Download presentation
Presentation is loading. Please wait.

1
Interactive Well-Being Lab www.sussex.ac.uk/iwl 1 Computerised Cognitive Behavioural Therapies

2
2

3
Mood and Anxiety Disorders 1 in 5 people suffer from anxiety or depression at any one time (ONS, 2000) Approximately 1/3 seek help for these common problems from their GP (Bebbington, 2005) 10% of those seeking treatment receive any kind of counselling or talking therapy Fewer (1%-5%) access evidence based talking therapies such as cognitive behavioural therapy Service capacity is limited and CBT therapists are inequitably distributed (Shapiro, Cavanagh & Lomas, 2003) 3
 Approximately 1/3 seek help for these common problems from their GP (Bebbington, 2005) 10% of those seeking treatment receive any kind of counselling or talking therapy Fewer (1%-5%) access evidence based talking therapies such as cognitive behavioural therapy Service capacity is limited and CBT therapists are inequitably distributed (Shapiro, Cavanagh & Lomas, 2003) 3")
4
Increasing access to psychological therapies A revolution in mental health care (Bennet-Levy, Richards & Farrand, 2010, p3) Range of initiatives to increase early access to effective psychological interventions – Training (and supervision) of more staff to deliver evidence based interventions – Restructuring services – Exploring alternatives to 1-to-1 therapies 4
 Range of initiatives to increase early access to effective psychological interventions – Training (and supervision) of more staff to deliver evidence based interventions – Restructuring services – Exploring alternatives to 1-to-1 therapies 4")
5
Low intensity interventions reduce the amount of time the practitioner is in contact with individual patients (Bennet-Levy, Richards & Farrand, 2010, p8) – Advice clinics (psycho-education) – Brief interventions – Group CBT (high volume approaches) – Guided and unguided self-help programmes supported in book/workbook format or delivered on computers/the internet 5
 – Advice clinics (psycho-education) – Brief interventions – Group CBT (high volume approaches) – Guided and unguided self-help programmes supported in book/workbook format or delivered on computers/the internet 5")
6
STEP 1 : All known and suspected presentations of depression STEP 2 : Persistent subthreshold depressive symptoms; mild to moderate depression STEP 3 : Persistent subthreshold depressive symptoms or mild to moderate depression with inadequate response to initial interventions; moderate and severe depression STEP 4: Severe and complex depression; risk to life; severe neglect Low-intensity psychosocial interventions, psychological interventions, medication and referral for further assessment and interventions Medication, high-intensity psychological interventions, combined treatments, collaborative care b and referral for further assessment and interventions Medication, high-intensity psychological interventions, electroconvulsive therapy, crisis service, combined treatments, multiprofessional and inpatient care Assessment, support, psychoeducation, active monitoring and referral for further assessment and interventions Focus of the intervention The stepped-care model for depression Nature of the intervention National Institute for Health and Clinical Excellence, 2009 6

7
NICE (2009) depression guidelines Low-intensity psychosocial interventions For people with persistent subthreshold depressive symptoms or mild to moderate depression, consider offering one or more of the following interventions, guided by the persons preference: – individual guided self-help workbooks based on the principles of cognitive behavioural therapy (CBT) – computerised cognitive behavioural therapy (CCBT) – a structured group physical activity programme. These should – be supported by a trained practitioner, who typically facilitates the self help programme and reviews progress and outcome – consist of up to six to eight sessions (face-to-face and via telephone) normally taking place over 9 to 12 weeks, including follow-up.
 normally taking place over 9 to 12 weeks, including follow-up..")
8
NICE indicated low intensity interventions for common mental health problems from http://www.iapt.nhs.uk/wp-content/uploads/iapt-data-handbook-appendices-v10.pdf See also NICE (2011) Guidance on Common Mental Health Disorders. NICE. NB IAPT services designed to deliver these guidelines, 3500 new workers etc Aim to identify and treat 100ks of people with anxiety and depression 8

