Download presentation
Presentation is loading. Please wait.

1
Development anatomy of the respiratory organ

3
3

4
Organ respiratoria Upper respiratory organs Nose Nasal cavity nasopharynx Lower respiratory organs Larynx Trachea Bronchi lung

6
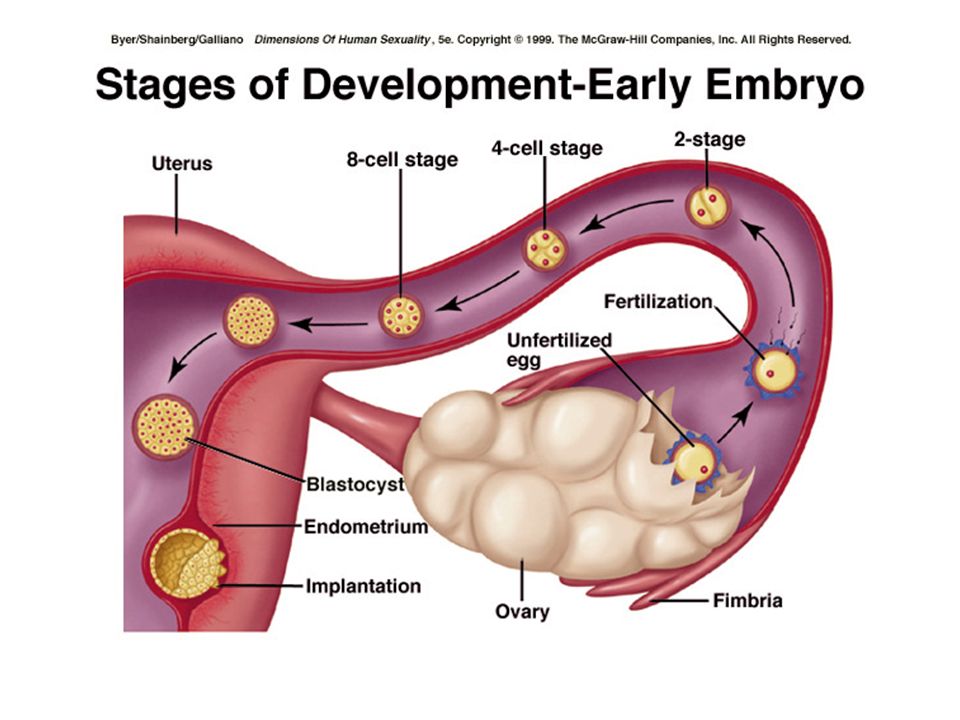
Embrio mg ke-2 Mg pertama: Tahapan embrioblast: zygot –hasil fertilisasi – blastomer – morula (16 sel)- 3 hari- blastokista – implantasi 6 hari
- 3 hari- blastokista – implantasi 6 hari")
7
Lapisan embriologi: 2 lapisan (bilaminer) cakram embrional: minggu ke 2- epiblast dan hipoblast 3 lapisan embriologi (gastrulasi): mg ke 3 embrional (hari ke 17) Ectoderm (epiblast) Mesoderm (epiblast) Endoderm (hypoblast)
 cakram embrional: minggu ke 2- epiblast dan hipoblast 3 lapisan embriologi (gastrulasi): mg ke 3 embrional (hari ke 17) Ectoderm (epiblast) Mesoderm (epiblast) Endoderm (hypoblast)")
8
Endoderm Usus enteron primitif Usus depan Pre entero anterior Mulut, esophagus, gaster, duodenum (partim) Hati, pancreas Saluran pernafasan Trachea, pulmo Thymus, thyroid Usus tengah Mesentero Duodenum, jejenum Ileum, colon ascen Colon transv (part) Usus belakang Met enteron caudal Colon trans (part) Colon desc, colon Sigmoid, rectum Vesica urinaria, urethra
 Hati, pancreas Saluran pernafasan Trachea, pulmo Thymus, thyroid Usus tengah Mesentero Duodenum, jejenum Ileum, colon ascen Colon transv (part) Usus belakang Met enteron caudal Colon trans (part) Colon desc, colon Sigmoid, rectum Vesica urinaria, urethra")
9
Embriologi: bagian thorax Minggu ke 3 (hari 15 – 21) embrional: embrio bagian cranial - caput – otak (hari 20) somite batang trunkus – somite, heart tuba fused bagian caudal sisi ventral sisi dorsal Minggu ke 4: trunkus – limb bud- kuncup lengan-arm bud (hari ke 26), leg bud (hari 28), heart bulg
 embrional: embrio bagian cranial - caput – otak (hari 20) somite batang trunkus – somite, heart tuba fused bagian caudal sisi ventral sisi dorsal Minggu ke 4: trunkus – limb bud- kuncup lengan-arm bud (hari ke 26), leg bud (hari 28), heart bulg")
10
somite

