Download presentation
Presentation is loading. Please wait.

1
Pharmacologic Treatment Considerations for the Obese Patient
Shala Swarm, FNP-BC Cheyenne Regional Medical Center Cheyenne Physician’s Group Weight Loss Center

2
No Disclosures

3
Objectives Identify three major Health Effects Obesity causes for patients and importance of addressing and treating obesity Select at least one treatment option for obesity for patients with major health conditions

4
Metropolitan Life Insurance Table
Ideal Body and BMI Ideal Body Weight Metropolitan Life Insurance Table Method to Calculate Women = 100 lbs for 5’0” + 5 lbs for each add. inch /- 10% Men = 110 lbs for 5’0” + 5 lbs for each add. Inch +/- 10% Body Mass Index Height to Weight Ratio Method to Calculate BMI = Weight (pounds) X 703 Height x Height (inches)
 X 703. Height x Height. (inches)")
5
Ideal Body Weight Charts
TABLE METROPOLITAN HEIGHT AND WEIGHT TABLE According to Frame, Ages MEN Weight in Pounds (In Indoor Clothing)* TABLE METROPOLITAN HEIGHT AND WEIGHT TABLE According to Frame, Ages 25-59 WOMEN Weight in Pounds (In Indoor Clothing)* HEIGHT SMALL MEDIUM LARGE (In Shoes)+ FRAME Feet Inches 5 2 3 4 6 7 8 9 10 11 1 HEIGHT SMALL MEDIUM LARGE (In Shoes)+ FRAME Feet Inches 4 10 11 5 1 2 3 6 7 8 9 Indoor clothing weighing 5 pounds for men and 3 pounds for women Shoes with 1-inch heels Source of basic data Build Study, Society of Actuaries and Association of Life Insurance Medical Directors of America, Copyright© 1996, 1999 Metropolitan Life Insurance Company Courtesy of the Metropolitan Life Insurance Company.
* TABLE METROPOLITAN HEIGHT AND WEIGHT TABLE According to Frame, Ages WOMEN Weight in Pounds (In Indoor Clothing)* HEIGHT. SMALL. MEDIUM. LARGE. (In Shoes)+ FRAME. Feet. Inches HEIGHT. SMALL. MEDIUM. LARGE. (In Shoes)+ FRAME. Feet. Inches Indoor clothing weighing 5 pounds for men and 3 pounds for women. Shoes with 1-inch heels. Source of basic data Build Study, Society of Actuaries and Association of Life Insurance Medical Directors of America, Copyright© 1996, 1999 Metropolitan Life Insurance Company Courtesy of the Metropolitan Life Insurance Company.")
7
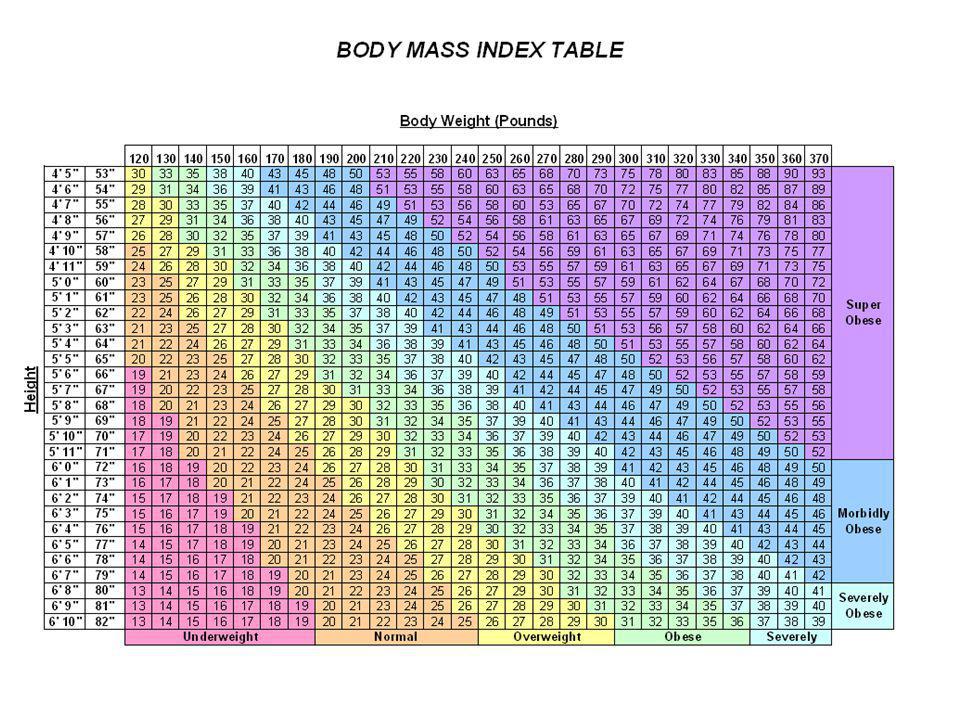
Definitions of Overweight and Obesity
Normal Range – BMI Overweight – BMI Obese – BMI Severe Obese – BMI Morbid Obese – BMI Super Obese – BMI > 50 BMI is limited due to body frame

8
Obesity is a Growing Concern

9
Obesity Trends* Among U.S. Adults BMI > 30

10
Obesity Trends* Among U.S. Adults

11
Obesity Trends* Among U.S. Adults

12
Obesity Trends* Among U.S. Adults

13
Obesity Trends* Among U.S. Adults
We have never had an epidemic like this that we have been able to track so thoroughly and see. As I told you, this is conservative. About 60 million adults, or 30 percent of the adult population, are now obese, which represents a doubling of the rate since 1980.

