Slowed speech rate through continuous phonation. 4. Pullouts. 5. Cancellations. Easy onsets , easy starts , easy voice , easy on or easing in Two ways to create an easy onset or easy start. emphasize increased airflow or gradual voicing onset. (e.g., hhhheeeeach or eeeeeach) Draw a hill or mountain to represent breathing & voice pattern.")
33
Ways to make talking easier
Light Contacts, Pullouts, Cancellations to Reduce Effort/Tension: a. Use light contacts to reduce tension and effort during sound placement—lighten contact by using more airflow during the contact b. Pullout or “ease out” of a stutter c. Cancel a stutter slowly and easily and then change to make the next attempt less stuttered or fluent. d. Rate any muscle tension during stuttering on a scale of 1-10

34
Ways to make talking easier
Reduce rate and transitions between words: a. prolonged method or “stretched speech” (Onslow et al., 1996) b. pause and stretch short phrases to reduce overall pace of a verbal interaction. ** Set up practice of specific strategies outside of therapy to facilitate generalization with other listeners--keep it simple
 b. pause and stretch short phrases to reduce overall pace of a verbal interaction. ** Set up practice of specific strategies outside of therapy to facilitate generalization with other listeners--keep it simple.")
35
Learn self management skills—problem solving, self monitoring and willingness to practice strategies outside of therapy. • Strategies are a plan for improvement • Have to be used voluntarily • Client must be aware of what to do and have confidence strategies will work • Client has to think about them and learn them • Fluency clients might develop only limited use or skill given the level of stuttering and motor stability

36
Six Steps in Developing Self Regulated Strategies (Reid & Lienemann, 2006)
Develop and define the skills needed. Discuss the strategy: “Sell it” and have client “buy in” Model the strategy: See the “expert” do it. Knows what to do, why it is being used, how to do it, recognize they know that they are doing it, and what needs to happen to keep it going Have child memorize the strategy Support the strategy—shift responsibility for use of strategy to the client, decrease prompting Develop independent performance

37
Goal #4: Increase self-management of stuttering through the manipulation of linguistic length and complexity of utterances. Activity: Manipulating the length and complexity of responses while using selected speech strategies. - Begin with contextualized materials concerning a theme or topic the child enjoys talking about. Information can be found on the internet and/or the child can bring information to therapy that is familiar to him or her. Materials Include: • pictures • drawings • written materials of any kind

38
Suggested linguistic complexity sequence coupled with strategy use
1. Labeling and short description of terms. Oral reading first then repeat content using eye contact with listener 2. Longer description of terms and concepts- some from material/some from personal experience. 3. Use questions that require an inference or an interpretation of information. 4. Story telling that is scripted 5. Unscripted story telling or topic discussion that is decontextualized.

39
Examples of linguistic complexity sequence coupled with strategy use—Topic is Baseball
Labeling --pitcher, catcher, first baseman, second baseman, home plate, foul lines, outfield, etc. Short Description -- Double play: when two outs are made before 2 runners reach base. -- Slide: when a player slides on the ground to touch the base.

41
Examples of linguistic complexity sequence coupled with strategy use—Topic is Baseball
Longer descriptions and concepts -- Tell me three ways a “strike” can occur. (client repeats all three ways listed below) a. the batter swings and misses the pitch b. the batter hits the fall foul (outside the lines of first and third base). c. the batter tips the ball and it’s caught by the catcher. --What is an “inning?” The part of the game when on team bats and has three outs and the other teams bats and has three outs. The bottom of the inning is always given to the home team.
 a. the batter swings and misses the pitch b. the batter hits the fall foul (outside the lines of first and third base). c. the batter tips the ball and it’s caught by the catcher. --What is an inning The part of the game when on team bats and has three outs and the other teams bats and has three outs. The bottom of the inning is always given to the home team.")
42
Examples of linguistic complexity sequence coupled with strategy use—Topic is Baseball
Inference and Interpretation -- Why is it difficult for pitchers to get strikeouts? -- If there is a runner on first base and the batter hits the ball on the ground, what might happen next? -- What happens when a runner tries to steal a base? Scripted story telling -- read short stories about baseball or professional base ball players and have the child retell the story. Unscripted story telling/Conversation -- Have child tell personal story about a baseball game that he played in or attended as a fan. -- Have a conversation about baseball or something that happened recently in the news about baseball.

