Download presentation
Presentation is loading. Please wait.

1
Robert A Thornton, Jr. District Epidemiologist Coastal Health District
A Storm of Disease Robert A Thornton, Jr. District Epidemiologist Coastal Health District

2
Coastal Health District

3
Why should we worry? During the past 2 decades natural disasters have killed millions of people and adversely affected the lives of at least 1 billion additional persons. Katrina

4
Why should we worry? After a natural disaster, negative impact can unveil either rapidly or slowly. Health effects Social effects Economic effects

5
Disaster related interruption of service
Power cuts can result in disruption of water treatment and sewage service. Vaccine preservation issues (private providers) After the New York blackout in 2003 there was an increase in the amount of diarrheal illness noted, meat and seafood causative agent…power was out several hours to 2 days
 After the New York blackout in 2003 there was an increase in the amount of diarrheal illness noted, meat and seafood causative agent…power was out several hours to 2 days.")
6
Rapid impact Sudden abundance of dead bodies Blunt trauma
Crush related injuries Drowning Death from communicable diseases (at least initially) are less common
 are less common.")
7
Displacement and risk of communicable disease
Size of displaced community (Chatham County 241,411 and District 524,032) Characteristics of population displaced Availability of safe water and latrines Vaccination status of population
 Characteristics of population displaced. Availability of safe water and latrines. Vaccination status of population.")
8
Risk factors for communicable disease transmission
Endemic and epidemic diseases that are common in the affected area. Geographic density of population Immunization status Degree of access to healthcare

9
Water related communicable disease
Diarrheal illness (especially after flooding) Vibrio cholerae E. coli Salmonella Shigella Cryptosporidium Giardia Norovirus
 Vibrio cholerae. E. coli. Salmonella. Shigella. Cryptosporidium. Giardia. Norovirus.")
10
After Hurricanes Allison and Katrina
Norovirus Vibrio cholerae (non toxigenic and toxigenic) Salmonella
 Salmonella.")
11
Nasty bugs after a nasty storm
Hurricane Katrina made landfall on August 29, 2005, with major impact on the U.S. Gulf Coast. During August 29--September 11, surveillance identified 22 new cases of Vibrio illness with five deaths in persons who had resided in two states. These illnesses were caused by V. vulnificus, V. parahaemolyticus, and V. cholerae. These organisms are acquired from the environment and are unlikely to cause outbreaks from person-to-person transmission.

12
Vibrio cholerae after Rita
The two cases of toxigenic V. cholerae O1 infection were identified in a Louisiana couple approximately 3 weeks after Hurricane Rita. On October 15, 2005, in southeastern Louisiana, a man aged 43 years and his wife aged 46 years had onset of diarrhea. The husband had a history of high blood pressure, alcoholism, diabetes, brain tumor, and chronic renal failure that required dialysis three times a week. On October 16, 2005, he was hospitalized for fever, muscle pains, nausea, vomiting, abdominal cramps, and severe diarrhea and dehydration; subsequently he experienced complete loss of renal function and respiratory and cardiac failure. However, after treatment with ciprofloxacin and aggressive rehydration therapy, the man recovered to his previous state of health. His wife had mild diarrhea and was treated as an outpatient with ciprofloxacin and extra fluids. Because the couple's residence had been severely damaged and flooded by Hurricane Rita, both patients had waded in coastal flood waters in late September, 2--3 weeks before their illness onset. Five days before onset of illness, both had eaten locally caught crabs. On October 14, the day preceding illness onset, both had eaten shrimp purchased from a local fisherman. The shrimp were boiled for 5 minutes; however, at least some of the boiled shrimp were returned to a cooler containing raw shrimp and were eaten later. Two other persons who ate the shrimp reported mild diarrhea and abdominal discomfort; they did not seek medical attention, and no stool or serum specimens were collected from them for testing.