14
Obesity Trends* Among U.S. Adults
We have never had an epidemic like this that we have been able to track so thoroughly and see. As I told you, this is conservative. About 60 million adults, or 30 percent of the adult population, are now obese, which represents a doubling of the rate since 1980.

15
Statistics US 33.8 % or one-third of the population Wyoming
Resource: CDC Wyoming In 2010 was: 25.1 % Resource: CDC World Worldwide obesity has more than doubled since 1980. In 2008, 1.5 billion adults, 20 and older, were overweight. Of these over 200 million men and nearly 300 million women were obese. 65% of the world's population live in countries where overweight and obesity kills more people than underweight. Resource: World Health Organization

16
Risks of Obesity

17
Co-Morbid Medical Conditions
Diabetes Hypertension Hyperlipidemia Cardiac Disease Sleep Apnea / Hypoventilation Liver disease Cancer risk Heartburn Asthma Osteoarthritis Depression Urinary Incontinence Menstrual Irregularity Infertility Leg Swelling Right side are potentially life threatening problems. Diabetic- tissues are insulin resistant

18
Complications of morbid obesity are LETHAL
4 Morbidly obese: die 10 to 15 years earlier 3 Mortality Ratio 2 1 Risk of Death is Exponential in the Morbidly Obese 20 25 30 35 40 Body Mass Index Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003; 289:

19
What Causes Obesity Environment ??? Genetics??? Takes many years
Decreased Mobility due to increased access Fast Food Video Games Sedentary Jobs Genetics??? Takes many years to these dramatic changes

20
Genetic Weight gain Environment
Weight Gain Cycle Genetic Weight gain Environment Appetite cravings reduced energy expenditure Co-morbid disease Natural history is progressive. BMI= 40 something changes. Satiety changes, full but not satisfied. Metabolic Hormonal

21
Other Causes Medications: Anti-psychotics Anti-depressants
Anti-epileptic's Steroids Diabetes meds Birth Control medications

22
Other Causes Health Conditions Endocrine Disorders Hormonal Disorders
Sleep Apnea Diabetes Orthopedic Injuries

23
WHAT DO YOU DO WITH THESE PATIENTS?
How do you treat them? Treat as in attitude Treat as is treatment

24
Goals Long term vs Short term Realistic
Small weight reduction can make a big difference A good starting goal is 10% weight loss 10% weight loss can make a big impact on multiple health conditions Prevent more weight gain

25
Treatment Options Screening Tests Diet Exercise
Psychological Evaluations Medications Surgery

26
Screening History Physical Exam EKG Special Measurements and Tests
Labs CBC CMP Thyroid Panel (TSH, free T3, free T4) Lipid Profile UA Fasting Insulin, 2 hour post-prandial glucose 25 (OH) D levels History should include diet history (eating disorders), weight gain history, lifestyle behaviors (eating out, schedules), what do they feel are their “bad” habits (snack at certain times of the day, ect. Exercise habits PMH and medications (may give clue to weight problems) Sleep Habits Physical Exam should include Skin Extra Measurements: BCA, body fat %, Waist Circ, neck size, body shape
 Lipid Profile. UA. Fasting Insulin, 2 hour post-prandial glucose. 25 (OH) D levels. History should include. diet history (eating disorders), weight gain history, lifestyle behaviors (eating out, schedules), what do they feel are their bad habits (snack at certain times of the day, ect. Exercise habits. PMH and medications (may give clue to weight problems) Sleep Habits. Physical Exam should include. Skin. Extra Measurements: BCA, body fat %, Waist Circ, neck size, body shape.")
27
Diet Calorie – a way to measure energy Calories in = Calories out 1 Calorie = 1 kilocalorie = 1000 calories

28
Diet Basal Metabolic rate (BMR) + Thermic effect of food (TEF)
The energy used to sustain life (breathing, cell functions) + Thermic effect of food (TEF) Energy used to digest food Activity Thermogenesis (AT) Energy used during exercises and activities of daily living (NEAT)
 + Thermic effect of food (TEF) Energy used to digest food. Activity Thermogenesis (AT) Energy used during exercises. and activities of daily living (NEAT)")
29
Diet BEE calculation (Harris-Benedict estimation)
BEE Females = (9.563 * Weight) + (1.85 * Height) - (4.676 * Age) BEE Males = (13.75 * Weight) + (5.003 * Height) - (6.775 * Age)
 + (1.85 * Height) - (4.676 * Age) BEE Males = (13.75 * Weight) + (5.003 * Height) - (6.775 * Age)")
30
Diet Factors that Alter Metabolic Rate
Body Composition (leaner have higher BMR) Age Growth Hormones Stress Temperature Changes Fasting Dieting Caffeine, Alcohol, and Smoking
 Age. Growth. Hormones. Stress. Temperature Changes. Fasting. Dieting. Caffeine, Alcohol, and Smoking.")
31
Diet Increasing Metabolism Regular Eating Habits Exercise
Increasing muscle mass