12
Development of face:nose Nasal placodes and medial and lateral nasal processes Nasal cofactor placode:two ectodermal elevation on each side of median plane of frontonasal process –and surface depression, and the edges become nasal process, the lateral more prominent, forms alae of nose Medial process merge each other, as result growing of maxillar eminence (maxillar process), become middle part of upper lip, upper jaw, primary palate Remains of maxillar process become cheek Mandibular process: lower lip and lower jaw Formation eyes: from lens placode;Formation external ear, from ectodermal cleft from series mesodermal thickening (pinna)
, become middle part of upper lip, upper jaw, primary palate Remains of maxillar process become cheek Mandibular process: lower lip and lower jaw Formation eyes: from lens placode;Formation external ear, from ectodermal cleft from series mesodermal thickening (pinna)")
15
Development of nasal cavity Formation of nasal pit, after primitive palate formed by fusion lateral and medial nasal processes, created partition between nasal pits and stomatodeum Formation of nasal sacs,nasal pits deepen and enlarge dorsally, caudally form nasal sacs Posterior part of nasal sacs, separated by buconasal membrane, and soon disappears, forming posterior nares Formation of nasal septum, the nasal sacs, separated each other by the with intervening part of frontonasal process Secondary palate, separates nasal cavities from mouth cavity Formation structures of lateral wall:lateral nasal process, nasal conchae, olfactory epithelium (ectodermal thickening) Paranasal sinus:xaxillary and sphenoid formed end of fetal life, other formed after birth
 Paranasal sinus:xaxillary and sphenoid formed end of fetal life, other formed after birth")
19
pharynx:cephalic (pre- laryngeal) of foregut (from buccopharyngeal membrane to tracheobroncheal diverticulum) Definitive pharynx:primitive pharynx after formed branchial apparatus (palate & mouth) Nasopharynx: communicate ventrally, forms cranial part of stomatodeum after formation palate Nasopharynx: from stomatodeum after ruptured buccopharyneal membrane Laryngopharynx: tracheobronchial diverticulum
 of foregut (from buccopharyngeal membrane to tracheobroncheal diverticulum) Definitive pharynx:primitive pharynx after formed branchial apparatus (palate & mouth) Nasopharynx: communicate ventrally, forms cranial part of stomatodeum after formation palate Nasopharynx: from stomatodeum after ruptured buccopharyneal membrane Laryngopharynx: tracheobronchial diverticulum")
20
Anomaly of nasal cavity Atresia of nasal cavity Anomaly of nasal septum, deflected of nasal septum and absence of septum Cleft palate (abnormal communication mouth and nasal cavity)
")
22
Primordia lower respiratory organs Respiratory diverticulum (lung bud): endodermal structures from foregut, forms epithelial lining Splanchnic mesoderm;surrounding lungbud: forms cartilagenous part, muscular, connective tissue component Fourth and six pharyngeal arches, forms cartilage (thyroid, cricoid, arytenoid, corniculata, cuneiform) and muscle of larynx (intrinsic muscle), cricothyroid, contrictor of pharynx muscles : innervasi n vagus (superior laryngeal & recurrent laryneal)
: endodermal structures from foregut, forms epithelial lining Splanchnic mesoderm;surrounding lungbud: forms cartilagenous part, muscular, connective tissue component Fourth and six pharyngeal arches, forms cartilage (thyroid, cricoid, arytenoid, corniculata, cuneiform) and muscle of larynx (intrinsic muscle), cricothyroid, contrictor of pharynx muscles : innervasi n vagus (superior laryngeal & recurrent laryneal)")
23
LARYNX VC5-VC7 Skeleton laryngis: cartilago laryngis Epiglottica (elastis) thyroidea (hyalin) cricoidea arytenoidea corciculata cuneiforme Articulatio cricothyroidea cricoarytenoidea
 thyroidea (hyalin) cricoidea arytenoidea corciculata cuneiforme Articulatio cricothyroidea cricoarytenoidea")
25
Embriologi rongga tubuh