13
Prevent illness from water
Listen to and follow public announcements. Local authorities will tell you if tap water is safe to drink or to use for cooking or bathing. If the water is not safe to use, follow local instructions to use bottled water or to boil or disinfect water for cooking, cleaning, or bathing. Correctly boil or disinfect water. Hold water at a rolling boil for 1 minute to kill bacteria. If you can't boil water, add 1/8 teaspoon (approximately 0.75 mL) of newly purchased, unscented liquid household bleach per gallon of water. Stir the water well, and let it stand for 30 minutes before you use it. You can use water-purifying tablets instead of boiling water or using bleach. For infants, use only pre-prepared canned baby formula. Do not use powdered formulas prepared with treated water. Disinfect children's toys that have come in contact with water. Use a solution of 1 cup of bleach in 5 gallons of water to disinfect the toys. Let toys air dry after cleaning. Some toys, such as stuffed animals and baby toys, cannot be disinfected; they should be discarded.
 of newly purchased, unscented liquid household bleach per gallon of water. Stir the water well, and let it stand for 30 minutes before you use it. You can use water-purifying tablets instead of boiling water or using bleach. For infants, use only pre-prepared canned baby formula. Do not use powdered formulas prepared with treated water. Disinfect children s toys that have come in contact with water. Use a solution of 1 cup of bleach in 5 gallons of water to disinfect the toys. Let toys air dry after cleaning. Some toys, such as stuffed animals and baby toys, cannot be disinfected; they should be discarded.")
14
Prevent illness from food
Identify and throw away food that may not be safe to eat. Throw away food that may have come in contact with flood or storm water. Throw away canned foods that are bulging, opened, or damaged. Throw away food that has an unusual odor, color, or texture. Throw away perishable foods (including meat, poultry, fish, eggs and leftovers) that have been above 40°F for 2 hours or more. Thawed food that contains ice crystals or is 40°F or below can be refrozen or cooked. If cans have come in contact with floodwater or storm water, remove the labels, wash the cans, and dip them in a solution of 1 cup of bleach in 5 gallons of water. Relabel the cans with a marker. Store food safely. While the power is out, keep the refrigerator and freezer doors closed as much as possible. Add block ice or dry ice to your refrigerator if the electricity is expected to be off longer than 4 hours. Wear heavy gloves when handling ice.
 that have been above 40°F for 2 hours or more. Thawed food that contains ice crystals or is 40°F or below can be refrozen or cooked. If cans have come in contact with floodwater or storm water, remove the labels, wash the cans, and dip them in a solution of 1 cup of bleach in 5 gallons of water. Relabel the cans with a marker. Store food safely. While the power is out, keep the refrigerator and freezer doors closed as much as possible. Add block ice or dry ice to your refrigerator if the electricity is expected to be off longer than 4 hours. Wear heavy gloves when handling ice.")
15
Vectorborne Diseases Initial flooding may actually wash away existing mosquito breeding sites (weeks delay) New areas of standing water create new breeding sites West Nile virus EEE

16
West Nile after Katrina

17
5 D’s for insects Dawn Dusk Drain Dress DEET

18
Repellants that can be used on skin and clothing
DEET (Chemical Name: N,N-diethyl-m-toluamide or N,N-diethly-3-methyl-benzamide) Picaridin (KBR 3023, Chemical Name: 2-(2-hydroxyethyl)-1-piperidinecarboxylic acid 1-methylpropyl ester ) Oil of Lemon Eucalyptus* or PMD (Chemical Name: para-Menthane-3,8-diol) the synthesized version of oil of lemon eucalyptus IR3535 (Chemical Name: 3-[N-Butyl-N-acetyl]-aminopropionic acid, ethyl ester) Permethrin can be used on clothing only
 Picaridin (KBR 3023, Chemical Name: 2-(2-hydroxyethyl)-1-piperidinecarboxylic acid 1-methylpropyl ester ) Oil of Lemon Eucalyptus* or PMD (Chemical Name: para-Menthane-3,8-diol) the synthesized version of oil of lemon eucalyptus. IR3535 (Chemical Name: 3-[N-Butyl-N-acetyl]-aminopropionic acid, ethyl ester) Permethrin can be used on clothing only.")
19
Diseases Associated with Overcrowding
Rashes Neisseria meningitidis meningitis Acute respiratory infections (especially those younger than 5 years of age)
")
20
Fungal Infections Warm, humid climate promotes fungal growth
Clean up and prevent mold growth. Clean up and dry out the building quickly (within 24 to 48 hours). Open doors and windows. Use fans to dry out the building. To prevent mold growth, clean wet items and surfaces with detergent and water. To remove mold growth, wear rubber gloves, open windows and doors, and clean with a bleach solution of 1 cup of bleach in 1 gallon of water. Throw away porous items (for example, carpet and upholstered furniture) that cannot be dried quickly. Fix any leaks in roofs, walls, or plumbing.
. Open doors and windows. Use fans to dry out the building. To prevent mold growth, clean wet items and surfaces with detergent and water. To remove mold growth, wear rubber gloves, open windows and doors, and clean with a bleach solution of 1 cup of bleach in 1 gallon of water. Throw away porous items (for example, carpet and upholstered furniture) that cannot be dried quickly. Fix any leaks in roofs, walls, or plumbing.")
21
Other injuries and concerns
Chain saw Cuts Musculoskeletal strains Heat exhaustion Dehydration Falls Electrical injuries Carbon monoxide poisoning (over 50 cases after Katrina) Animal bites (mammals, reptiles and insects)
 Animal bites (mammals, reptiles and insects)")
22
Figure 2