32
Diet Food Label RDA vs DV – Serving Size and amount per container
DV is a % based on a 2000 calorie diet RDA is recommended daily allowance (guidelines to promote optimal health to prevent deficiencies) These are not on the food label. Serving Size and amount per container Calories Protein Sugars Dietary Fiber 5%, 10%, 20% as low, moderate, high Think what you what high % and low %
 These are not on the food label. Serving Size and amount per container. Calories. Protein. Sugars. Dietary Fiber. 5%, 10%, 20% as low, moderate, high. Think what you what high % and low %")
33
Diet Protein 4 kcal/gm Carbohydrates 4 kcal/gm Fat 9 kcal/gm
DRI: 0.8gm/kg of IBW (Increased amounts needed to protect lean body mass in restricted calorie diets) Growth and repair of body tissues Sources: meat, fish, legumes, dairy, peanuts Carbohydrates 4 kcal/gm DRI: 130 gm/day Energy Source Sources: grains, fruits, vegetables Fat 9 kcal/gm Acceptable Ranges: 20-35% of daily kcal Helps with digestion and absorption of fat soluble vitamins Saturated, Monounsaturated, Polyunsaturated and Essential Alcohol 7 kcal/gm No nutrient value *DRI – Dietary References Intake Sat. Fat – no double bonds Mono fat – 1 double bond Poly fat – 2 or more double bonds
 Growth and repair of body tissues. Sources: meat, fish, legumes, dairy, peanuts. Carbohydrates 4 kcal/gm. DRI: 130 gm/day. Energy Source. Sources: grains, fruits, vegetables. Fat 9 kcal/gm. Acceptable Ranges: 20-35% of daily kcal. Helps with digestion and absorption of fat soluble vitamins. Saturated, Monounsaturated, Polyunsaturated and Essential. Alcohol 7 kcal/gm. No nutrient value. *DRI – Dietary References Intake. Sat. Fat – no double bonds. Mono fat – 1 double bond. Poly fat – 2 or more double bonds.")
34
Diet Keys to Success Portions
Planning Ahead (meal planning and spacing of meals) Protein Conscious Eating Liquid Calories vs Solid Food Water Intake Conscious Eating – fullness vs hunger and eating away from distractions
 Protein. Conscious Eating. Liquid Calories vs Solid Food. Water Intake. Conscious Eating – fullness vs hunger and eating away from distractions.")
35
Diets Types of Diets VLCD (very low calorie diets – 400-800 cal/day)
LCD (low calorie diets – cal/day) Self Directed (Weight Watchers, Atkins)
 Self Directed (Weight Watchers, Atkins)")
36
Diet VLCD Medically Supervised
The lower the calories, the higher the protein needed (1.2 g/kg women, 1.5 g/kg men) Short term Vitamin Supplementation Side Effects: GI, electrolyte, gout, psych, skin, neurological Contraindications: many Medically Supervised: electrolytes frequently, EKG every 30 pounds, weekly visits Wadden et al study showed no greater long-term weight loss than LCD Contraindications: Absolute- T1DM, epilepsy, arrhythmias, recent MI, psychosis, substance abuse, pregnancy or lactation, medical diseases that is unstable Relative – CHf, TIAs, DVT, NSAIDS, psych, under 16 years SE: fatigue, cold intol., hair falling out, nutrient deficiencies Not long term use
 Short term. Vitamin Supplementation. Side Effects: GI, electrolyte, gout, psych, skin, neurological. Contraindications: many. Medically Supervised: electrolytes frequently, EKG every 30 pounds, weekly visits. Wadden et al study showed no greater long-term weight loss than LCD. Contraindications: Absolute- T1DM, epilepsy, arrhythmias, recent MI, psychosis, substance abuse, pregnancy or lactation, medical diseases that is unstable. Relative – CHf, TIAs, DVT, NSAIDS, psych, under 16 years. SE: fatigue, cold intol., hair falling out, nutrient deficiencies. Not long term use.")
37
Diet LCD Medically Supervised More compliance Weekly Visits
Done by portion control, low-fat, low-carb, or calorie counting

38
Protein and Weight Loss
Diet Protein and Weight Loss Changes Body Composition by decreasing body fat but protects lean tissue mass (protein synthesis in muscles and burning of calories) Stabilizes Blood Sugars (insulin levels) Satiety Reference: Layman Insulin is primary growth hormone Lose more weight rapidly, but long term may be similar results to WW
 Stabilizes Blood Sugars (insulin levels) Satiety. Reference: Layman. Insulin is primary growth hormone. Lose more weight rapidly, but long term may be similar results to WW.")
39
Diet Protein Diets – Safety and Monitoring UA Vitamins Multi-vitamin
Calcium if needed Vitamin D Fish Oil UA to check for ketones

40
Physical Activity Exercise – planned activity
NEAT (non-exercise activity thermogensis) Daily Activities
 Daily Activities.")
41
Exercise Aerobic or Cardiovascular Uses fatty acids for fuel
Cardiovascular fitness Long bursts of activities Oxygen dependant (breakdown of ATP) Anaerobic or Resistance Intracellular glycogen as fuel Improves lean body mass Oxygen independent (lactic acid build-up) Reference: Williams Circulation 2007
 Anaerobic or Resistance. Intracellular glycogen as fuel. Improves lean body mass. Oxygen independent (lactic acid build-up) Reference: Williams Circulation")
42
Exercise Preventing Injury Warm up and cool down and stretching
Always warm up before stretching (optional) Cool down (below target heart rate level) then stretch Body Recovery (resistance needs rest day) Interval Training (not everyday) Use guide – ACSM’s Guidelines for Exercise Testing Interval training pushes body into anaerobic phase and will get more lactic acid Need light day on “rest day”
 Cool down (below target heart rate level) then stretch. Body Recovery (resistance needs rest day) Interval Training (not everyday) Use guide – ACSM’s Guidelines for. Exercise Testing. Interval training pushes body into anaerobic phase and will get more lactic acid. Need light day on rest day")
43
Psychological Evaluation
Eating Disorders Emotional Eating (depression) Stress Eating Patterns Being Overweight “protecting” patient Support Systems
 Stress. Eating Patterns. Being Overweight protecting patient. Support Systems.")
44
Meds, Meds, and more Meds

45
Medications Most are short term use only (but obesity is chronic)
Safety Addiction Cost **ALL MEDICATIONS NEED TO BE USED WITH BEHAVIORAL MODIFICATIONS OR THEY WILL NOT BE EFFECTIVE** Contraindications for most HTN, arteriosclerosis, hyperthyroidism, glaucoma, drug abuse hx, anti-depressants, seizures, pregnancy and lactation

46
Medications Regulatory Challenges Efficacy Safety
Benefit-risk evaluation History of obesity medications Perception Regulatory Challenges article How long should trials be?