43
Picture Description C “Tell me what you are thinking about before you say the first phrase.” A “Tell me how you are feeling before or during the time you say something about the picture.” L “What you are going to say?” (How long and complex is it?) M “How are you going to say it? Use a strategy when you tell me about the picture.” S Who are you talking to? (Client talks to clinician, another person in therapy or take home to parents)
 M How are you going to say it Use a strategy when you tell me about the picture. S Who are you talking to (Client talks to clinician, another person in therapy or take home to parents)")
44
Treatment example of how the linguistic context can be used to support cognitive, affective, motor, and social domains SPEECH MATERIAL 1. Baseball is a game that is played on a field shaped like a diamond. 2. The long boundary lines of the field go from home plate in a line to the first and third base sides of the field. 3. A foul ball occurs when the the ball is hit outside of the lines of the playing field. 4. The object of the game is to get more runners to cross home plate than the other team during a nine inning game. 5. All the players sit in dugouts while their team is at bat. Everyone sits in the dugout while one person bats and another player gets ready to become the next hitter. CLINICIAN FOCUSES ON: Selection of 1, 2, or 3 strategies to practice—even include some voluntary stuttering. What is the child going to use and does he understand how and why the strategy works? If there there is any emotional or physical tension present before or during speech practice? Monitoring performance and wait for a couple of seconds to give feedback. How did that feel? How did that work? What changed? What didn’t change? Having child rate performance on a scale of 1-5. Having child read the phrases and then say phrases using eye contact with clinician. Say it again to another listener (if possible) Have child make comments or answer questions about the topic so that it is more difficult and challenging.
 Have child make comments or answer questions about the topic so that it is more difficult and challenging.")
45
What types of data do I need to collect to document outcomes?
Documenting progress (or lack thereof) in treatment involves both quantitative and qualitative measures. Use a portfolio approach to documenting changes. Not all goals or processes achieved in therapy have to be quantified. Qualitative data such as: 1) comments from the child, parents, or teachers, 2) drawings, diagrams, and a transcript of explanations of concepts that relate to any cognitive, affective, motor, or social component being treated.
 in treatment involves both quantitative and qualitative measures. Use a portfolio approach to documenting changes. Not all goals or processes achieved in therapy have to be quantified. Qualitative data such as: 1) comments from the child, parents, or teachers, 2) drawings, diagrams, and a transcript of explanations of concepts that relate to any cognitive, affective, motor, or social component being treated.")
46
Quantitative Measures
• Reductions in stuttering frequency and severity (% of stuttered words or syllables and improvements in SSI-4 score) • Speech rate within normal limits (conversational or narrative speech rates for children 7-11 ranges from syllables per minutes). • Naturalness of speech (rated on a scale of 1-9; 1= highly natural and 9=highly unnatural). • Improvements in cognitive, affective, linguistic, and social measures obtained during the assessment, using objective data across multiple occasions to show change
 • Speech rate within normal limits (conversational or narrative speech rates for children 7-11 ranges from syllables per minutes). • Naturalness of speech (rated on a scale of 1-9; 1= highly natural and 9=highly unnatural). • Improvements in cognitive, affective, linguistic, and social measures obtained during the assessment, using objective data across multiple occasions to show change.")
47
Concluding Thoughts • Approach therapy as a dynamic, multidimensional process. Many factors interact to maintain the disorder and multiple factors need to be addressed in therapy. Consider therapy as a journey not a destination. • Use a multidimensional assessment that includes more than just a measure of stuttering in order to tailor the therapy to the needs of the child. • Children who stutter need to see that they should not hide from their stuttering, that it’s OK to stutter, and with time and a little work, they can learn to talk in an easier way.