23
Summary of Illness after Katrina
During September 1--22, chronic illness (e.g., diabetes, asthma, emphysema, and cardiovascular disease) was the most commonly reported category in ECs, peaking at 651 visits on September 9 (in all four states combined) and accounting for 33% (4,786) of the 14,531 total visits included in these analyses. GI illness, the second most commonly reported category, accounted for 27% (3,892) of total visits and peaked in ECs during September Visits for respiratory illness increased during September 1--22, accounting for 20% (2,896) of total visits and 52% (1,003) of visits during September The percentage of visits for rash illnesses accounted for 16% (320) of visits during September 1--4, decreased somewhat, and then increased again to 20% (376) of visits during September Visits for injury and mental illness accounted for less than 6% each of the total visits during September In HCFs, during September 5--22, injury was the most commonly reported category, with approximately 135 visits reported daily, peaking at 532 on September 8, and accounting for 58% (5,716) of 9,772 total HCF visits for the six categories. Respiratory illness was the second most commonly reported condition, accounting for 16% (1,550) of total HCF visits. During September 5--22, GI, rash, and chronic and mental illnesses each accounted for less than 10% of the total HCF visits.
 was the most commonly reported category in ECs, peaking at 651 visits on September 9 (in all four states combined) and accounting for 33% (4,786) of the 14,531 total visits included in these analyses. GI illness, the second most commonly reported category, accounted for 27% (3,892) of total visits and peaked in ECs during September Visits for respiratory illness increased during September 1--22, accounting for 20% (2,896) of total visits and 52% (1,003) of visits during September The percentage of visits for rash illnesses accounted for 16% (320) of visits during September 1--4, decreased somewhat, and then increased again to 20% (376) of visits during September Visits for injury and mental illness accounted for less than 6% each of the total visits during September In HCFs, during September 5--22, injury was the most commonly reported category, with approximately 135 visits reported daily, peaking at 532 on September 8, and accounting for 58% (5,716) of 9,772 total HCF visits for the six categories. Respiratory illness was the second most commonly reported condition, accounting for 16% (1,550) of total HCF visits. During September 5--22, GI, rash, and chronic and mental illnesses each accounted for less than 10% of the total HCF visits.")
24
Emergency Response Illness After Katrina
Upper respiratory and skin rash symptoms were the most common physical symptoms reported by police officers and firefighters and lacerations and sprains were the most common injuries. In addition, approximately one third reported either depressive symptoms or symptoms of posttraumatic stress disorder (PTSD), or both. Floodwater contact with the nose, mouth, or eye was reported by 51% of firefighters (254 of 500) and 30% of police officers (258 of 864); 52% of police officers (473 of 910) and 63% of firefighters (330 of 524) reported rescuing citizens from flooded areas.
, or both. Floodwater contact with the nose, mouth, or eye was reported by 51% of firefighters (254 of 500) and 30% of police officers (258 of 864); 52% of police officers (473 of 910) and 63% of firefighters (330 of 524) reported rescuing citizens from flooded areas.")
25
Emergency Response Illness After Katrina
Police officers and firefighters reported similar prevalences of physical health symptoms. Approximately 28% of police officers (236 of 848) and 31% of firefighters (162 of 525) reported upper respiratory symptoms (i.e., head/sinus congestion or nose/throat irritation). Cough was reported by 21% of police officers (176 of 845) and 23% of firefighters (124 of 525). Skin rash was reported by 54% of police officers (493 of 909) and 49% of firefighters (258 of 525). Injuries most commonly reported by police officers and firefighters were lacerations (police officers: 20% [184 of 912] and firefighters: 24% [127 of 525]), sprains/strains (13% [120 of 912] and 25% [130 of 525]), falls (9% [84 of 912] and 10% [54 of 525]) and animal bites/stings (11% [104 of 911] and 8% [41 of 525]). Of 525 firefighters, 114 (22%) reported symptoms consistent with PTSD, and 133 of 494 (27) reported major depressive symptoms. Of 912 police officers, 19% (170) reported PTSD symptoms and 26% (227 of 888) reported major depressive symptoms. Among all police officers, 31% (279) reported seeing a health-care provider for post-hurricane illnesses and injuries; health-care utilization among firefighters was not assessed.