47
Medications History of Obesity Medications
Drug Year Approved Year Removed Short Term Use Desoxyephedrine 1947 ?????? Phenmetrazine 1956 Phentermine 1959 Still On Market Diethylpropion Phendimetrazine Benzphetamine 1960 Mazindol 1973 Fenfluramine 1997 Long Term Use Dexfenfluramine 1996 Sibutramine 2010 Orlistat 1999

48
Medications Ephedrine (available as a restricted prescription medication) Phentermine (FDA approved 1957) Diethylpropion Phendimetrazine Benzphetrazine Xenical Merida (pulled off market fall 2010)
")
49
Medications Ephedrine Dose Range 12.5-75 mg/day
Norepinephrine releaser Used mainly for hypotension and bronchospasms Ephedra was herbal form that was banned in 2004 Side Effects: tremors, nervousness, insomnia, increase HR and BP Cautions/Contraindications: MAOI, breastfeeding, hyperthyroidism, CAD, HTN, arrhythmias, CV disease, DM, glaucoma, seizures, renal impairment, prolonged use

50
Medications Phentermine Phentermine HCL (Adipex-P, Fastin)
Phentermine Resin (Ionamin) Dose mg/day CNS Stimulate Side Effects: palpitations, tachycardia, HTN, insomnia, dizziness, euphoria, tremors, HA, pulmonary HTN, valvular heart disease, irritability Cautions/Contraindications: CV disease, pregnancy and lactation, HTN, hyperthyroidism, glaucoma, agitation, drug abuse, DM Most commonly Rx anerotic med
 Dose mg/day. CNS Stimulate. Side Effects: palpitations, tachycardia, HTN, insomnia, dizziness, euphoria, tremors, HA, pulmonary HTN, valvular heart disease, irritability. Cautions/Contraindications: CV disease, pregnancy and lactation, HTN, hyperthyroidism, glaucoma, agitation, drug abuse, DM. Most commonly Rx anerotic med.")
51
Medications Diethylpropion (Tenuate) Dose Range: 25-75 mg/day
Similar to bupropion chemically Side Effects: tachycardia, HTN, pulmonary HTN, valvular heart disease, seizures, psychosis, hallucinations, leukopenia, constipation, dry mouth, N/V, diarrhea, abdominal discomfort, anxiety, dizziness, HA, insomnia, arrhythmias, palpitations Caution/Contraindications: pulmonary HTN, HTN, arteriosclerosis, hyperthyroidism, glaucoma, agitations, drug abuse, valvular hear disease, heart murmur, CV disease, seizure disorder, psychiatric disorder Should be 2nd consideration

52
Medications Phendimetrazine (Bontril) Dose Range: 35-105 mg/day
Mechanism of action unknown, CNS stimulant Side Effects: tachycardia, HTN, pulmonary HTN, restlessness, agitation, tremor, flushing, sweating, blurred vision, constipation, nausea, diarrhea, gastric pain, anxiety, dizziness, HA, insomnia, palpitations, urinary frequency Caution/Contraindications: pulmonary HTN, HTN, arteriosclerosis, hyperthyroidism, glaucoma, agitation, drug abuse, valvular hear disease, heart murmur, CV disease, DM

53
Medications Benzphetamine (Didrex) Dose Range: 25-50 mg/day
Mechanism of action unknown, CNS stimulant Side Effects: psychosis, tachycardia, HTN, cardiomyopathy, cardiac ischemia, restlessness, agitation, tremor, flushing, sweating, constipation, nausea, diarrhea, dizziness, HA, dry mouth, insomnia, unpleasant taste, palpitations, urinary frequency Caution/Contraindications: HTN, arteriosclerosis, hyperthyroidism, glaucoma, agitation, drug abuse, valvular hear disease, heart murmur, CV disease, DM, arrhythmias

54
Medications Xenical (Orlistat, Alli) Dose Range: 60-120 mg TID
Mechanism of action: inhibits gastric and pancreatic lipases, reducing fat absorption Side Effects: angioedema, fat-soluble vitamin deficiency, hepatotoxicity; oily spotting flatus with discharge, fecal urgency, fatty stools, oily evacuation, fecal incontinence, URI, influenza, HA, abdominal pain, back pain, nausea, menstrual irregularities, UTI, fatigue, arthritis, rectal pain, dizziness, infectious diarrhea Caution/Contraindications: malabsorption syndromes, cholestasis, eating disorders Kidney and Pancreas problems??? Arch Intern Med. 2011 Apr 11;171(7): Orlistat and acute kidney injury: an analysis of 953 patients.
: Orlistat and acute kidney injury: an analysis of 953 patients.")
55
Medications Off Label Use Antidepressants Insulin Sensitizers
Anti-Seizures Combination Therapy 5-HTP / Carbidopa