9
NICE indicated low intensity interventions for common mental health problems from http://www.iapt.nhs.uk/wp-content/uploads/iapt-data-handbook-appendices-v10.pdf See also NICE (2011) Guidance on Common Mental Health Disorders. NICE. NB IAPT services designed to deliver these guidelines, 3500 new workers etc Aim to identify and treat 100ks of people with anxiety and depression 9

10
Increasing access to psychological therapies for common mental health problems such as depression, anxiety and insomnia 10

11
Outline What is computerised cognitive behavioural therapy (CCBT)? Evidence of effectiveness for CCBT Evidence of how best to support users CCBT journey Uptake Engagement / Adherence Completion and maintaining longer term outcomes Future research questions to be addressed 11

12
Computerised Cognitive Behavioural Therapies 12

13
Computerised Psychological Therapies A structured, interactive program which guides the user through a psychological intervention Computerised Cognitive Behavioural Therapy – Psycho-education – Assessment of current problems with feedback and change monitoring – Action plans and goals – Guided change techniques (e.g. behavioural activation, evaluating negative automatic thoughts, problem solving) – Putting learning into practice (homework) Accessed via interactive computing device, and usually via the internet –PC, smartphone, IVR, Tablet/Ipad Supported by trained healthcare staff –Trained in the delivery of low-intensity interventions –Typically brief, remote, weekly support sessions (by phone or email) 13
 – Putting learning into practice (homework) Accessed via interactive computing device, and usually via the internet –PC, smartphone, IVR, Tablet/Ipad Supported by trained healthcare staff –Trained in the delivery of low-intensity interventions –Typically brief, remote, weekly support sessions (by phone or ) 13.")
17
Colour your life

18
Swedish group

19
One example… www.beatingtheblues.co.uk

21
e.g. Behavioural Activation When? Where? Barriers? Feedback Guidance Psycho- education Case examples to help learning Genuineness Warmth Assessment Action planning Collaboration Negotiation of goals Guided discovery Monitoring Review

23
Multimedia which guides the user through the program and illustrates learning examples

25
Summary

30
Are these CCBT programs effective? Do they help users to make sense of their problems Do they lead to a reduction in difficulties and improved well being, sustained in the longer term? 30

31
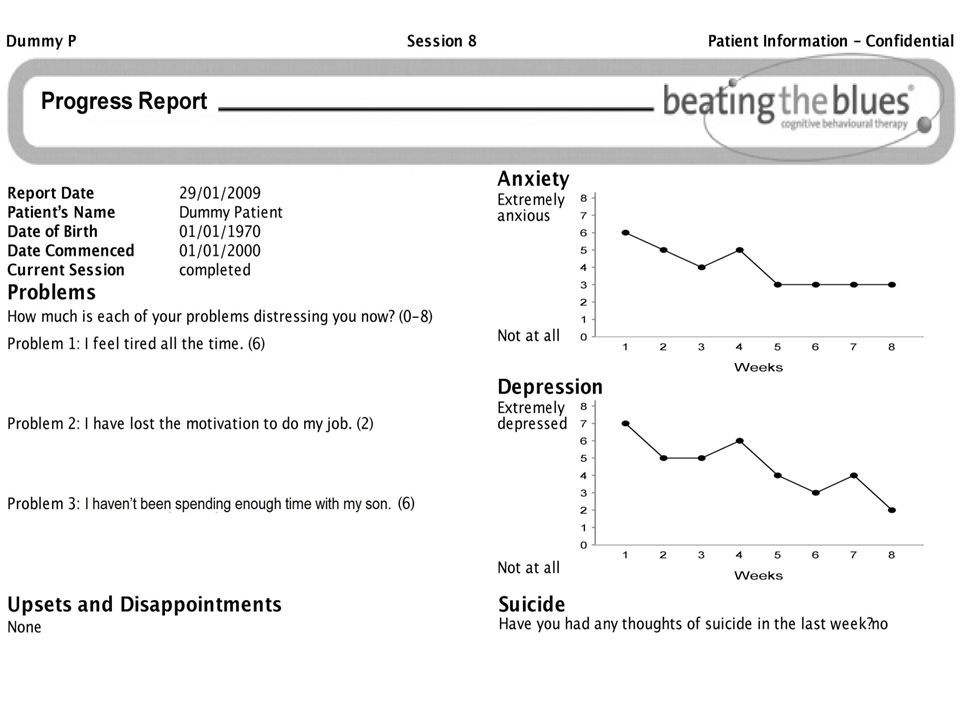
Randomised Controlled Trial: Beating the Blues vs usual care in NHS Primary Care GP patients aged 18-75 with depression and/or anxiety, with or without antidepressant medication 276 participants from 12 primary care practices Outcome measures: Beck Depression Inventory Beck Anxiety Inventory Work and Social Adjustment Scale Health Service Usage Pre, Post, 1 month, 3 month and 6 month follow- up Proudfoot et al (2004) British Journal of Psychiatry 31
 British Journal of Psychiatry 31")
32
N = 276 Proudfoot et al (2004) British Journal of Psychiatry Mean of 1 mo more DFD in 6 mo FU, Outcomes comparable to 8 FTF Sheff. 30 25 20 15 10 5 0 Computerised-CBT for Depression 32