 and 31% of firefighters (162 of 525) reported upper respiratory symptoms (i.e., head/sinus congestion or nose/throat irritation). Cough was reported by 21% of police officers (176 of 845) and 23% of firefighters (124 of 525). Skin rash was reported by 54% of police officers (493 of 909) and 49% of firefighters (258 of 525). Injuries most commonly reported by police officers and firefighters were lacerations (police officers: 20% [184 of 912] and firefighters: 24% [127 of 525]), sprains/strains (13% [120 of 912] and 25% [130 of 525]), falls (9% [84 of 912] and 10% [54 of 525]) and animal bites/stings (11% [104 of 911] and 8% [41 of 525]). Of 525 firefighters, 114 (22%) reported symptoms consistent with PTSD, and 133 of 494 (27) reported major depressive symptoms. Of 912 police officers, 19% (170) reported PTSD symptoms and 26% (227 of 888) reported major depressive symptoms. Among all police officers, 31% (279) reported seeing a health-care provider for post-hurricane illnesses and injuries; health-care utilization among firefighters was not assessed.")
26
Immunizations Tetanus and diphtheria toxoid (receipt of primary series, and Td booster within 10 years). Not transmitted person to person, toxin released by the anaerobic tetanus bacillus Clostridium tetani Hepatitis B vaccine series for persons who will be performing direct patient care or otherwise expected to have contact with bodily fluids
. Not transmitted person to person, toxin released by the anaerobic tetanus bacillus Clostridium tetani. Hepatitis B vaccine series for persons who will be performing direct patient care or otherwise expected to have contact with bodily fluids.")
27
Immunizations hepatitis A vaccine (low probability of exposure, even under these conditions, in U.S. ) No transmission from contaminated water has been identified in the U.S. since the 1980s. Hepatitis A outbreaks have not occurred following other hurricanes or floods in other parts of the country, including the devastating hurricanes in Florida last year, and the Midwestern floods of the late 1990's. The Gulf Region has had few hepatitis A cases in recent years, with less than 10 in the past 3 months reported from the New Orleans area. Thus, even though the water and sewage systems are damaged or out of operation in many areas along the Gulf Coast , the risk of a hepatitis A epidemic is extremely low. Vaccine will take at least one to two weeks to provide substantial immunity. typhoid vaccine (low probability of exposure, even under these conditions, in U.S. ). cholera vaccine (low probability of exposure, even under these conditions, in U.S. , plus no licensed cholera vaccine available in the U.S. ). meningococcal vaccine (no expectation of increased risk of meningococcal disease among emergency responders). rabies vaccine series (the full series is required for protection). Persons who are exposed to potentially rabid animals should be evaluated and receive standard post-exposure prophylaxis, as clinically appropriate.
 No transmission from contaminated water has been identified in the U.S. since the 1980s. Hepatitis A outbreaks have not occurred following other hurricanes or floods in other parts of the country, including the devastating hurricanes in Florida last year, and the Midwestern floods of the late 1990 s. The Gulf Region has had few hepatitis A cases in recent years, with less than 10 in the past 3 months reported from the New Orleans area. Thus, even though the water and sewage systems are damaged or out of operation in many areas along the Gulf Coast , the risk of a hepatitis A epidemic is extremely low. Vaccine will take at least one to two weeks to provide substantial immunity. typhoid vaccine (low probability of exposure, even under these conditions, in U.S. ). cholera vaccine (low probability of exposure, even under these conditions, in U.S. , plus no licensed cholera vaccine available in the U.S. ). meningococcal vaccine (no expectation of increased risk of meningococcal disease among emergency responders). rabies vaccine series (the full series is required for protection). Persons who are exposed to potentially rabid animals should be evaluated and receive standard post-exposure prophylaxis, as clinically appropriate.")
28
Handwashing Handwashing or hand sanitizing is one of the most important actions that persons can take that will limit the spread of infection.