56
5-HTP = 5-hydroxytryptophan
Medications 5-HTP = 5-hydroxytryptophan Increases the production of serotonin Over the counter Wide margin of safety Not been associated risk for serotonin syndrome Does not alter cardiovascular parameters Rapidly Metabolized by peripheral decarboxylase High Doses are needed to increase brain 5-HT since it is rapidly metabolized by peripheral decarboxylase (intestine, kidney, blood, liver)
")
57
5-HTP = 5-hydroxytryptophan
Medications 5-HTP = 5-hydroxytryptophan Other Uses: anxiety, depression, alcohol withdrawal, headaches Side Effects: anorexia, diarrhea, dizziness, drowsiness, eosinophilia, flatulence, N/V, somnolence, palpitations, insomnia, hypomania, stomach pain, taste disturbance, weight gain Avoid Use: eosinophilia syndromes, MAOI use, mitochondrial encephalomyopathy Caution in: antidepressant use, down syndrome, GI disorders, platelet disorders, psychiatric disorder history, PUD, renal disease

58
Medications Antidepressants
SSRI (selective serotonin reuptake inhibitors) – Increase 5-HT (serotonin) in the satiety center and down regulate 5-HT2A auto-receptors which increase 5-HT (serotonin) secretion Side Effects: dry mouth, insomnia, nausea, tremor, headache, sweating, decreased libido, Serotonin Syndrome Weight Loss Success: Limited results, but may be helpful for emotional eating or night time eating syndrome (sertraline) Article in Obesity Research Nov 1995 showed some effectiveness of fluoxetine and weight loss. A study by Stunkard et al in J Clin Psychiatry 2006 confirmed sertraline and NES.
 – Increase 5-HT (serotonin) in the satiety center and down regulate 5-HT2A auto-receptors which increase 5-HT (serotonin) secretion. Side Effects: dry mouth, insomnia, nausea, tremor, headache, sweating, decreased libido, Serotonin Syndrome. Weight Loss Success: Limited results, but may be helpful for emotional eating or night time eating syndrome (sertraline) Article in Obesity Research Nov 1995 showed some effectiveness of fluoxetine and weight loss. A study by Stunkard et al in J Clin Psychiatry 2006 confirmed sertraline and NES.")
59
Medications Antidepressants
Bupropion (Wellbutrin) – Inhibits neuronal uptake of norepinephrine and dopamine Chemically like diethylpropion Side Effects: dry mouth, headache, agitation, nausea, dizziness, constipation, tremor, sweating, abnormal dreams, insomnia, tinnitus, diarrhea, abdominal pain, anxiety Weight Loss Success: Can decrease appetite and cravings Article by Anderson, James et al in Obes Research 2002 showed 7.2% weight loss at 24 weeks and 10.1% sustained weight loss at 48 weeks.
 – Inhibits neuronal uptake of norepinephrine and dopamine. Chemically like diethylpropion. Side Effects: dry mouth, headache, agitation, nausea, dizziness, constipation, tremor, sweating, abnormal dreams, insomnia, tinnitus, diarrhea, abdominal pain, anxiety. Weight Loss Success: Can decrease appetite and cravings. Article by Anderson, James et al in Obes Research 2002 showed 7.2% weight loss at 24 weeks and 10.1% sustained weight loss at 48 weeks.")
60
Medications Insulin Sensitizers Metformin (Glucophage)
Indicated for Diabetes Type 2 Mechanism of Action: decreases hepatic glucose production and intestinal glucose absorption; increases insulin sensitivity and peripheral glucose uptake Side Effects: nausea, diarrhea, flatulence, anorexia, headache, metallic taste

61
Medications Insulin Sensitizers Byetta (exenatide)
Victoza (liraglutide) Indicated for Diabetes Type 2 Mechanism of Action: activates glucagon-like-peptide-1 (GLP-1) receptor, increasing insulin secretion, decreasing glucagon secretion, and delaying gastric emptying (incretin mimetic) Side Effects: nausea, vomiting, diarrhea, nervousness, dizziness, headache, dyspepsia, decreased appetite Liraglutide contraindicated in pancreatitis and thyroid carcinoma
 Indicated for Diabetes Type 2. Mechanism of Action: activates glucagon-like-peptide-1 (GLP-1) receptor, increasing insulin secretion, decreasing glucagon secretion, and delaying gastric emptying (incretin mimetic) Side Effects: nausea, vomiting, diarrhea, nervousness, dizziness, headache, dyspepsia, decreased appetite. Liraglutide contraindicated in pancreatitis and thyroid carcinoma.")
62
Anti-Seizure Medications
Topiramate (Topamax) Indicated for Seizures and Migraine headaches Mechanism of Action: modulated GABA-A receptors, weak caronic anhydrase inhibitor, exhibits state-dependent bloackade of voltage- dependant Na and Ca channels Side Effects: dizziness, parathesias, fatigue, difficulty concentrating, somnolence, weight loss, nervousness, ataxia, diarrhea, nausea, nystagmus, tremor, fever, taste changes, taste changes, myopia, nephrolithiasis Contraindications: increased intraocular pressure
 Indicated for Seizures and Migraine headaches. Mechanism of Action: modulated GABA-A receptors, weak caronic. anhydrase inhibitor, exhibits state-dependent bloackade of voltage- dependant Na and Ca channels. Side Effects: dizziness, parathesias, fatigue, difficulty concentrating, somnolence, weight loss, nervousness, ataxia, diarrhea, nausea, nystagmus, tremor, fever, taste changes, taste changes, myopia, nephrolithiasis. Contraindications: increased intraocular pressure.")
63
Medications Others for thought Probiotics ??? Antibiotics ???
Vitamin D ??? Vitamin D: vitamin D receptors found on the adipocyte and deficiency of vitamin D allows adipocyte enlargement