33
Beck Anxiety Inventory Outcomes Pre Post 1 mo FU 3 mo FU 6 mo FU TAU Beating the Blues 20 15 10 5 0 N = 276 Proudfoot et al (2004) British Journal of Psychiatry 33
 British Journal of Psychiatry 33")
34
Work and Social Adjustment Scale 20 15 10 5 0 TAU Beating the Blues Pre Post 1 mo FU 3 mo FU 6 mo FU N = 276 Proudfoot et al (2004) British Journal of Psychiatry 34
 British Journal of Psychiatry 34")
35
Summary of RCT outcomes Beating the Blues offers clinical benefits over and above treatment at usual 2/3rds users complete all 8 sessions Intent-to-treat analysis shows that benefits are maintained to 6-months post treatment Outcome: cost ratios demonstrate that Beating the Blues is a cost-effective intervention for depression primary care Lost employment costs are significantly lower following Beating the Blues than treatment as usual McCrone, P., Knapp, M., Proudfoot, J., Cavanagh, K., Ryden, C., Ilson, S., Gray, JA, Shapiro, DA. (2004) British Journal of Psychiatry 35
 British Journal of Psychiatry 35.")
36
Further evidence of effectiveness of CCBT (Beating the Blues) for depression In routine primary care –(N=219, Cavanagh et al., 2006) In specialist CBT service (N=555; Learmonth et al., 2007) In student health services (Mitchell & Dunn, 2007; McHugh et al., 2010) In secondary care adult mental health service (N = 23; Ormrod et al., 2010) In service user led self-help clinic (N= 510, Cavanagh et al., 2011) 36
 for depression In routine primary care –(N=219, Cavanagh et al., 2006) In specialist CBT service (N=555; Learmonth et al., 2007) In student health services (Mitchell & Dunn, 2007; McHugh et al., 2010) In secondary care adult mental health service (N = 23; Ormrod et al., 2010) In service user led self-help clinic (N= 510, Cavanagh et al., 2011) 36")
37
Reviews of the evidence for CCBT Systematic review of the evidence identified 175 studies, including 103 RCTs evaluating the use of 97 different Computerised Psychotherapy programs 37