29
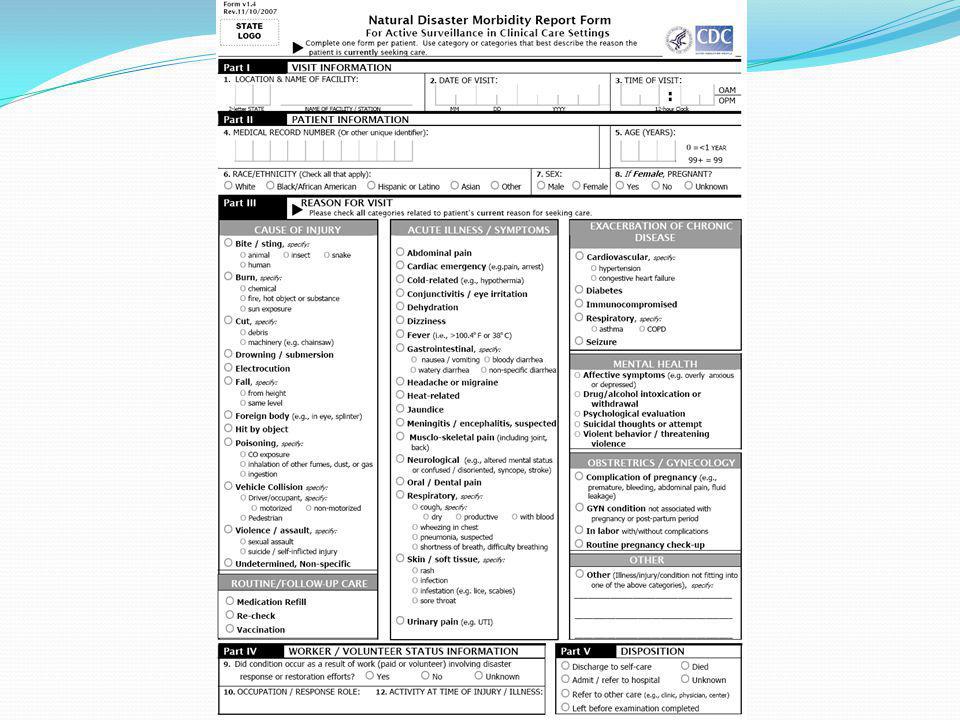
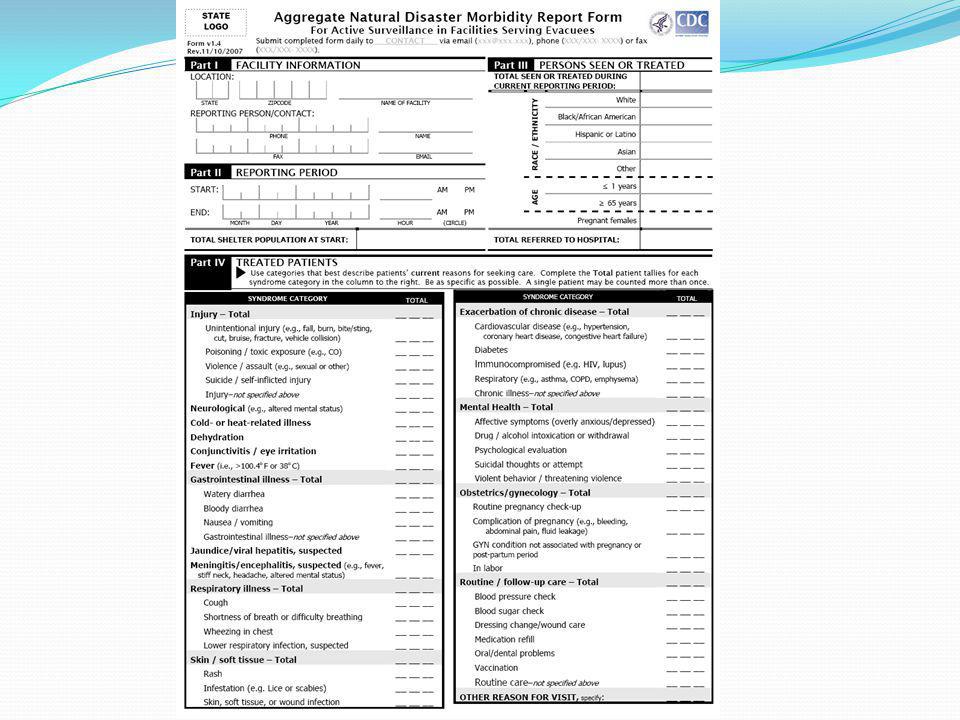
Benefits of Surveillance
Identify the number of illnesses and deaths-related to disasters and provide basic morbidity and mortality information. Identify high risk groups that could benefit from immediate public health interventions. Evaluate and assess the direct and indirect impact of the disaster and human toll in affected communities on high vulnerable groups. Provide information on disaster-related morbidity and mortality for emergency officials and public health officers to assist in future planning and mitigation efforts.

