Download presentation
Presentation is loading. Please wait.

1
By: A.RashedM. Assistant Professor of Pediatric Dentistry
Eruption By: A.RashedM. Assistant Professor of Pediatric Dentistry

2
How eruption happens?! Elongation of tooth root
Forces exerted by vascular tissues around the tooth Hormonal influnces Alveolar crest resorption Growth and pull of periodontal membrane …

3
Eruption and tooth development.
1. the crown cal. Completes the tooth begins its migration 2. 2/3 of root cal. Completes the tooth emerges into soft tissue 3. ¾ of root cal. Completes the tooth emerges into oral cavity

4
Why does emergence of teeth happen at different times?

5
Eruption?! Emergence?!

6
Problems associated with eruption in primary teeth
Illingworth and Tasanen study: YES NO Daytime restlessness Infection Finger sucking Temperature rise Rubbing of the gum Diarrhea Increase in drooling Coughing Some loss of appetite Sleep disturbances

7
What if signs not related to eruption be mistaken as eruption signs?!

8
What can we do to releive pain and difficulty?

9
What is this?! why does it happen? Treatment?

10
Shedding of primary teeth, eruption of permanent teeth

11
Overretained primary teeth
why may primary teeth over retain? How should they be treated?

12
What do you see? What should we do?

13
What do you see? What should we do?

14
What do you see? What should we do?

15
Ankylosis infraocclusion

16
Are all ankylosed teeth, necessarily infraoccluded?

17
Are all infraoccluded teeth, necessarily ankylosed?

18
How can infraocclusion and ankylosis be differentiated?
Radiographs Percussion test

19
What problems may infraoccluded teeth cause?

20
Treatment in primary teeth?
1. With successor 2. Without successor

21
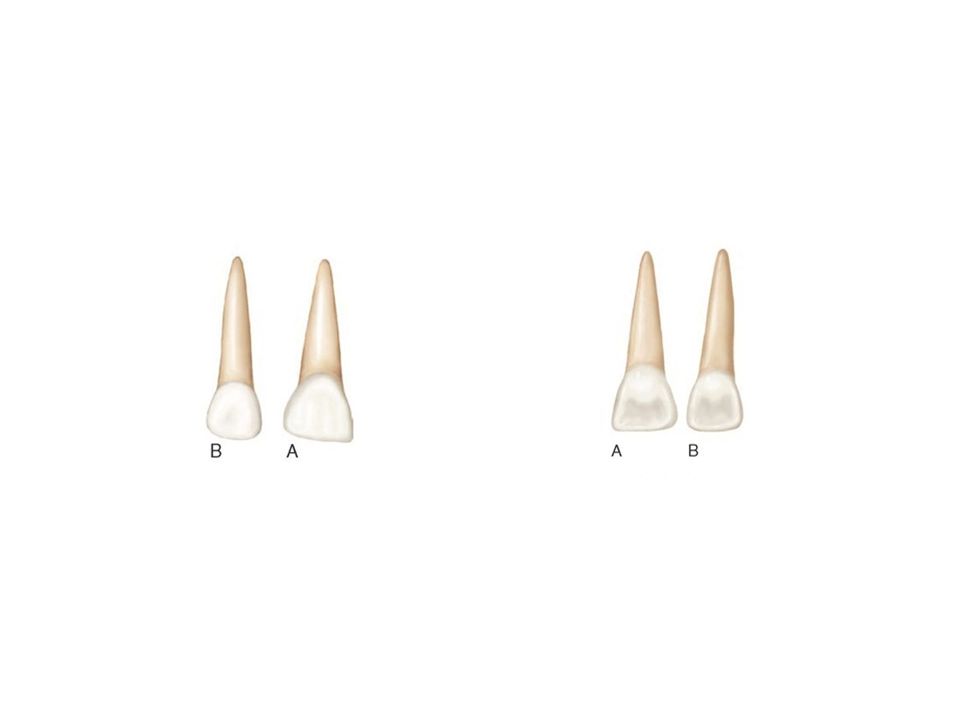
Major contrasts between primary and permanent teeth
Anterior teeth: higher crown width (M-D)/ crown length 2. Anterior teeth: narrower and longer roots with wide crowns (cervical third view)-comparatively- Primary molar: slender and longer roots that flare beyond the outline of the crown –comparatively- There is no trunk, each root directly comes from the crown 4. More prominent cervical ridge: buccal, lingual, labial 5. Primary molar: more slender at their cervical portion mesiodistally (bulby)
/ crown length. 2. Anterior teeth: narrower and longer roots with wide crowns (cervical third view)-comparatively- Primary molar: slender and longer roots that flare beyond the outline of the crown –comparatively- There is no trunk, each root directly comes from the crown. 4. More prominent cervical ridge: buccal, lingual, labial. 5. Primary molar: more slender at their cervical portion mesiodistally (bulby)")
22
Major contrasts between primary and permanent teeth
6. Primary molar: : buccal and lingual surfaces are flatter which result in a narrower occlusal surface (bulby) 7. Primary molars: Buccal cervical ridges are much more pronounced especially ‘D’ Less pigmentation, and whiter 9. The pulp chamber is relatively larger in all dimensions, pulp horns are high 10. The enamel is relatively thin, the dentine thickness is limited 11. Primary teeth are smaller than permanent teeth
 7. Primary molars: Buccal cervical ridges are much more pronounced especially ‘D’ Less pigmentation, and whiter. 9. The pulp chamber is relatively larger in all dimensions, pulp horns are high. 10. The enamel is relatively thin, the dentine thickness is limited. 11. Primary teeth are smaller than permanent teeth.")
31
Lunch and sleep!

Similar presentations









. All rights reserved. No part of this product may be reproduced or transmitted in any.>")
