64
Medications Combination Therapy Obesity is a chronic medical condition and just like any other chronic medical condition multiple medications are usually necessary to proper control of the health condition. Example: HTN, Diabetes

65
Medications Combined Medications Phentermine + 5-HTP/carbidopa
5-HTP and carbidopa can counteract side effects of phentermine Dual action with NE release (phentermine) and increased 5-HT release Dual mechanism can increase satiety and decrease food craving Dosing Phentermine dosing + compounded 5-HTP / carbidopa 5-HTP = 5-25 mg carbidopa = always 5 mg
 and increased 5-HT. release. Dual mechanism can increase satiety and decrease food craving. Dosing. Phentermine dosing + compounded 5-HTP / carbidopa. 5-HTP = 5-25 mg. carbidopa = always 5 mg.")
66
Combination Medications
Both phentermine and wellbutrin have norepinephrine effects and therefore recommended not to use them together

67
Medications What may be to come
Naltrexone + bupropion (Contrave) – rejected by the FDA in February 2011 (Orexigen) Topiramate + phentermine (Qnexa) – (Vivus) Zonesamide + bupropion (Empatic) – (Orexigen) Pramlintide + metreleptin – Amylin Pharmaceuticals Lorcaserin (expected to be named Lorqess) - Arena Pharmaceuticals Tesofensine - NeuroSearch Liraglutide Exenatide GLP-1 + PYY 3-36 – Emisphere Technologies
 – rejected by the FDA in February 2011 (Orexigen) Topiramate + phentermine (Qnexa) – (Vivus) Zonesamide + bupropion (Empatic) – (Orexigen) Pramlintide + metreleptin – Amylin Pharmaceuticals. Lorcaserin (expected to be named Lorqess) - Arena Pharmaceuticals. Tesofensine - NeuroSearch. Liraglutide. Exenatide. GLP-1 + PYY 3-36 – Emisphere Technologies.")
68
Medications Thoughts for Research Safety Satiety Side Effects
Long Term Cost Look at gut hormones instead of CNS

69
Thoughts for the Future
Orexigens Neuropeptide Y (NPY) Agouti-related protein (AgRP) Orexin A and B Melanin-concentrating hormone (MCH) Ghrelin (activates NPY and AgRP) Anorexigens Brain-derived neurotrophic factor Alpha-melanocyte stimulating hormone (alpha-MSH) Pro-opiomelanocortin (POMC) Serotonin Cocaine-amphetamine-regulating transcript (CART) Leptin *** Insulin *** *** Inhibit NPY and AgRP
 Agouti-related protein (AgRP) Orexin A and B. Melanin-concentrating hormone (MCH) Ghrelin (activates NPY and AgRP) Anorexigens. Brain-derived neurotrophic factor. Alpha-melanocyte stimulating hormone (alpha-MSH) Pro-opiomelanocortin (POMC) Serotonin. Cocaine-amphetamine-regulating transcript (CART) Leptin *** Insulin *** *** Inhibit NPY and AgRP.")
70
Other Thoughts Need for a safe anti-obesity medication for long term use as obesity is a chronic condition; Short term control is not useful Medications should always be used with diet, exercise and behavioral modification changes Should get informed consent

71
Medications What not to prescribe – HCG diet
ASBP Statement on HCG diet: 1. The Simeons method for weight loss is not recommended. 2. The Simeons diet is not recommended. 3. The use of HCG for weight loss is not recommended. ASBP Position Statement on HCG Diet:

72
Weight Loss Surgery Options

73
Gastric restrictive Malabsorptive
Weight Loss Surgery Gastric restrictive Malabsorptive Vertical Banded Gastroplasty JI bypass Bilio Pancreatic Bypass Duodenal Switch Gastric Bypass Long Limb Gastric Bypass R o u x – e n Y Gastric Sleeve L A P A R O S C O P I C Gastric Band System Gastric Bypass Gastric Sleeve Gastric Band

74
Typical Weight Loss surgery patient
Weight Range (pounds) Number In Each Range How heavy is the average weight loss surgery patient?
 Number In Each Range. How heavy is the average weight loss surgery patient")
75
Candidates for Surgery
Weight Loss Surgery Candidates for Surgery BMI >40 BMI >35 with significant co-morbidities H&P to assess need for cardiac/pulmonary clearances Psychological Evaluation Dietary Screening

76
Gastric restrictive Malabsorptive
JI bypass Bilio Pancreatic Bypass Duodenal Switch Gastric Bypass Long Limb Vertical Banded Gastroplasty Gastric Bypass R o u x – e n Y Gastric Bypass Lap Band

77
Gastric restrictive Malabsorptive
JI bypass Bilio Pancreatic Bypass Duodenal Switch Gastric Bypass Long Limb Vertical Banded Gastroplasty Gastric Bypass R o u x – e n Y Gastric Bypass Lap Band

78
Weight Loss Surgery Mal-absorptive Procedures
JI Bypass Performed from 1950s-1970s Problems / Complications: mineral and electrolyte imbalances, protein malnutrition, abdominal discomfort including flatus and diarrhea, liver disease, renal disease, peripheral neuropathy, pericarditis, and more. BPD / DS More demanding operation than the RYGB Problems / Complications: diarrhea, foul smelling flatulence, mal-absorption of fat soluble vitamins, protein malnutrition, ulcers, and dumping syndrome.