38
Evidence base for CCBT Some evidence of effectiveness (at least in comparison to a waitlist control) Marks, Cavanagh & Gega (2007) Phobias Phobias Panic Panic OCD OCD PTSD PTSD GAD GAD Stress Stress Depression Depression Eating disorders (BN) Eating disorders (BN) Problem drinking Problem drinking Substance misuse Substance misuse Pain Pain Tinnitus Tinnitus Insomnia Insomnia Sexual problems Sexual problems Schizophrenia Schizophrenia Childhood anxiety, depression, headaches, ASD, encopresis, asthma Childhood anxiety, depression, headaches, ASD, encopresis, asthma 38
 Marks, Cavanagh & Gega (2007) Phobias Phobias Panic Panic OCD OCD PTSD PTSD GAD GAD Stress Stress Depression Depression Eating disorders (BN) Eating disorders (BN) Problem drinking Problem drinking Substance misuse Substance misuse Pain Pain Tinnitus Tinnitus Insomnia Insomnia Sexual problems Sexual problems Schizophrenia Schizophrenia Childhood anxiety, depression, headaches, ASD, encopresis, asthma Childhood anxiety, depression, headaches, ASD, encopresis, asthma 38")
39
Meta-analysis of internet-based interventions (Barak et al, 2008) Internet Interventions versus control conditions: Weighted Mean Effect Size = 0.53 (64 articles, 92 studies reviewed) Internet Interventions versus face-to-face: no significant difference 39
 Internet Interventions versus control conditions: Weighted Mean Effect Size = 0.53 (64 articles, 92 studies reviewed) Internet Interventions versus face-to-face: no significant difference 39")
40
Meta-analysis of CCBT for Depression and Anxiety - Andrews et al 2010 Favours CCBT 40

41
Guided self help versus face to face CBT Cuijpers et al, 2010 41

42
Does CCBT work? Computerized treatments have been shown to be a less-intensive, cost- effective way to deliver empirically validated treatments for a variety of psychological problems 42

43
CCBT appears to be a good thing But – –Not everyone tries them 38% (range 4% - 83%) of those invited to CCBT research trial start program (Waller & Gilbody, 2008) –Not everyone sticks with them Meta-analysis of studies of CCBT for depression mean dropout rate 32% (range 0-75%; Kaltenthaler et al., 2008) –Professionals not always be hopeful about the value of self-help in the therapeutic context e.g. Whitfield and Williams, 2004; Stallard et al., 2010 43

44
How can we optimise the user experience of CCBT in order to increase access to and benefit from psychological therapies? 44

45
Turning on, tuning in and (not) dropping out UptakeEngagementCompletion CCBT programs can be effective, but how can we ensure that those who may benefit are able to make use of these programs? 45

46
The 4 ps of CCBT PatientProvider Program 46 Problem

47
The patient: who is suitable for CCBT? NICE recommends that anyone meeting criteria for GAD, panic, persistent subtheshold and mild- to-moderate depression should be offered the choice of CCBT –Willing and able criteria –No specific exclusion criteria (locally determined) e.g. high risk, primary substance/alcohol misuse There is no strong evidence to support the idea that younger people or males are more well suited to CCBT * 47
 e.g. high risk, primary substance/alcohol misuse There is no strong evidence to support the idea that younger people or males are more well suited to CCBT * 47.")
48
The patient: who is suitable? Pre-treatment expectancies predict treatment completion (Cavanagh et al, 2010) and longer term treatment outcomes (12 months FU; Graaf et al., 2010) MacLeod et al (2009) Higher levels of patient motivation, program credibility, likely adherence, self-efficacy and a lower degree of hopelessness associated with benefits from self-help programs Ongoing research exploring the influence of individual differences in attitudes to helpseeking, attachment orientation etc. 48
 and longer term treatment outcomes (12 months FU; Graaf et al., 2010) MacLeod et al (2009) Higher levels of patient motivation, program credibility, likely adherence, self-efficacy and a lower degree of hopelessness associated with benefits from self-help programs Ongoing research exploring the influence of individual differences in attitudes to helpseeking, attachment orientation etc. 48.")
49
The problem: what problems can be helped by CCBT? Both anxiety and depression (and others) The need for support may vary by disorder – Anxiety can benefit from unguided or minimally guided self-help – Depression may require additional support Newman et al (2011) Depression may be associated with reduced motivation, reduced activation, feelings of hopelessness and rumination – which may make it more difficult to engage with the programme (and CBT in general) – so more support needed 49
 The need for support may vary by disorder – Anxiety can benefit from unguided or minimally guided self-help – Depression may require additional support Newman et al (2011) Depression may be associated with reduced motivation, reduced activation, feelings of hopelessness and rumination – which may make it more difficult to engage with the programme (and CBT in general) – so more support needed 49.")
50
The program: which programs work? Evidence-based self-help interventions Untested programs based on the principles of CBT Program features to consider – Structure – Content: toolkit and techniques – Common factors (empathy, warmth, alliance, structure etc) 50
 50.")
51
Set menu or a la carte? Some evidence of improved adherence with greater structure (Celio et al, 2003) Preliminary evidence from Andersson (2010) suggests both models can work No head to head trials published Best evidence to date is for structured programs 51
 Preliminary evidence from Andersson (2010) suggests both models can work No head to head trials published Best evidence to date is for structured programs 51.")
52
Content: Whats in the box? Tools and guided change techniques Little dismantling evidence available to date on what specifically works in CCBT Matching the users needs and preferences Importance of familiarity with the materials 52