26
Rongga rongga tubuh Pembentukan selom intraembrional mg 3: sebelumnya – rongga amnion, selom ekstraembrional, kantong kuning telur Akhir mg 3; mesoderm lateral – somatik & splanknik - -- selom intraembrional (dada sampai panggul) Lapisan somatik – lapisan parietal membran serosa – rongga peritoneum, pleura dan kantong jantung;Lapisan splanknik – lapisan visceral m. serosa nya – di dorsal sbg mesenterium dorsale, dan di ventral sbg mesenterium ventrale (di usus depan) krn ada septum transversum
 krn ada septum transversum.")
27
Diaphragma dan rongga dada Septum transversum – sekat mesoderm : rongga dada – tangkai kantong kuning telur Tidak memisahkan sempurna rongga dada & rongga perut Lubang: saluran perikardioperitoneal di kiri kanan usus depan Ada tunas pulmo, tumbuh cepat di dalam saluran perikardioperitoneal, lipatan pleuroperikardial – rigi menonjol – ruang dada primitif, pulmo meluas, rongga mesoderma dinding tubuh – dibelah 2 komponen:dinding dada definitif dan membrana pleuroperikardial Jantung turun, sinus venosus, membrana tertarik keluar – rongga dada; rongga perikardium tetap & dua rongga pleura tetap

28
Rongga dada & perut serta diaphragma Mg ke 7: rongga dada & perut tertutup oleh selaput pleuroperitoneal (: lipatan pleuroperitoneal), septum transversom, mesenterium esophagus--- mioblas dinding tubuh membentuk bagian otot diaphragma Klinis : hernia diaphragmatica
, septum transversom, mesenterium esophagus--- mioblas dinding tubuh membentuk bagian otot diaphragma Klinis : hernia diaphragmatica")
29
Embriologi diaphragma Septum transversum (bag tendinosa) Mioblast dinding tubuh lateral & ventral (bag. Muscular) Selaput pleuroperitoneal (sekat yang ditempati mioblas) Mesenterium esophagus (crura)
 Selaput pleuroperitoneal (sekat yang ditempati mioblas) Mesenterium esophagus (crura).")
30
Perkembangan bagian badan

31
Derivat 3 lapisan embrional di thorax endoderm Esophagus (fore gut), Pulmo (fore gut) Thymus – saccus pharyngealis mesoderm Jantung, pembuluh darahMesoderma somatik Somite: skelotome (tulang); otot (dermomiotome) Mesoderma splanknik ectooderm Medulla spinalis: basalis (ventral) & alaris (dorsalis Sel crista neuralis
, Pulmo (fore gut) Thymus – saccus pharyngealis mesoderm Jantung, pembuluh darahMesoderma somatik Somite: skelotome (tulang); otot (dermomiotome) Mesoderma splanknik ectooderm Medulla spinalis: basalis (ventral) & alaris (dorsalis Sel crista neuralis")
32
Embriologi trachea & pulmo Embrio 4 mg: tunas pulmo (diverticulum respiratorium) – tonjolan keluar dari dinding ventral usus depan Epitel – larynx, trachea, bronchus, epitel paru dari endoderm Tulang rawan, otot polos – dari mesoderma splanknik sekeliling usus depan Rigi esophagotrachealis – septum – trpisa h: esophagus & trachea dan tunas pulmo
 – tonjolan keluar dari dinding ventral usus depan Epitel – larynx, trachea, bronchus, epitel paru dari endoderm Tulang rawan, otot polos – dari mesoderma splanknik sekeliling usus depan Rigi esophagotrachealis – septum – trpisa h: esophagus & trachea dan tunas pulmo")
33
Phases of lung development Embryonic phase Pseudoglandular phase Canalicular phase Saccular phase Alveolar phase Classification in the adult lung

36
1Foregut 2Anlage of the thyroid 3Anlage of the lungs 4Stomach 5Anlage of the dorsal pancreas 6Midgut 7Hindgu