79
Gastric Restrictive Procedures
Staple line failure.

80
Gastric Restrictive Procedures

81
Protein calorie malnutrition
B12 iron Since the stomach is involved in iron and Vitamin B12 absorption, these may not be absorbed adequately following bypass. As a result anemia may develop. The patient feels tired and listless, and blood tests show low levels of hematocrit, hemoglobin, iron, Vitamin B12. The condition can be prevented and treated, if necessary, by taking extra iron and B12. Since the food stream bypasses the duodenum, the primary site of calcium absorption, the possibility of calcium deficiency exists, and all patients should take supplemental calcium to forestall this. Ca++ Dehydration Protein calorie malnutrition 81

82
Gastric Restrictive Procedures
Ghrelin receptors Staple line failure. 82

83
Gastric Sleeve Gastric Bypass 2nd stage R o u x – e n - Y
L A P A R O S C O P I C Gastric Bypass R o u x – e n Y 2nd stage Staple line failure. 83

84
Gastric Restrictive Procedure
Pure gastric restrictive procedures are common in Europe and Australia

86
Weight Loss Surgery Risks of Surgery
Complications may include Mortality (0.24%) Staple line leaks (RYGB) (0.73%) PE (0.25%) DVT (0.17%) Wound infections (1.8%) Marginal ulcers Malnutrition GI Bleed (0.44%) Small Bowel Obstruction (0.40%) These percents were 30 day mortality and complication rate, Source ASMBS
 Staple line leaks (RYGB) (0.73%) PE (0.25%) DVT (0.17%) Wound infections (1.8%) Marginal ulcers. Malnutrition. GI Bleed (0.44%) Small Bowel Obstruction (0.40%) These percents were 30 day mortality and complication rate, Source ASMBS.")
87
Weight Loss AACE/TOS/ASMBS Bariatric Surgery Guidelines, Endocr Pract. 2008;14(Suppl 1)
")
88
Weight Loss Surgery Safety and Monitoring Routine lifetime follow up
Lap Band: monthly for 6 months and fills based on symptoms but routine visits for life RYGB and Sleeve: 1 week, 1 month, 3 month, 6 months, 9 months, 1 year, 18 months, and annually Regular follow up visits help with compliance and better weight loss

89
Weight Loss Surgery Safety and Monitoring Vitamin Supplementation
Bands – multi-vitamin, calcium, fish oil RYGB / Sleeve – multi-vitamin (bariatric), calcium, B12, iron, fish oil
, calcium, B12, iron, fish oil.")
90
Weight Loss Surgery Routine Labs
Bands – general health screening (annually) RYGB / Sleeves – CBC, CMP, folate, thiamine, B12, total iron, TIBC, ferritin, A1C, lipids, vitamin D, TSH Annual bone density
 RYGB / Sleeves – CBC, CMP, folate, thiamine, B12, total iron, TIBC, ferritin, A1C, lipids, vitamin D, TSH. Annual bone density.")
91
Weight Loss Surgery Diet Slow diet progression Food Intolerances
No No Foods Eating Behaviors that need changed

92
Weight Loss Surgery DO NOT Prescribe NSAIDS after RYGB
Prescribe steroids after RYGB Prescribe extended release medications after RYGB SMOKE

93
lifelong. NIH Consensus Severe obesity is a
Chronic, intractable, and progressive disorder; any therapeutic program must, therefore, be lifelong. Just like any other CHRONIC illness

