Download presentation
Presentation is loading. Please wait.

1
The Community Health Center Association of CT
Team-Based Care Webinar #3 Population Health, Care Management, Self Management Support & Care Coordination Presented to The Community Health Center Association of CT Presented by Susan Crocetti, RN & Regina Neal, MPH, MS March 30, 2012 1

2
Objectives Explore the importance of and methods necessary to use team-based care in the successful delivery of: understanding and acting on needs of populations of patients meeting the needs of patients with conditions that respond well to evidence-based guidelines and care management assisting patients to partner in the successful management of their conditions coordinating the care of patients and providing continuity across various levels and transitions of care

3
When Providers Work Without a Team
Delivering all evidence-based guidelines for preventive and chronic disease care has been estimated to take 18 hours a day for an average sized patient panel (Yarnall et al 2009; Alexander et al 2005) Most physicians only deliver 55% of recommended care, 42% report not having enough time with their patients (Center for Studying Health System Change 2008; Bodenheimer & Laing 2007) Providers are spending 13% of their day in care coordination and only using their medical knowledge 50% of the time (Gottschalk 2005; Margolis & Bodenheimer 2010) Patient care is fragmented and patients are dissatisfied with the level of attention they receive in primary care (Bodenheimer 2008)
 Most physicians only deliver 55% of recommended care, 42% report not having enough time with their patients. (Center for Studying Health System Change 2008; Bodenheimer & Laing 2007) Providers are spending 13% of their day in care coordination and only using their medical knowledge 50% of the time. (Gottschalk 2005; Margolis & Bodenheimer 2010) Patient care is fragmented and patients are dissatisfied with the level of attention they receive in primary care (Bodenheimer 2008)")
4
Who is On the Team and Who Can Support the Team?
Core Team: Provider, MA’s, LPN’s, Clerk Internal Resources: RN’s, Referral Coord, Billing Staff, Dietician, Educators, IT Staff, Pharmacists, SW External Resources: Community Health Workers, Insurance Nurse Disease/Case Managers, Vendors, Specialists, Hospitalist

5
Supporting the Work of the Team
Human Resources (core, internal and external) Systems (PMS, Registry, E-Rxing, HER, Portal) Clinical tools (flowsheets, structured notes, EMR templates and decision support functions, Standing orders) Written Standards (Job descriptions, workflows) Training Program Evaluation and Feedback
 Systems (PMS, Registry, E-Rxing, HER, Portal) Clinical tools (flowsheets, structured notes, EMR templates and decision support functions, Standing orders) Written Standards (Job descriptions, workflows) Training Program. Evaluation and Feedback.")
6
Delivering Between Visit Support to Populations of Patients
Sub categories of patients by age, sex, diagnosis, etc. are identified Have these patients received services as recommended in the evidence-based guidelines or are their outcomes in line with expectations? Patients who are missing these services or are not in goal can be contacted for follow up or referred for more intensive management This data can be used to understand how well we are providing care and if we are improving

7
So, How Do You Do This? Analyze your patient panel and community demographics Demographics (Age, Sex, Race, Ethnicity, Income & Education Level) PMS, registry, EMR reports Local census data Clinical Information (Diagnosis, medications, allergies, clinical measurements Risk Factors (smoking, family circumstances, drug use, mental health concerns, etc.) How is a team able to achieve this? Systems, IT resources, written training materials, admin support
 How is a team able to achieve this Systems, IT resources, written training materials, admin support.")
8
But First You Have to Capture the Information…
Who collects the information and is it entered accurately? Allergies, risk factors, preventive service updates, etc. can be captured by MA/LPN at beginning of visit Are structured (mapped) fields being used to allow reports to be generated? Does someone know how to set up and run the reports accurately and is there time dedicated to this?
 fields being used to allow reports to be generated Does someone know how to set up and run the reports accurately and is there time dedicated to this")
9
Workflow Considerations for Comprehensive Health Assessments
Could patient self assessments be completed by the patient at home prior to visit; accessible as a form on the website or portal? Would require pre-visit planning and staff assigned to mail the form or advise/remind patient to use portal MA’s could assist with completion and data entry prior to provider portion of visit Ideal if this information is also captured as structured data Define when this is done initially and when updated (annually?)
")
10
Choosing Clinical Measures to Monitor Your Population
Use National Quality Forum sanctioned measures for standardization and benchmarking for quality improvement Choose a balanced scope of measure “types” Efficient to link with important conditions or high risk group Consider vendor-ready MU CQM’s and UDS cross mapping How complete or automated is the data? Who makes the decision at the practice? Is the team included in the discussion and aware of the project from the beginning? They may have valuable information to help avoid some pitfalls.