37
embryonic phase The embryonic phase of lung development begins with the formation of a groove in the ventral lower pharynx, the sulcus laryngotrachealis (stage 10, ca. 28 days, 10 ). After a couple of days - from the lower part - a bud forms, the true lung primordium (stage 12, ca. 30 days, 12 ). In the further subdivision into the two main bronchi (stage 14, ca. 33 days, 14 ) the smaller bud on the left is directed more laterally than the somewhat larger one on the right that - parallel to the esophagus - is directed more caudally. Thus the asymmetry of the main bronchi, as they present in adults, is already established. The subsequent divisions of the endodermal branches also take place unequally in that on the right three further buds form and, on the left, only two, corresponding to the later pulmonary lobes. In the next division step, which occurs at the end of the embryonic period, the segments of the individual pulmonary lobes arise.
. After a couple of days - from the lower part - a bud forms, the true lung primordium (stage 12, ca. 30 days, 12 ). In the further subdivision into the two main bronchi (stage 14, ca. 33 days, 14 ) the smaller bud on the left is directed more laterally than the somewhat larger one on the right that - parallel to the esophagus - is directed more caudally. Thus the asymmetry of the main bronchi, as they present in adults, is already established. The subsequent divisions of the endodermal branches also take place unequally in that on the right three further buds form and, on the left, only two, corresponding to the later pulmonary lobes. In the next division step, which occurs at the end of the embryonic period, the segments of the individual pulmonary lobes arise..")
38
at the end of the embryonic period the first segments appear in the five (three right and two left) lobes of the lungs. With their distended ends the lungs resemble an exocrine gland. At this time the pulmonary vessels have formed themselves. The pulmonary circulation system (smaller circulation system) is formed out of the 6th pharyngeal arch artery. These develop somewhat differently than the other 4 aortic arches in that first a vessel plexus forms around the lung anlage, originating from the aortic sac. The true 6th aortic arch is only then formed after vessels - also from the dorsal aorta - grow into this plexus and thus a connection between the truncus pulmonalis and dorsal aorta has arisen.
 is formed out of the 6th pharyngeal arch artery. These develop somewhat differently than the other 4 aortic arches in that first a vessel plexus forms around the lung anlage, originating from the aortic sac. The true 6th aortic arch is only then formed after vessels - also from the dorsal aorta - grow into this plexus and thus a connection between the truncus pulmonalis and dorsal aorta has arisen..")
39
From the aortic sac a vessel plexus arises around the lung anlagen that with the lung buds extends caudally. 1First aortic arch (atrophying) 2Second aortic arch 3Third aortic arch (internal carotid artery forms from the ventral part) 4Fourth aortic arch (on the right: part of the subclavian artery, left: arcus aortae) 5Dorsal aorta 6Lung buds 7Aortic sac 8Pulmonary plexus
 2Second aortic arch 3Third aortic arch (internal carotid artery forms from the ventral part) 4Fourth aortic arch (on the right: part of the subclavian artery, left: arcus aortae) 5Dorsal aorta 6Lung buds 7Aortic sac 8Pulmonary plexus.")
40
Pseudoglandular phase At this stage the lungs resemble the development of a tubulo- acinous gland. According to the classical view, the entire air-conducting bronchial tree up to the terminal bronchioli are set down in this phase (16 generations). Recent morphometric studies (3) have shown that with the end of the pseudoglandular phase 20 generations are partially present in the lungs, which means that at this point in time the respiratory ducts have already been formed. The primordial system of passages, the air-conducting bronchial tree, is initially coated by cubic epithelium3 These are the precursor cells of the ciliated epithelium and of the secretory cells. In humans, the first ciliated epithelial cells can be found in the 13th week of pregnancy (7). In the respiratory part the first typically lung-specific cells, connected to the terminal bronchioli, appear: the type II pneumocytes (alveolar cells) (3). The developing broncho- pulmonary epithelium begins to produce amniotic fluid, which is also found in the lungs up to the time of birth.73
. Recent morphometric studies (3) have shown that with the end of the pseudoglandular phase 20 generations are partially present in the lungs, which means that at this point in time the respiratory ducts have already been formed. The primordial system of passages, the air-conducting bronchial tree, is initially coated by cubic epithelium3 These are the precursor cells of the ciliated epithelium and of the secretory cells. In humans, the first ciliated epithelial cells can be found in the 13th week of pregnancy (7). In the respiratory part the first typically lung-specific cells, connected to the terminal bronchioli, appear: the type II pneumocytes (alveolar cells) (3). The developing broncho- pulmonary epithelium begins to produce amniotic fluid, which is also found in the lungs up to the time of birth.73.")
41
the pseudoglandular phase In the pseudoglandular phase the lungs resemble a gland. At the end of this phase the precursors of the pneumocytes can be discerned in the respiratory sections as cubic epithelium.