53
Common factors There is considerable evidence of common factors embedded within widely used CCBT programs (Barazzone, Cavanagh & Richards, under review) Users report a therapeutic alliance with CCBT programs (Ormrod et al., 2010) Ongoing research to understand more about these engagement processes 53
 Users report a therapeutic alliance with CCBT programs (Ormrod et al., 2010) Ongoing research to understand more about these engagement processes 53")
54
The provider: staff training and supportive context for CCBT Therapists with training in self-help are more confident and positive about self help (Keeley et al., 2002) Therapist expectancies and frequency of programme use are improved with training (McLeod et al., 2009) 54
 Therapist expectancies and frequency of programme use are improved with training (McLeod et al., 2009) 54")
55
Encouraging uptake and engagement, and reducing drop-out Identifying key problems and goals to work on Identifying appropriate self-help materials Supporting the person in their efforts to change Monitoring and review of progress From Baguley et al (2010) Good Practice Guidelines for Self-Help in IAPT Services. IAPT. 55

56
Phone or email support for CCBT A scheduled 10 minute contact, once a week –Service users tend not to call helplines (e.g. Kenwright et al., 2004) Remote services supported by phone confer similar outcome and satisfaction to same programs in CCBT clinic (MacKinnon et al., 2008) No added value to more frequent contact (Klein et al., 2009) No added value to using >1 medium of communication (Andersson et al., 2003) Andersson et al (2009) A clear deadline provided for the duration of the treatment improves program completion Reminders sent by post-card, email, telephone or text may have an impact on program adherence and on outcome (Clarke et al., 2005) 56
 Remote services supported by phone confer similar outcome and satisfaction to same programs in CCBT clinic (MacKinnon et al., 2008) No added value to more frequent contact (Klein et al., 2009) No added value to using >1 medium of communication (Andersson et al., 2003) Andersson et al (2009) A clear deadline provided for the duration of the treatment improves program completion Reminders sent by post-card, , telephone or text may have an impact on program adherence and on outcome (Clarke et al., 2005) 56.")
57
Managing expectations Peoples mental model of accessing psychological support or therapy may differ from the guided self-help treatment option –I didnt expect homework –I suppose I thought it would be some sort of counselling… –I wasnt sure about their [assistant psychologist] role. I didnt realise that she was going to work through the book with me –I dont know how long the sessions were supposed to be Macdonald et al., 2007 57
![Managing expectations Peoples mental model of accessing psychological support or therapy may differ from the guided self-help treatment option –I didnt expect homework –I suppose I thought it would be some sort of counselling… –I wasnt sure about their [assistant psychologist] role.](http://images.slideplayer.com/3/795843/slides/slide_57.jpg "I didnt realise that she was going to work through the book with me –I dont know how long the sessions were supposed to be Macdonald et al.,")
58
Managing expectations User expectancies can be improved by a taster session with CCBT programs (Mitchell and Gordon, 2007) Novel features of the guided self-help service should be made explicit and rehearsed e.g. –The programme structure and content –The primary wellbeing practitioner role –What to expect from scheduled phone support –Session length (programme and support) and work in between sessions –Ongoing monitoring and review etc 58