11
Reporting is the Next Step
Setting up the technical specifications Provider / Team attribution – clean up those panels! Data Quality – team members are the key! Manual data entry outside of visits Historical data / preloading the EMR Outside data Data entry during visits Using correct fields for data entry / mapping issues Interfaces Mapping issues or other technical concerns (POS vs. POC results) Data entry errors Timeliness (communication between those responsible for data entry and those running reports)
 Data entry errors. Timeliness (communication between those responsible for data entry and those running reports)")
12
Testing and Transparency to Improve Quality and Maintain Trust
Test on one team first Share technical specifications of reports (numerator and denominator definitions) with providers and teams QA initial reports before distribution to uncover major errors (and hold onto your credibility!) Give report detail to providers/teams to verify that a “No means No” (and not a problem with how the data was collected / report set up) Give feedback to teams on what you’ve learned about the reporting process – good and bad
 with providers and teams. QA initial reports before distribution to uncover major errors (and hold onto your credibility!) Give report detail to providers/teams to verify that a No means No (and not a problem with how the data was collected / report set up) Give feedback to teams on what you’ve learned about the reporting process – good and bad.")
13
Once You Have Confidence in the Reports, Take Action – But Be Prepared
What Who, When, How Considerations Phone Calls Personal vs. automated Front office vs. back block of time vs. “fit in” centralized vs. team –based Vendor vs. internal Wrong number HIPAA – leaving message on VM or with another person How many attempts Letters Wrong address Looks like a bill Automated errors Secure Electronic Communication Names distributed to team for further action Providers Care Managers Educators Referral Coordinator Patient Navigator Clearly define expectations F/u to ensure actions were taken Share ideas

14
Everyone Must Be Involved in Supporting the Team’s Population Management Work with Contingency Plans
Wrong letter Deceased Patient got the service already Patients call but can’t get through / in (consider timing with back to school or flu season) You run out of vaccine Staff aren’t aware of outreach and don’t know how to handle questions or complaints
 You run out of vaccine. Staff aren’t aware of outreach and don’t know how to handle questions or complaints.")
15
Words of Encouragement
Scripting of outreach call or contingency responses and Wording of outreach letters Get feedback from all staff so the wording is done in a way that the patients will understand Use this as an opportunity to remind the patients that they are part of your team!

19
Did It Make a Difference?
Keeping track of who responded because of the outreach – how will you know? Compare pre and post clinical metrics Ask staff and patients what they liked or didn’t like about the initiative; get their thoughts on how to do it better next time Celebrate the success of this team effort!!

20
Population Management, Meet Quality Improvement…
If patients got the service in the first place there would be fewer names on those lists to outreach!! Involve the team (and patients!) in ideas of how to get the patient to complete the service before it’s overdue No such thing as a crazy idea (well, yes there is, but it’s ok, because it might lead to an idea that’s not so crazy)
 in ideas of how to get the patient to complete the service before it’s overdue. No such thing as a crazy idea (well, yes there is, but it’s ok, because it might lead to an idea that’s not so crazy)")
21
Moving From Population Generalized Needs to a Focus on Individuals with Specific Needs
Care Management Assuming responsibility for the patient’s care needs Ensuring continuity of care Utilizing evidence-based guidelines as care delivery standards Coordinating necessary specialty care Following transitions to and from care outside the practice © Qualis Health 2010 4

22
Is Care Management a Position or a Concept?
How can a team accomplish the components with or without a designated RN Care Manager position Identify criteria for intensified services; at-risk individuals Adopt evidence-based guidelines of care; pre-visit planning Establish plan of care with patient/family input, goals, assessment of progress toward goals; exploring barriers, acting to remove barriers Coordinate services from all care givers to ensure continuity Follow-up for care provided in facilities Coordinate medically necessary referral services Facilitate proactive communication; interdisciplinary team conferences Disease-specific and preventive health education Self-management plan and support