42
Relatively early in the development of the lungs, endocrine-active cells (Kultschitsky cells) appear that produce bombesin and serotonin. In contrast to the precursors of the pneumocytes, which originate from the endoderm, they stem from the neural crest (neuroectoderm). Via paracrine mechanisms bombesin probably plays a decisive role for lung development in that mainly the type II pneumocytes proliferate. (1)1 The differentiation of the lungs takes place in a centrifugal direction. In the central, air- conducting portions of the lungs the epithelium begins to differentiate into cilia-carrying cells and goblet cells. After the 10th week cartilage and smooth muscle cells as well as bronchial glands can be found in the wall of the bronchi. The peripheral sections partially retain - until far beyond the pseudoglandular phase - cubic epithelium that is still little differentiated
. Via paracrine mechanisms bombesin probably plays a decisive role for lung development in that mainly the type II pneumocytes proliferate. (1)1 The differentiation of the lungs takes place in a centrifugal direction. In the central, air- conducting portions of the lungs the epithelium begins to differentiate into cilia-carrying cells and goblet cells. After the 10th week cartilage and smooth muscle cells as well as bronchial glands can be found in the wall of the bronchi. The peripheral sections partially retain - until far beyond the pseudoglandular phase - cubic epithelium that is still little differentiated.")
43
This is important for a further proliferation of the bronchial tree into the surrounding mesenchymal tissue. f one begins, roughly estimated, with a number of 15'000 terminal bronchioli (8) per lung in adults and thereby ca. 15,000 acini and with a theoretical assumption of a dichotomous division of the pulmonary branches, one has the result that this stage is attained after little fewer than 2 14 generations.8 In the late pseudoglandular stage one finds, however, far more than 15'000 end pieces. Thus the lung end pieces at this stage already represent the respiratory portions of the lungs.
 per lung in adults and thereby ca. 15,000 acini and with a theoretical assumption of a dichotomous division of the pulmonary branches, one has the result that this stage is attained after little fewer than 2 14 generations.8 In the late pseudoglandular stage one finds, however, far more than end pieces. Thus the lung end pieces at this stage already represent the respiratory portions of the lungs..")
44
Canalicular phase in the classical description of lung development, in this phase the canaliculi branch out of the terminal bronchioli. The canaliculi compose the proper respiratory part of the lungs, the pulmonary parenchyma. All of the air spaces that derive from a terminal bronchiolus form an acinus. Each one comprises respiratory bronchioli and the alveolar ducts and later the alveolar sacculi. The chief characteristic of this canalicular phase is the alteration of the epithelium and the surrounding mesenchyma. Along the acinus, which develops from the terminal bronchiolus, an invasion of capillaries into the mesenchyma occurs. The capillaries surround the acini and thus form the foundation for the later exchange of gases. The lumen of the tubules becomes wider and a part of the epithelial cells get to be flatter. From the cubic type II pneumocytes develop the flattened type I pneumocytes.

45
A sufficient differentiation of the type II pneumocytes into the type I pneumocytes and the proliferation of the capillaries into the mesenchyma marks an important step towards the fetus being able to survive outside the uterus after roughly the 24th week of pregnancy.

