Download presentation
Presentation is loading. Please wait.

1
” قالوا سبحانك لا علم لنا إلا ما علمتنا إنك أنت العليم الحكيم“
بسم الله الرحمن الرحيم ” قالوا سبحانك لا علم لنا إلا ما علمتنا إنك أنت العليم الحكيم“

2
Mostafa EL-Haddad Kasr El-Ainy Hospital Cairo University
Head And Neck Cancer Mostafa EL-Haddad Kasr El-Ainy Hospital Cairo University NEMROCK 2009

3
Proposal For Work Flow Wide field with a predefined borders (between the physician and the radiographer). Simulator film. Blocks to be drawn on the Simulator film. (better in a predefined shapes :triangles, Rectangles, and Squares) Physics planning. UK system Educational purposes
 Physics planning. UK system. Educational purposes.")
4
Category 1 Priority; Patients with the tumour types for which there is evidence that prolongation of treatment affects outcome, and who are being treated radically with curative intent. The data reviewed show very strong evidence that prolongation of overall treatment time affects treatment outcome or local tumour control (cure rates) in patients with the following tumours: • SCC of the head and neck region. • SCC cervix. • non-small cell carcinoma of lung (NSCLC). Guidelines for the Management of the Unscheduled Interruption or Prolongation of a Radical Course of Radiotherapy (2nd Edition. 2002).
 in patients with the following tumours: • SCC of the head and neck region. • SCC cervix. • non-small cell carcinoma of lung (NSCLC). Guidelines for the Management of the Unscheduled Interruption or Prolongation of a Radical Course of Radiotherapy (2nd Edition. 2002).")
5
MD Anderson series showed that completed combined treatment (Surgery+Radiotherapy) in 11 weeks is better than 11 to 13 weeks and more than 13 weeks is the worst.
 in 11 weeks is better than 11 to 13 weeks and more than 13 weeks is the worst.")
6
Why Head And Neck Is Special
Very Complicated anatomy. Many risk organ in a very narrow space. Needs high precision. Patients in very bad shape. RCR report for priority.