94
References National Institutes of Health (NIH) National Heart, Lung and Blood Institute (NHLBI) North American Association for the Study of Obesity. The practical guide: identification, evaluation, and treatment of overweight and obesity in adults. NIH; 2000; NIH Publication No National Institutes of Health (NIH) National Heart, Lung and Blood Institute (NHLBI). Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. NIH; 1998; NIH Publication No Center for Disease Control. Overweight and Obesity. Center for Disease Control. Overweight and Obesity. World Health Organization. Overweight and Obesity. Build Study, Society of Actuaries and Association of Life Insurance Medical Directors of America, 1980. Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003 Jan 8;289(2): Knight JA. Diseases and disorders associated with excess body weight. Ann Clin Lab Sci. 2011 Spring;41(2): American Society of Bariatric Physicians (ASBP). Bariatric Practice Guidelines American Society of Bariatric Physicians (ASBP). Position statement on HCG diet. Millward D, Layman D, et. al. Protein quality assessment: impact of expanding understanding of protein and amino acid needs for optimal health. AJCN 2008 May; 87, (5), 1576S-1581S. Gardner CD, Kiazand A, Alhassan S, Kim S, Stafford RS, Balise RR, Kraemer HC, King AC. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA. 2007 Mar 7;297(9): Shai I, et. al, Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008 Jul 17;359(3): Sacks FM, et. al, Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N Engl J Med. 2009 Feb 26;360(9):859-73 Mahan L.K, and Escott-Stump, S. Krause’s Food, Nutrition, & Diet Therapy. 11th ed. Philadelphia, Pennsylvania. Elsevier Epocrates Rx Version San Mateo (CA): Epocrates, Inc. Food and Drug Administration. FDA Approved obesity drugs. Heal, D. Gosden, J. and Smith S Regulatory challenges for new drugs to treat obesity and comorbid metabolic disorders. BJCP 68:6: Hussain, SS and Bloom SR. The pharmacological treatment and management of obesity. Postgrad Med Jan: 123 (1): Cooke, D and Bloom S. The obesity pipeline: current strategies in the development of anti-obesity drugs. Nat. Rev Drug Discov Nov: 5(11): Kaplan LM. Pharmacologic therapies for obesity. Gastroenterol Clin North Am Mar: 39 (1):
 National Heart, Lung and Blood Institute (NHLBI) North American Association for the Study of Obesity. The practical guide: identification, evaluation, and treatment of overweight and obesity in adults. NIH; 2000; NIH Publication No National Institutes of Health (NIH) National Heart, Lung and Blood Institute (NHLBI). Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. NIH; 1998; NIH Publication No Center for Disease Control. Overweight and Obesity. Center for Disease Control. Overweight and Obesity. World Health Organization. Overweight and Obesity. Build Study, Society of Actuaries and Association of Life Insurance Medical Directors of America, Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA Jan 8;289(2): Knight JA. Diseases and disorders associated with excess body weight. Ann Clin Lab Sci Spring;41(2): American Society of Bariatric Physicians (ASBP). Bariatric Practice Guidelines American Society of Bariatric Physicians (ASBP). Position statement on HCG diet. Millward D, Layman D, et. al. Protein quality assessment: impact of expanding understanding of protein and amino acid needs for optimal health. AJCN 2008 May; 87, (5), 1576S-1581S. Gardner CD, Kiazand A, Alhassan S, Kim S, Stafford RS, Balise RR, Kraemer HC, King AC. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA Mar 7;297(9): Shai I, et. al, Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med Jul 17;359(3): Sacks FM, et. al, Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N Engl J Med Feb 26;360(9): Mahan L.K, and Escott-Stump, S. Krause’s Food, Nutrition, & Diet Therapy. 11th ed. Philadelphia, Pennsylvania. Elsevier. Epocrates Rx Version San Mateo (CA): Epocrates, Inc. Food and Drug Administration. FDA Approved obesity drugs. Heal, D. Gosden, J. and Smith S Regulatory challenges for new drugs to treat obesity and comorbid metabolic disorders. BJCP 68:6: Hussain, SS and Bloom SR. The pharmacological treatment and management of obesity. Postgrad Med Jan: 123 (1): Cooke, D and Bloom S. The obesity pipeline: current strategies in the development of anti-obesity drugs. Nat. Rev Drug Discov Nov: 5(11): Kaplan LM. Pharmacologic therapies for obesity. Gastroenterol Clin North Am Mar: 39 (1):")
95
References Cont. Kootte RS, et. al; The therapeutic potential of manipulating gut microbiota in obesity and type 2 diabetes mellitus. Diabetes Obes Metab Aug. Ly, NP et. al.; Gut microbiota, probiotics, and vitamin D: interrelated exposures influencing allergy, asthma, and obesity? J Allergy Clin Immunol May; 127 (5): Weir Ma, Beyea MM, Gomes T., et. al. Orlistat and acute kidney injury: an analysis of 953 patients. Arch Intern Med. 2011 Apr 11;171(7):703-4. Brethauer SA, Chand B, Schauer PR. Risks and benefits of bariatric surgery: current evidence. Cleveland Clinic Journal of Medicine (2006) 75(11); Anonymous. Perioperative safety in the longitudinal assessment of bariatric surgery. NEJM Jul; 361(5) 445. Goutham RAO. Office-based strategies for the management of obesity. Am Fam Physician Jun 15; 81(12): American Society of Bariatric Surgery (ASMBS). Rational for surgical treatment. Gastrointestinal Surgery for Severe Obesity. NIH Consensus Statement 1991 Mar 25-27;9(1):1-20. Goldstein DJ, Rampey AH Jr, Roback PJ, Wilson MG, Hamilton SH, Sayler ME, Tollefson GD. Efficacy and safety of long-term fluoxetine treatment of obesity--maximizing success. Obes Res. 1995 Nov;3 Suppl 4:481S-490S. Stunkard AJ, Allison KC, Lundgren JD, Martino NS, Heo M, Etemad B, O'Reardon JP. A paradigm for facilitating pharmacotherapy at a distance: sertraline treatment of the night eating syndrome. J Clin Psychiatry. 2006 Oct;67(10): Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003; 289: AACE/TOS/ASMBS Bariatric Surgery Guidelines, Endocr Pract. 2008;14 (Supp 1)
: Weir Ma, Beyea MM, Gomes T., et. al. Orlistat and acute kidney injury: an analysis of 953 patients. Arch Intern Med Apr 11;171(7): Brethauer SA, Chand B, Schauer PR. Risks and benefits of bariatric surgery: current evidence. Cleveland Clinic Journal of Medicine (2006) 75(11); Anonymous. Perioperative safety in the longitudinal assessment of bariatric surgery. NEJM Jul; 361(5) 445. Goutham RAO. Office-based strategies for the management of obesity. Am Fam Physician Jun 15; 81(12): American Society of Bariatric Surgery (ASMBS). Rational for surgical treatment. Gastrointestinal Surgery for Severe Obesity. NIH Consensus Statement 1991 Mar 25-27;9(1):1-20. Goldstein DJ, Rampey AH Jr, Roback PJ, Wilson MG, Hamilton SH, Sayler ME, Tollefson GD. Efficacy and safety of long-term fluoxetine treatment of obesity--maximizing success. Obes Res Nov;3 Suppl 4:481S-490S. Stunkard AJ, Allison KC, Lundgren JD, Martino NS, Heo M, Etemad B, O Reardon JP. A paradigm for facilitating pharmacotherapy at a distance: sertraline treatment of the night eating syndrome. J Clin Psychiatry Oct;67(10): Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003; 289: AACE/TOS/ASMBS Bariatric Surgery Guidelines, Endocr Pract. 2008;14 (Supp 1)")
Similar presentations












. OR FAT WEIGHT COMPARED TO FAT FREE WEIGHT BODY WEIGHT = 200 LBS. %BODY FAT.>")