46
The type I pneumocytes differentiate out of the type II pneumocytes. The capillaries approach the walls of the acini

47
canalicular phase The first breathing movement can be registered already at the end of the embryonic period. They are controlled by a breathing center in the brain stem. Nevertheless, these breathing movements are paradoxical in that when the diaphragm contracts, the thorax moves inwardly and vice versa. (2)2 The surfactant (abbreviation for surface active agent) consists of glycerophospholipids, specific proteins, neutral fats and cholesterol. It covers the alveolar surface and reduces the surface tension so that, following birth, the alveoli do not collapse during the expiration. At the end of this canalicular phase which is the beginning of the saccular phase (ca. 25 weeks) - a large part of the amniotic fluid is produced by the lung epithelium. From this time on, the maturity of the lungs can be measured clinically based on the activity of the type II pneumocytes, which begin to produce the surfactant. The ratio of lecithin to sphingomyelin in the amniotic fluid, which increases with fetal age is determined. In this stage developmental damage already affects the gas-exchange components and result in structural alterations of the later pulmonary parenchyma.
2 The surfactant (abbreviation for surface active agent) consists of glycerophospholipids, specific proteins, neutral fats and cholesterol. It covers the alveolar surface and reduces the surface tension so that, following birth, the alveoli do not collapse during the expiration. At the end of this canalicular phase which is the beginning of the saccular phase (ca. 25 weeks) - a large part of the amniotic fluid is produced by the lung epithelium. From this time on, the maturity of the lungs can be measured clinically based on the activity of the type II pneumocytes, which begin to produce the surfactant. The ratio of lecithin to sphingomyelin in the amniotic fluid, which increases with fetal age is determined. In this stage developmental damage already affects the gas-exchange components and result in structural alterations of the later pulmonary parenchyma..")
48
From the last trimester whole clusters of sacs form on the terminal bronchioli, which represent the last subdivision of the passages that supply air. In the saccular phase the last generation of air spaces in the respiratory part of the bronchial tree is born. At the end of each respiratory tract passage smooth- walled sacculi form, coated with type I and type II pneumocytes. The septa (primary septa) between the sacculi are still thick and contain two networks of capillaries that come from the neighboring sacculi. The interstitial space is rich with cells and the proportion of collagen and elastic fibers is still small. This matrix, though, plays an important role for the growth and differentiation of the epithelium that lies above it (9). At the end of this phase the interstitial fibroblasts begin with the production of extracellular material in the interductal and intersaccular space.9
 between the sacculi are still thick and contain two networks of capillaries that come from the neighboring sacculi. The interstitial space is rich with cells and the proportion of collagen and elastic fibers is still small. This matrix, though, plays an important role for the growth and differentiation of the epithelium that lies above it (9). At the end of this phase the interstitial fibroblasts begin with the production of extracellular material in the interductal and intersaccular space.9.")
49
The capillaries multiply around the acini. They push close to the surface and form a common basal membrane with that of the epithelium 1. Type I pneumocyte 2Type II pneumocyte 3Capillaries

50
he blood-air barrier in the lungs is reduced to three, thin layers: type I pneumocyte, fusioned basal membrane, and endothelium of the capillary. 1Type I pneumocyte 2Saccular space 3Type II pneumocyte 4Basal membrane of the air passage 5Basal membrane of the capillaries 6Endothelium of the capillaries

51
the saccular phase, At birth, i.e., at the end of the saccular phase, all generations of the conducting and respiratory branches have been generated. The sacculi are thin, smooth-walled sacks and correspond to the later alveolar sacculi.

52
alveolar phase Depending on the author, the alveolar phase begins at varying times. Probably in the last few weeks of the pregnancy, new sacculi and, from them, the first alveoli form. Thus, at birth, ca. 1/3 of the roughly 300 million alveoli should be fully developed. The alveoli, though, are only present in their beginning forms. Between them lies the parenchyma, composed of a double layer of capillaries, that forms the primary septa between the alveolar sacculi.

53
In the alveolar phase the alveoli form from the terminal endings of the alveolar sacculi and with time increase their diameter. 1Alveolar duct 2Primary septum 3Alveolar sac 4Type I pneumocyte 5Type II pneumocyte 6Capillaries

54
Already before birth these alveolar sacculi get to be increasingly complex structurally. Thereby, a large number of small protrusions form along the primary septa. Soon, these become larger and subdivide the sacculi into smaller subunits, the alveoli, which are delimited by secondary septa. Ultrastructural investigations show that overall where such alveoli appear, they are surrounded by elastic fibers that form the interstitial septa between two capillary nets. In the first 6 months, their number increases massively. This "alveolarization" and therewith the formation of secondary septa should - to a limited extent still - continue up to the first year and a half of life.

55
In the alveolar phase after birth more and more alveoli form from the terminal endings of the alveolar sacculi and with time increase in diameter. They are delimited by secondary septa. 1Alveolar duct 2Secondary septum 3Alveoli 4Type I pneumocyte 5Type II pneumocyte 6Capillaries

58
In the adult lung one distinguishes between conducting and respiratory zones. In the conducting zone, all branches of the bronchial tree, the walls of which contain cartilage tissue and seromucous glands, are bronchi. As soon as cartilage and glands are no longer present, bronchioli are involved.