7
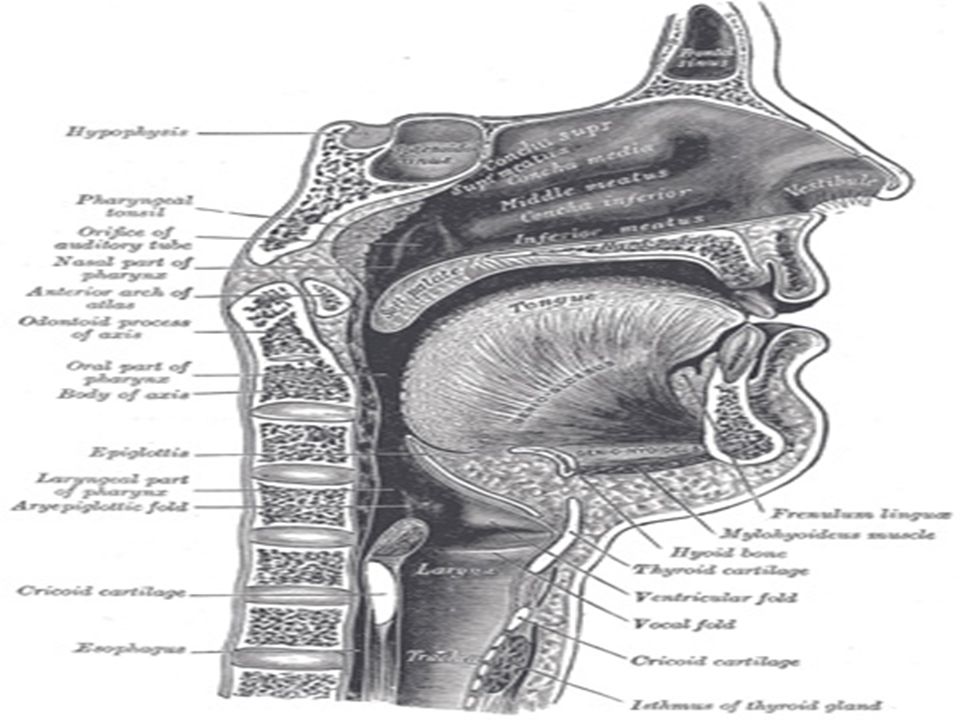
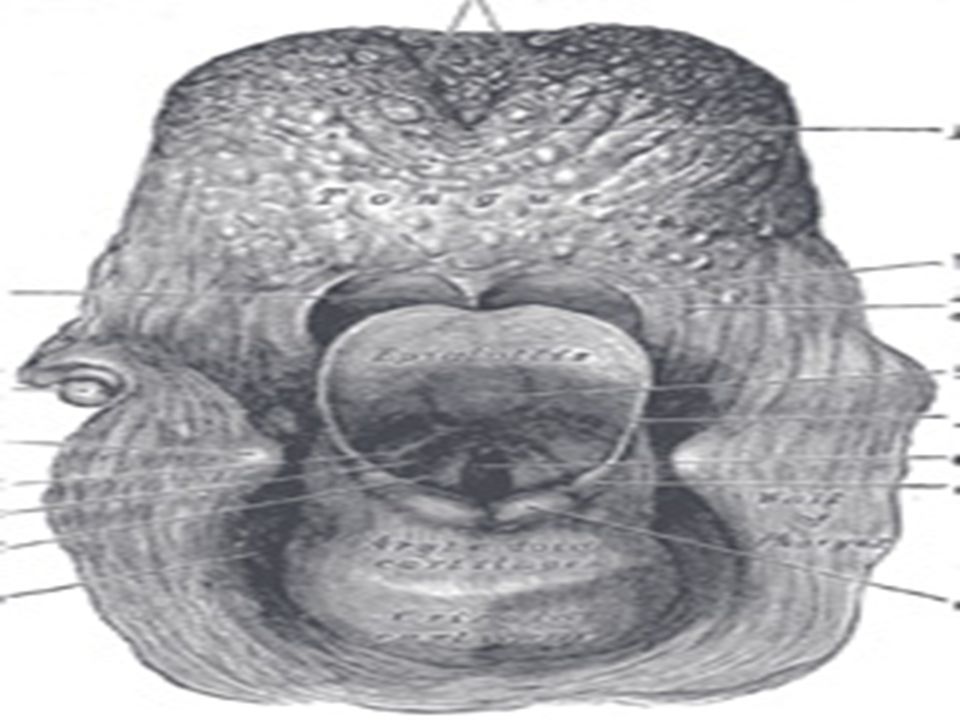
ANATOMY

13
Imaging In Head and Neck Cancer
CT scan: Accurate information about pneumatization, integrity of bony structures. MRI: soft tissue extension, Perineural, perivascular infiltration, intracranial extension. Base of skull CT? MRI?. Imaging before or after Biopsy? Larynx?

14
General Rules for Imaging
MR of choice in: Parotid, facial area, skull base (intracranial extension), Any tumor with potential perineural affection, oral cavity and oropharynx. T2 WI excellent tumor to muscle enhancement. T2 allows differentiation between secretions and mucosal thickening together with tumor which have low signal (Low water content). In T1 look at the tumor invading Fat. (Fat shows high signal in T1).
, Any tumor with potential perineural affection, oral cavity and oropharynx. T2 WI excellent tumor to muscle enhancement. T2 allows differentiation between secretions and mucosal thickening together with tumor which have low signal (Low water content). In T1 look at the tumor invading Fat. (Fat shows high signal in T1).")
15
CT is preferable if Swallowing may be a problem. (Ca Larynx).
DON’T FORGET NECK ULTRASOOUND. PET and PET CT.

16
Thyroid. Parotid. Ear. Eye and Orbit. PNS. FORGET IT

17
Immobilization Comfort and immobilization. Unsightly setup marks. Mask, Tape stretched, Beam directing shell. Coughing, sneezing, respiration and swallowing. Mark LNs. Important land marks: (canthus, orbits, external auditory canal, oral commissures). Before making the mask, use the fluoroscopy to align the patient and put him in the suitable position.
. Before making the mask, use the fluoroscopy to align the patient and put him in the suitable position.")
18
In Our Department Put all head and neck patients on the C head rest.
PNS, Nasopharynx. (MAIN). Ear, parotid: may be on patient side. Pituitary in Flexion. You can use hyperextension in any patient where you can protect the larynx .
. Ear, parotid: may be on patient side. Pituitary in Flexion. You can use hyperextension in any patient where you can protect the larynx .")
19
Facial Mask system Thermoplastic mask. Beam directing shell.
Plastic material.