23
How to Help the Team Provide Care Management
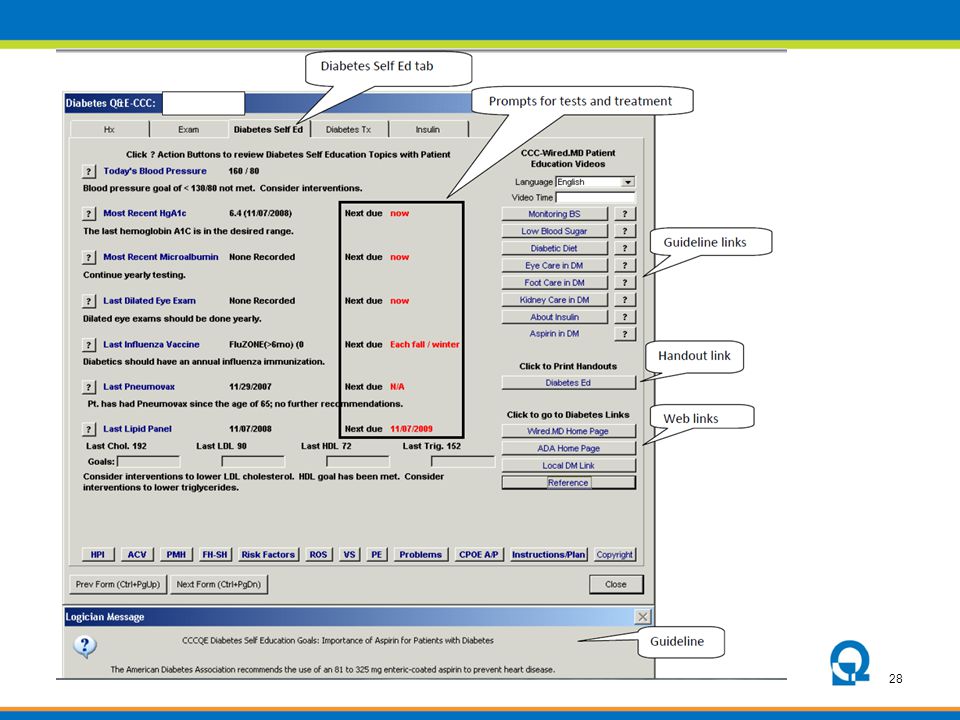
How to Help the Team Provide Care Management? Choosing Guidelines and Implementing Tools Prompts for services Standing orders Prompts for H&P Decision support for treatments Order sets Condition specific flowsheets Patient Education Care Plans Goal setting and assessment Templates in condition specific progress notes Staff workflow and training materials Alerts

24
Mercy Clinics, Inc. Des Moines, Iowa

29
Example of Written Plan of Care
Denmark D. Patient-physician partnering to improve chronic disease care. Fam Pract Manag. May 2004:55-56

30
Self-Management Plan/Tool

31
Are The Tools User Friendly?
Consider the affect on workflows of all team members – get their input! Establish the best sequence for templates and forms Consolidate actions onto one screen/form or provide links between templates or functions in EMR for team efficiency Smart phrases/quick text options for efficient documentation Choose key areas for prompts to avoid alert or “click” fatigue in EMR’s

32
Sustaining Use of EMR Templates
Allow for customization whenever possible: Users appreciate the ability to customize applications to their own work processes and are more likely to adopt and continue using the system if such capabilities exist. Engage patients in the technology: Showing the computer screen to the patient and collaboratively writing notes can enhance the patient–physician interaction, thus making physicians more likely to continue using the system. To maintain patient support for the system, make it clear that care recommendations are based on individual health needs. AHRQ Health Care Innovations Exchange / Schnipper, JL McColgan KE, Linder JA, et al. Improving management of chronic diseases with documentation-based clinical decision support: results of a pilot study. AMIA Annu Symp Proc. 2008; 1050.