59
Diagrams for comparing the constructions of the walls in the respiratory tract 1Ciliated epithelium 2Goblet cell 3Gland 4Cartilage 5Smooth muscle cell 6Clara cell 7Capillary 8Basal membrane 9Surfactant 10Type I pneumocyte 11Alveolar septum 12Type II pneumocyte

60
According to their function the respiratory tract passages are divided into conducting and respiratory zones: Conducting zone = 16 generations Segmental bronchi are continued by several generations of Intersegmental bronchi (up to ca. 1 mm diameter). After these follow the Bronchioli (< 1mm diameter) that after several divisions go over into Terminal bronchioli (ca. 0.4 mm diameter). They subdivide numerous times and represent the end stretch of the purely conductive respiratory tract. The measurements come from histological findings. Histological image of respiratory epithelium.Respiratory zone = 7 generations Out of the terminal bronchioli several generation of Respiratory bronchioli (= 3 generations) proceed. From them follow several generations of Alveolar ducts (= 3 generations) that in Alveolar sacculi (last generation = 23rd generation) end
. After these follow the Bronchioli (< 1mm diameter) that after several divisions go over into Terminal bronchioli (ca. 0.4 mm diameter). They subdivide numerous times and represent the end stretch of the purely conductive respiratory tract. The measurements come from histological findings. Histological image of respiratory epithelium.Respiratory zone = 7 generations Out of the terminal bronchioli several generation of Respiratory bronchioli (= 3 generations) proceed. From them follow several generations of Alveolar ducts (= 3 generations) that in Alveolar sacculi (last generation = 23rd generation) end.")
62
For the branching out of ever new lung buds an interaction between the respiratory endodermal epithelium and the surrounding pulmonary mesenchyma is primarily responsible. Mainly the epidermal growth factor (EGF) and the extracellular form of the transforming growth factors (TGF-b) appear to be important for lung development. In addition, one finds specific extracellular matrix components like collagen of types I and III, as well as proteoglycan and the fibronectin and syndecan glycoproteins.. ( These molecules are found around the passages and in the forks of the bronchial tree. They are responsible for the stabilization of the already formed structures - these are not present in the regions of the newly formed branches. Epimorphine, a further protein, appears to promote the formation of epithelial passages. If epimorphine is blocked by antibodies, the epithelium that lies above it can not form itself into tubes and remains unorganized
 and the extracellular form of the transforming growth factors (TGF-b) appear to be important for lung development. In addition, one finds specific extracellular matrix components like collagen of types I and III, as well as proteoglycan and the fibronectin and syndecan glycoproteins.. ( These molecules are found around the passages and in the forks of the bronchial tree. They are responsible for the stabilization of the already formed structures - these are not present in the regions of the newly formed branches. Epimorphine, a further protein, appears to promote the formation of epithelial passages. If epimorphine is blocked by antibodies, the epithelium that lies above it can not form itself into tubes and remains unorganized.")
63
anomaly Laryngeal atresia Fistula tracheo- esophageal Tracheal stenosis, atresia Agenesis trachea Agenesis of lung Hyaline membrane disease/respiratory distress syndrome

65
Tracheoesophageal fistula A fistula is a tube. The esophagus is a tube that goes to the stomach and the trachea is a tube that goes to the lungs. Normally these two tubes do not connect but when a baby has a tracheoesophageal fistula, there is a tube connecting the two. This can cause problems with feeding and even breathing in newborns and needs to be corrected.

66
Oesophageal Atresia and/or Tracheoesophageal Fistula Embryology Smith's theory: The trachea and esophagus initially begin as a single tube. The lateral esophageal grooves are formed as the dorsal esophagus is separated from the ventral trachea. Should the septation process continue distally, esophageal atresia would result. Grunewald's theory: Elongation of the trachea is rapid in a caudal direction. When there is a fistula producing fixation of esophagus to trachea, the dorsal wall of the esophagus is drawn forward and downward to be incorporated into the trachea. Atresia of the esophagus results because of the fistula. Bronchogenic theory: The esophagus does not develop at all distally. Rather, a third "bronchus" develops in the primordial lung bud and grows inferiorly to attach to the stomach.