30
Steps that CHD department of Epidemiology will take in order to conduct post storm surveillance
Pre-event communication with State Epidemiology will take place. Alternate operations site will be established, phone numbers and fax numbers provided to community partners and establishment of web capabilities (satellite). Inform healthcare community how to contact CHD Epidemiology staff (hospitals, healthcare providers, infection control practitioners, emergency departments, urgent care centers and laboratory directors)
. Inform healthcare community how to contact CHD Epidemiology staff (hospitals, healthcare providers, infection control practitioners, emergency departments, urgent care centers and laboratory directors)")
31
Provide alternate instructions for disease reporting to aforementioned healthcare partners.
Make sure that extra specimen collection forms and supplies are available for bacterial, viral, ova and parasite testing. Communication with Environmental Health staff to resolve health issues such as animal bites (displaced animals both wild and domestic), investigation of shelter outbreaks, foodborne and waterborne illnesses. Work closely with immunization staff in the event vaccine preventable diseases become a threat to the health of the community (tetanus).
, investigation of shelter outbreaks, foodborne and waterborne illnesses. Work closely with immunization staff in the event vaccine preventable diseases become a threat to the health of the community (tetanus).")
32
Establish and maintain communication with mosquito control staff.
Post hurricane surveillance for injury/illness will take place (hospitals, nursing homes, acute care centers, shelters, correctional facilities) Establish communication with newly opening storm shelters via the local Incident Command System/EOC (Emergency Operations Center). Review disease reporting procedures and determine who will discuss infection control procedures with shelter staff following the storm. Coordinate with Environmental Health Specialists who will be conducting sanitation inspections of shelters and feeding stations. Continue to communicate with shelters (in person or over the phone). Daily communication and monitoring is best for ensuring any community health issues or outbreaks can be addressed as soon as possible.
 Establish communication with newly opening storm shelters via the local Incident Command System/EOC (Emergency Operations Center). Review disease reporting procedures and determine who will discuss infection control procedures with shelter staff following the storm. Coordinate with Environmental Health Specialists who will be conducting sanitation inspections of shelters and feeding stations. Continue to communicate with shelters (in person or over the phone). Daily communication and monitoring is best for ensuring any community health issues or outbreaks can be addressed as soon as possible.")
33
Summary of Disease/Illness
Outbreak management

Similar presentations










. WHAT IS HEPATITIS B DISEASE?>")
![[insert presenting organization]](/11/3127541/big_thumb.jpg "[insert presenting organization]>")