 and work in between sessions –Ongoing monitoring and review etc 58.")
59
Drop out from CCBT Meta-analysis of studies of CCBT for depression mean dropout rate 32% (range 0-75%; Kaltenthaler et al., 2008) Reasons for drop out from CCBT –Too busy / change of circumstances –Early gains / accomplishment of goals –Dissatisfaction with therapy or CCBT No significant difference in dropout rates between guided self help and FTF therapies in head-to-head RCTS (RRR = 1.14; Cuipers et al., 2010) Managing expectations, program matching, planned endings, progress review and strategies for managing difficulties with engagement may support completion 59
 Reasons for drop out from CCBT –Too busy / change of circumstances –Early gains / accomplishment of goals –Dissatisfaction with therapy or CCBT No significant difference in dropout rates between guided self help and FTF therapies in head-to-head RCTS (RRR = 1.14; Cuipers et al., 2010) Managing expectations, program matching, planned endings, progress review and strategies for managing difficulties with engagement may support completion 59")
60
Summary CCBT can offer an effective method of treatment for depression and anxiety Promoting uptake, engagement, and completion are key provider tasks. Chose programs with evidence of effectiveness Information, taster sessions and training help Brief weekly support is vital Reminders and prompts may also help There is lots more research to be done! 60

61
Selected books 61

62
Good practice guidance for use of self-help Baguley, C., Farrand, P., Hope, R., Leibowitz, J., Lovell, K., Lucock, M., ONeill, C., Paxton, R., Pilling, S., Richards, D., Turpin, G., White, J. and Williams, C. (2010) Good practice guidance on the use of self-help materials within IAPT services. Technical Report. IAPT This version is available at http://eprints.hud.ac.uk/9017/ 62
 Good practice guidance on the use of self-help materials within IAPT services. Technical Report. IAPT This version is available at")
63
Home pages of some evidence based CCBT programs –www.ccbt.co.uk –www.ccbt.co.uk – fearfighter, ocfighter, copewww.ccbt.co.uk –www.beatingtheblues.co..uk –www.beatingtheblues.co..uk – beating the blueswww.beatingtheblues.co..uk –www.livinglifetothefull.com –www.livinglifetothefull.com – living life to the fullwww.livinglifetothefull.com –www.moodgym.anu.edu.au –www.moodgym.anu.edu.au - moodgymwww.moodgym.anu.edu.au –www.anxietyonline.com – various programs for anxiety problemswww.anxietyonline.com –www.calipso.co.uk –www.calipso.co.uk – overcoming depression, overcoming bulimiawww.calipso.co.uk –www.interapy.nl –www.interapy.nl – various programs for stress, anxiety, depressionwww.interapy.nl –www.livanda.se –www.livanda.se – various programs for stress, anxiety, depressionwww.livanda.se 63

64
Thanks! kate.cavanagh@sussex.ac.uk Interactive Well-being Lab www.sussex.ac.uk/iwl Cavanagh, K (2010) Turning on, tuning in and (not) dropping out. In J. Bennett-Levy (Ed). Oxford Guide to Low Intensity CBT Interventions. Oxford University Press: Oxford, UK. 64
 Turning on, tuning in and (not) dropping out. In J. Bennett-Levy (Ed). Oxford Guide to Low Intensity CBT Interventions. Oxford University Press: Oxford, UK. 64.")
Similar presentations














 patients Policy.>")