48
References Arndt, J. & Healey, E.C. (2001). Concomitant disorders in school-age children who stutter. Language, Speech, Hearing Services in Schools, 32, Bernstein Ratner, N. & Sih, C. (1987). Effects of gradual increases in sentence length and complexity on children’s dysfluency. Journal of Language Speech and Hearing Disorders, 52, Bloodstein, O. & Bernstein Ratner, N. (2008). A handbook on stuttering. 6th Ed. Clifton Park, NY: Delmar Learning. Bothe, A. K., Davidow, J. H., Bramlett, R. E., & Ingham, R. J. (2006). Stuttering treatment research : I. Systematic review of incorporating trial quality assessment of behavioral, cognitive, and related approaches. American Journal of Speech-Language Pathology, 15 (4), Brutten, G. and Vanryckeghem, M. (2007). Behavior Assessment Battery for School-Age Children Who Stutter. San Diego, CA: Plural Publishing. Healey, E.C., Scott Trautman, L., and Susca, M. (2004). Clinical applications of a multidimensional model for the assessment and treatment of stuttering. Special Issue on fluency disorders in Contemporary Issues in Communication Disorders, 31, Healey, E.C., Scott Trautman, L. & Panico, J. (2001). A model for manipulating linguistic complexity in stuttering therapy. International Stuttering Awareness Day Online Conference, Mankato State University, Mankato, MN.
. Effects of gradual increases in sentence length and complexity on children’s dysfluency. Journal of Language Speech and Hearing Disorders, 52, Bloodstein, O. & Bernstein Ratner, N. (2008). A handbook on stuttering. 6th Ed. Clifton Park, NY: Delmar Learning. Bothe, A. K., Davidow, J. H., Bramlett, R. E., & Ingham, R. J. (2006). Stuttering treatment research : I. Systematic review of incorporating trial quality assessment of behavioral, cognitive, and related approaches. American Journal of Speech-Language Pathology, 15 (4), Brutten, G. and Vanryckeghem, M. (2007). Behavior Assessment Battery for School-Age Children Who. Stutter. San Diego, CA: Plural Publishing. Healey, E.C., Scott Trautman, L., and Susca, M. (2004). Clinical applications of a. multidimensional model for the assessment and treatment of stuttering. Special Issue on. fluency disorders in Contemporary Issues in Communication Disorders, 31, Healey, E.C., Scott Trautman, L. & Panico, J. (2001). A model for manipulating linguistic. complexity in stuttering therapy. International Stuttering Awareness Day Online. Conference, Mankato State University, Mankato, MN.")
49
References Ingham, J. and Riley, G. (1998). Guidelines for documentation of treatment efficacy for young children who stutter. Journal of Speech-Language-Hearing Research. 41, Manning, W. H. (2010). Clinical decision making in fluency disorders. Clifton Park, NY: Delmar, Cengage Learning. Maas, E., Robin, D., Hula, S, Freedman, S, Wulf, G, Ballard, K, & Schmidt (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17, Onslow, M., Costa, L., Andrews, C., Harrison, E., & Packman, A. (1996). Speech outcomes of a prolonged-speech treatment for stuttering. Journal of Speech and Hearing Research, 39, Reid, R. & Lienemann, T. O. (2006). Strategy instruction for students with learning disabilities. New York: Guildford. Smith, A. (1999). Stuttering: A unified approach to a multifactorial, dynamic disorder. In N. Ratner and E. C. Healey (Eds.) Stuttering research and practice: Bridging the gap. Mahwah, New Jersey, Lawerance Earlbaum Associates, Publishers. Starkweather, C. W. & Givens-Ackerman, J. (1997) Stuttering. Austin, TX: PRO-ED, Inc. Yairi, E. & Seery, C. (2011). Stuttering: foundations and clinical applications. Upper Saddle River, NJ: Pearson.
. Clinical decision making in fluency disorders. Clifton Park, NY: Delmar, Cengage Learning. Maas, E., Robin, D., Hula, S, Freedman, S, Wulf, G, Ballard, K, & Schmidt (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17, Onslow, M., Costa, L., Andrews, C., Harrison, E., & Packman, A. (1996). Speech outcomes of a prolonged-speech treatment for stuttering. Journal of Speech and Hearing Research, 39, Reid, R. & Lienemann, T. O. (2006). Strategy instruction for students with learning disabilities. New York: Guildford. Smith, A. (1999). Stuttering: A unified approach to a multifactorial, dynamic disorder. In N. Ratner and E. C. Healey (Eds.) Stuttering research and practice: Bridging the gap. Mahwah, New Jersey, Lawerance Earlbaum Associates, Publishers. Starkweather, C. W. & Givens-Ackerman, J. (1997) Stuttering. Austin, TX: PRO-ED, Inc. Yairi, E. & Seery, C. (2011). Stuttering: foundations and clinical applications. Upper Saddle River, NJ: Pearson.")
50
Internet Resources Major resource and links to other websites about stuttering: Stuttering information for professionals and consumers Stuttering Foundation of America: National Stuttering Association UNL Fluency Center

Similar presentations














>")







>")