33
Care Coordination: Closed Loop Test Tracking
Ensures that results are received, reviewed by provider, and acted upon for every lab or imaging test ordered Who tracks depends on: Type of test Where the test was performed How results are received Electronic systems to support the process Methods include Fully automated order/result reconciliation Partially automated reports Manual logs, accordion file or spread sheets Situations that could result in a test not being performed or communicated appropriately: Failure to order the test correctly Failure to meet insurance coverage criteria Failure to contact and schedule the patient for test Failure of the patient to show up for test Technical issue resulting in incomplete testing (QNS, for example)
![]()
34
Communicating Test Results
Normal & abnormal results Establish timeframe for communicating to patients and let them know what to expect Proactive vs. reactive communication Who is responsible? EMR workflow can be standardized so that as provider signs off on labs, a patient letter is created, routed to the MA who prints and mails at the end of the day

35
Closed Loop Referral Tracking
Ensures that the patient completed a visit and a note was received back from the specialist each time a specialty referral given to the patient Who does this, does type of referral matter?
![]()
36
Coordinating Transitions of Care
How do you know there has been an ER visit or hospitalization? Coordination with other care facilities (rehab, SNF, etc.) Transfer to new PCP Transition from pediatric service to adult medicine Who does this and when?
 Transfer to new PCP. Transition from pediatric service to adult medicine. Who does this and when")
37
When Will the Care Management Services Be Delivered?
What staff are qualified and available? RN’s for complex patients LPN’s and MA to follow specific guidelines approved by providers and RN’s for preventive, straight forward education and management When can these services be provided? Incorporating into visit cycle Exploring alternative visit types Telephonic consultation Mailings

38
Pre-visit Planning Care Coordinator reviews :
Health Maintenance services due Medication Reconciliation Records Lab Log to determine outstanding labs Referral Log to determine outstanding consults Complex Needs to be referred internal or external Huddles used for focused communication on the day of the visit

39
Incorporating Care Management By The Team Into The Visit Cycle
Before the Provider Portion of the Visit PCP, demographics, missing reports, preventive services, risk factors, med rec, test & referral tracking, SMS, basic pt ed, agenda During the Provider Portion of the Visit Assess, diagnose, care plan, deliver services After the Provider Portion of the Visit Reinforce care plan and SMS plan, complex education and SMS by others

40
In Between Visits is KEY!!
Population management reports & outreach Data entry QA of reports F/u phone calls Pre-visit planning Test & referral tracking Communication of test results F/u after transitions Establishing external resources and community services Enhance technology Training & standard development! How do you manage to get this done with a full day of patients?

41
Alternative Visit Option: Planned Care Visit
Visit is structured similar to a physical exam Interval determined by condition Tightly choreographed agenda so nothing is missed Follow up phone call Multi-disciplinary to bring in other perspectives Nutrition Exercise Pharmacist Daily huddle is essential to efficient planned care

42
Annual Planned Exam Workflow
One month prior to appointment: Letter to the patient with lab slips and notification of other Health Maintenance requirements Three weeks prior to appointment: MA contacts patient to schedule routine testing (e.g., mammogram, bone density, etc.) One week prior to appointment: Patient has labs drawn Two days prior to appointment: Place appointment reminder call to patient and remind them to bring patient questionnaire and medication list (better yet, medications) with them
 One week prior to appointment: Patient has labs drawn. Two days prior to appointment: Place appointment reminder call to patient and remind them to bring patient questionnaire and medication list (better yet, medications) with them.")
43
Shared Medical Appointment
A shared medical appointment, also known as a group visit, is a 90-minute visit when multiple patients are seen as a group for follow-up, routine or consult care.

44
Team Based Care Delivered in a Shared Medical Appointment or Group Visit
Open more access to patients to be cared for by the team Improves productivity and enhances efficiency of a healthcare team Enhance the patient’s visit by offering a therapeutic approach – time for education and self management support Patients teach patients by sharing experiences and helpful information who may be dealing with the same issues Agenda setting is more flexible and the pace of the visit is more relaxed

45
Provider Support or Nurse Visits
Used for follow up such as: Blood pressure rechecks Vaccines given in a series Hearing and vision screening Patient teaching Anticoagulation management Others?

46
Just one more outreach call….
Questions?? Just one more outreach call….

Similar presentations