67
The esophagus and trachea derive from the primitive foregut. During the fourth and fifth weeks of embryologic development, the trachea forms as a ventral diverticulum from the primitive pharynx (caudal part of the foregut),5 as illustrated in Figure 3. A tracheoesophageal septum develops at the site where the longitudinal tracheoesophageal folds fuse together.. This septum divides the foregut into a ventral portion, the laryngotracheal tube and a dorsal portion (the esophagus). Esophageal atresia results if the tracheoesophageal septum is deviated posteriorly. This deviation causes incomplete separation of the esophagus from the laryngotracheal tube and results in a concurrent tracheoesophageal fistula
,5 as illustrated in Figure 3. A tracheoesophageal septum develops at the site where the longitudinal tracheoesophageal folds fuse together.. This septum divides the foregut into a ventral portion, the laryngotracheal tube and a dorsal portion (the esophagus). Esophageal atresia results if the tracheoesophageal septum is deviated posteriorly. This deviation causes incomplete separation of the esophagus from the laryngotracheal tube and results in a concurrent tracheoesophageal fistula.")
68
Successive stages in the development of the tracheoesophageal septum during embryologic development. (A) The laryngotracheal diverticulum forms as a ventral outpouching from the caudal part of the primitive pharynx. (B) Longitudinal tracheoesophageal folds begin to fuse toward the midline to eventually form the tracheoesophageal septum. (C) The tracheoesophageal septum has completely formed. (D) If the tracheoesophageal septum deviates posteriorly, esophageal atresia with a tracheoesophageal fistula develops.
 The laryngotracheal diverticulum forms as a ventral outpouching from the caudal part of the primitive pharynx. (B) Longitudinal tracheoesophageal folds begin to fuse toward the midline to eventually form the tracheoesophageal septum. (C) The tracheoesophageal septum has completely formed. (D) If the tracheoesophageal septum deviates posteriorly, esophageal atresia with a tracheoesophageal fistula develops..")
69
Relative frequencies of occurrence of the various types of esophageal atresia (EA) with and without tracheoesophageal fistula (TEF).
 with and without tracheoesophageal fistula (TEF).")
70
Esophageal atresia is characterized by incomplete formation of the esophagus. It is often associated with a fistula between the trachea and the esophagus. Many anatomic variations of esophageal atresia with or without tracheoesophageal fistula have been described7,8 (Figure 4). Table 11,3,9-12 provides a summary of the incidence of these variations at multiple worldwide surgical centers. The most common variant of this anomaly consists of a blind esophageal pouch with a fistula between the trachea and the distal esophagus, which is estimated to occur 84 percent of the time. The fistula often enters the trachea close to the
. Table 11,3,9-12 provides a summary of the incidence of these variations at multiple worldwide surgical centers. The most common variant of this anomaly consists of a blind esophageal pouch with a fistula between the trachea and the distal esophagus, which is estimated to occur 84 percent of the time. The fistula often enters the trachea close to the.")
72
GI Motility online (May 2006) | doi:10.1038/gimo6 Figure 10 Main types of tracheoesophageal fistulae
 | doi: /gimo6 Figure 10 Main types of tracheoesophageal fistulae")
73
he figure shows both tracheoesophageal fistula (A-E) and tracheal abnormalities ( F-J). Note that A-E do not correspond with the classification of the type of tracheoesophageal fistula. A shows type C, B type B, C type D, D type E, and E type A tracheoesophageal fistula, respectively. (Source: Netter medical illustration with permission from Elsevier. All rights reserved.)
.")
75
The main varieties of tracheoesophageal fistula. Possible directions of the flow of the contents are indicated by arrows. Esophageal atresia, as illustrated in A, is associated with tracheoesophageal fistula in more than 85% of cases. B, Fistula between the trachea and esophagus. In C, air cannot enter the distal esophagus and stomach. Air can enter the distal esophagus and stomach in D, and the esophageal and gastric contents may enter the trachea and lungs.

76
Classification (Gross's Anatomical Classification) Type A: Esophageal atresia without tracheoesophageal fistula. Type B: Esophageal atresia with proximal tracheoesophageal fistula. Type C: Esophageal atresia with distal tracheoesophageal fistula (most common type) (85%). Type D: Esophageal atresia with proximal and distal fistula. Type E: Tracheoesophageal fistula without atresia. (Not shown)
 (85%). Type D: Esophageal atresia with proximal and distal fistula. Type E: Tracheoesophageal fistula without atresia. (Not shown).")
Similar presentations




















 Monday, May 04, 2015 Monday, May 04, 2015.>")