20
Radioopaque Markers And Stents
Wires to mark important structures or lymph nodes. Stent to depress the tongue, protrude the lips.

21
Patient Fixation

22
Positioning Mask on the Simulation, Why?

23
Positioning Tilt your patient head ?? Do you know what you did?
You re tilting the gantry.

24
Positioning e.g.: If the head of the patient is rotated 10 degree you have to turn the gantry in the same direction for 10 degree as well. If you want to see this you can put a small lead mark on the patient eye and put the gantry in 90 degr both leads should be on one line.

25
Positioning Bad alignment for your patient, Do you know what you are doing?? You are turning your couch

26
Neutral Position Head elevation required to produce a neutral position varies from patient to patient, depends on the patient chest size, In some patients specially children it might be necessary to elevate the patient chest to achieve a comfortable position. A styrofoam of adequate thickness can be placed below the chest every session.

27
Head supports Hyperextension can be achieved by elevating the chest without make a strain on the head.

28
Head support

29
The neck is rested but not the head, this open room for a movement
A comfortable head support is one that tightly fits to the posterior surface of the head and neck and help the patient to maintain the position without straining. The neck is rested but not the head, this open room for a movement

30
Dental Impression When you have to use tongue depressor?

31
Dental Impression When the maxillary antrum is treated the Tongue and lower half of the mouth can be excluded. Likewise, when a tumor of the tongue or the floor of the mouth are treated the upper part of the mouth can be excluded. Used a dental impression material with a syringe inside for breathing.

32
Treatment Techniques Basic treatment technique: for the majority:
Two lateral and one lower anterior fields. First including the spinal cord in phase I and then off cord for phase II.

33
Overlapping Region Problem
WHY IT’S A PROBLEM? The lateral fields diverge caudally in the anterior neck and the anterior neck diverge cephalade in the lateral.

35
Ways To Solve this Overlap
Lateral field project caudally in the supraclavicular field Supraclavicular field project cranially in the lateral field.

36
Ways To Solve this Overlap
Method1: Midline spinal cord block in the anterior supraclavicular field. Against: Can not be done when anterior structures should be included in the field.

37
Why narrower? Narrower to avoid covering lower jugular nodes.
Take care the shadow should be adequately covering the cord (take care of the projection

38
Ways To Solve this Overlap
Method 2: Gap between two fields calculated by : ½ field1 length x depth/SSD + ½ field2 length x depth/SSD Against: High uncertainty.

39
Ways To Solve this Overlap
Method 3: Put a block over the spinal cord at the posterior inferior angle of the lateral field. Against: Difficult set-up. Still there is lateral and anterior overlap

40
Still there is overlap in the lateral and anterior soft tissues
Still there is overlap in the lateral and anterior soft tissues? How can you solve it?

42
When We can not use this block?
Still there will be overlap in the lateral and anterior soft tissue Extensive lymphadenopathy or high risk of posterior cervical node involvement.(nasopharynx)
")
44
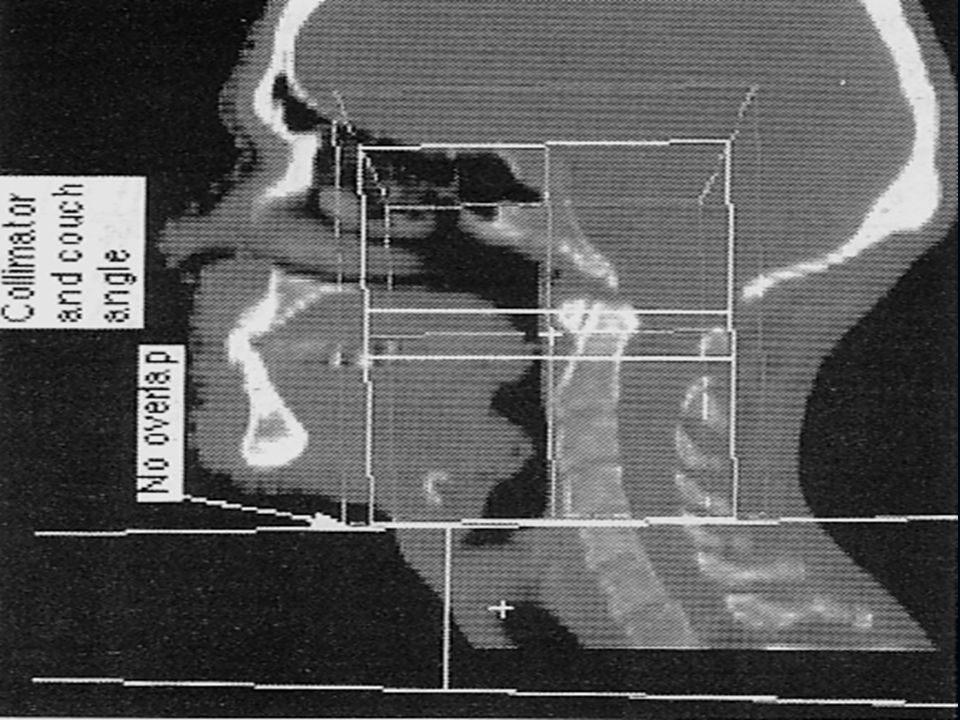
Ways To Solve this Overlap
Method 4: Use Collimator and Couch angle. Against: Time consuming (table move only from inside the room). Errors in movement.
. Errors in movement.")
46
Anterior neck field Lateral head and neck field Overlap region

47
Overlap region corrected

49
Overlap region

50
Overlap region corrected

55
Ways To Solve this Overlap
Method 5: Turn the couch 90 degree and move the gantry accordingly.. Against: Time consuming (table move only from inside the room), errors in movement.
, errors in movement.")
56
???
58
Tracheostomy Problems
Site of recurrence : 10% risk. No tissue, dose may be higher on the spinal Cord. Need a doughnut bolus to avoid suffocation.

59
HAVE FUN!! :)
")
60
Clothes Clamp

61
Clothes Clamp Another use?

62
How Can You Determine the Energy for Electron beam
Spinal Cord Separation=12cm Take care for neck asymmetry

63
Portal Arrangements Opposed –lateral photon fields, with the patient immobilized in supine position are used for treatment of most cancers : oral cavity, Larynx, pharynx. Superior border: Determined by the location of the known disease and likely spread pattern. Whenever possible avoid : Optic pathways, part of the TMJ and auditory canal from the portals. In General: Either it will be 1- At the base of skull when we want to include the retropharyngeal node, e.g. Hypopharynx. 2- Above base when the site is already in the base, e.g. nasopharynx. 3- Just safety margin above the tumor (Larynx).
.")
64
Superior border: Nasopharynx Hypopharynx Oropharynx Oral cavity:
Larynx Above skull base. because the primary at skull base. Skull base? Retropharyngeal nodes Skull base? Primary at skull base. Do you want lymph node? So skull base/If not take only a margin (1 to 2 cm). Glottic? Above the glottis. Supraglottic? Lymph nodes so skull base. Subgltic (very rare) only margin above the larynx. Glottic with extensive supra? Skull base.
. Glottic Above the glottis. Supraglottic Lymph nodes so skull base. Subgltic (very rare) only margin above the larynx. Glottic with extensive supra Skull base.")
65
PLEASE DON’T CUT IN A NODE OR A TUMOR
Lower border: Ask this question: can I protect the larynx? PLEASE DON’T CUT IN A NODE OR A TUMOR YES NO Put your border above the arytenoid (below hyoid bone) Put your as low as possible
 Put your as low as possible.")
66
Lower border (ctn): It is desirable to exclude the larynx from the field from the lateral field when this setup does not compromise the target. How? Lower border of the lateral fields is placed just superior to the arytenoids (below hyoid bone). In patient who can hyperextend his neck an asymmetric jaw (half beam block), can be used. If the patient can not hyperextend the neck, use a slanting inferior border (by collimation), to avoid matching at the sloping submental area. When the larynx can not be excluded the lower border is placed as low as possible, at the neck shoulder junction.
. In patient who can hyperextend his neck an. asymmetric jaw (half beam block), can be used. If the patient can not hyperextend the neck, use a slanting inferior border (by collimation), to avoid matching at the sloping submental area. When the larynx can not be excluded the lower border is placed as low as possible, at the neck shoulder junction.")
67
? Take care Portal Arrangements Anterior border:
Covering skin over the larynx. Margin anterior to the tumor or its site. ? Take care not with: tumor extend to anterior subcutaneous tissue, large submandibular nodes, jugular lymph nodes are present, Surgical scar? Extracapsular extension A strip of the anterior midline skin is usually spared whenever possible to minimize lymph-drainage impairment after irradiation.

68
Group I: Low risk: 20%. T1 Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa

69
Group II Intermediate risk 20–30% T1: Soft palate, pharyngeal wall, supraglottic larynx, tonsil T2: Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa

70
Goup: III High risk>30%
T1–T4Nasopharynx, pyriform sinus, base of tongue. T2–T4: Soft palate, pharyngeal wall, supraglottic larynx, tonsil . T3–T4: Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa.

71
Posterior border: If N0 with low risk of subclinical spread to the posterior cervical nodes, the posterior border is placed behind the insertion of the sternomastoid. If N+ cases or primary tumors with substantial spread to the posterior cervical nodes, posterior border placed behind the spinous process or with good safety margin to the

75
SHOWER?? NO evidence that taking shower will increase the skin reaction!!. IF you can let your patient take a shower in the day before his replanning day. And in patients tattooed.

76
To Summarize Nasopharynx, oropharynx, or Oral Cavity the junction should be made above the thyroid notch (thus the anterior spinal cord shield protect the larynx as well). In the hypopharynx and the larynx we avoid midline shield.
. In the hypopharynx and the larynx we avoid midline shield.")
77
3D CRT IN HEAD AND NECK CANCER
How to define and delineate your target volume

78
How to Approach your Patient
Ask yourself the following questions: 1-Where is the tumor?. 2- Is there is any Lymph nodes? 3- If No Lymph nodes is it a site rich in lymphatic?. 4- What’s the role of surgery: - resectable? 5- Lymph nodes dissected or Not?

79
Early stage Disease Surgery Vs Radio and Chemo.
How to decide? If functional outcome is better with CRT go for it if not ! Go for Surgey. TAKE CARE!!! Not only ChemoRT but good ChemoRT.

80
Late Stages T3-T4 Usually Surgery first if resectable.
You still can Try CRT if organ preservation is required. (provided salvage surgery may still be an option. e.g. patient reliable for good follow-up. Surgeon reliable for good surgery. Famous Laryngeal preservation trials: Veterans Affairs (larynx neoadjuvant), EORTC (Hypopharynx neoadjuvant), (RTOG larynx Concurrent CRT value). Recently Urba et al JCO 2006(NEW is the use of concurrent CRT if good response to the neoadjuvant treatment. Veterans affair NEMJM 1991, EORTC JNCI 1996, RTOG NEJM 2003, Urba et al 2006
, EORTC (Hypopharynx neoadjuvant), (RTOG larynx Concurrent CRT value). Recently Urba et al JCO 2006(NEW is the use of concurrent CRT if good response to the neoadjuvant treatment. Veterans affair NEMJM 1991, EORTC JNCI 1996, RTOG NEJM 2003, Urba et al")
81
Organs At Risk (OARs) Chiasma: 50-52 Optic Nerves: 50- 52
Eyes (Lens) : 10Gy Spinal Cord: 5cm: 50Gy, 10 cm: 50 , 20cm: 45Gy Brain Stem: 60Gy but 2/3: 53Gy whole 50Gy. Brachial plexus: 60Gy. Salivary Glands: situlation 26Gy, without 23Gy, complete loss of function 32Gy. (TD5/5 Emami et al 1991) TD5/5 emami et al 1991.
 : 10Gy. Spinal Cord: 5cm: 50Gy, 10 cm: 50 , 20cm: 45Gy. Brain Stem: 60Gy but 2/3: 53Gy whole 50Gy. Brachial plexus: 60Gy. Salivary Glands: situlation 26Gy, without 23Gy, complete loss of function 32Gy. (TD5/5 Emami et al 1991) TD5/5 emami et al")
82
Computer Tomography with or without MRI fusion

83
Toxicity Hypogeusia. Ageusia. Dysgeusia.
Dysgeusia: change of normal taste

87
Target Volume Delineation

88
ANATOMIE

90
Lymphatic System Basic Anatomical Consideration:
- Well lateralized tumor spread to ipsilateral L.N. Midline tumors may spread to both sides. Patients with huge L.N (N3) may have contralateral L.N. (lymphatic obstruction leads to Lymph shunts). Which parts in head and neck has very little incidence of lymphatic spread? Middle ear, Vocal Cord, PNS???. Head and neck contain around 30% of all lymphatic vessels and Lns.
 may have contralateral L.N. (lymphatic obstruction leads to Lymph shunts). Which parts in head and neck has very little incidence of lymphatic spread Middle ear, Vocal Cord, PNS . Head and neck contain around 30% of all lymphatic vessels and Lns.")
91
Risk of Lymph node involvement depends on: 1- T stage.
2- Lymphatic invasion (in biopsy). 3- Degree of differentiation. I Low risk<20 T1Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa
. 3- Degree of differentiation. I Low risk<20 T1Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa.")
92
Group I: Low risk: 20%. T1 Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa

93
Group II Intermediate risk 20–30% T1: Soft palate, pharyngeal wall, supraglottic larynx, tonsil T2:Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa

94
Goup: III High risk>30%
T1–T4Nasopharynx, pyriform sinus, base of tongue. T2–T4: Soft palate, pharyngeal wall, supraglottic larynx, tonsil . T3–T4: Floor of mouth, oral tongue, retromolar trigone, gingiva, hard palate, buccal mucosa.

95
1- Oral Cavity and oropharynx:
a- lateralized. b- Middle line. 2- Larynx and Hypopharynx. 3- Nose, NHH, and Nasopharynx

96
Nasopharynx Target: differ according to treatment phase
Phase I: structures included? GTV1: include mass seen in MRI. GTV2: LNs affected CTV1: nasopharynx proper, sphenoid air sinus, basiocciput, base of skull to include, posterior ethmoids, posterior one third of maxillary antrum, neck nodes (retropharyngeal, posterior cervical , jugular). Lateral and posterior pharyngeal wall to the level of mid tonsillar fossa Never forget: examination, EUA, Dental assessment…..etc.
. Lateral and posterior pharyngeal wall to the level of mid tonsillar fossa. Never forget: examination, EUA, Dental assessment…..etc.")
97
Nasopharynx LOOK HERE CAREFULLY

98
Maxillary Antrum Different position WHY?? HOW??
Eye opened looking forward. If rotating the eye ??. Putting the retina in the high dose region.

99
Maxillary Antrum To include the apex of the maxillary antrum while excluding the eye, the beam can be vertical with the chin extended or the head position can be neutral and the couch rotated 90 degree, the gantry then turned to the appropriate angle The Apex of the antrum is located behind the orbit , so by hyper-extending the neck you re bringing the apex below the orbit.

100
Maxillary Antrum And PNS
GTV all gross tumor that can be seen in imaging. PTV include: GTV with 2-3 cm margin. Then reduce it to 1-2 cm margin. (this may not fulfill what you need so do it if you don’t know what to do!!). Some centers now include the submandibular and subdigastric L.Ns in patients with Squamous cell or poorly differentiated carcinoma.
. Some centers now include the submandibular and subdigastric L.Ns in patients with Squamous cell or poorly differentiated carcinoma.")
101
Maxiallry Antrum ctn Volume include: Upper border: above Crista galli?
Why? To include the ethmoids. Or Lower edge of the cornea if no orbital infiltration.

102
Lower Border: 1cm below the floor of the sinus.
Medial border: 1-2 cm across the midline to cover the contralateral ethmoid sinus. Lateral border: extend one cm beyond the apex of the sinus. Lateral portal: Anterior border: is anterior to the anterior wall. Posterior border: is behind the pterygoid plates.

103
Maxillary sinus conformal
Volume to be included: 1- Maxillary sinus. 2- Palate. 3- Alveolar ridge. 4- Nasal Cavity. 5- Medial orbit. 6- nasopharunx. 7- pterygopalatine and infratemporal fossae.

105
LETS HAVE SOME PRACTICE
ATLAS CT

106
THANK YOU

Similar presentations