Download presentation
Presentation is loading. Please wait.

1
Medical Mycology Systemic Mycoses
Hugh B. Fackrell Filename; fungi_system.ppt

2
Fungal Infections Systemic Mycoses Opportunistic Infections
Superficial fungal infections Cutaneous Mycoses Subcutaneous Mycoses Systemic Mycoses

3
Systemic or Deep Mycoses
Histoplasmosis Coccidiomycosis Blastomycosis Cryptococcosis

4
Histoplasmosis before HIV
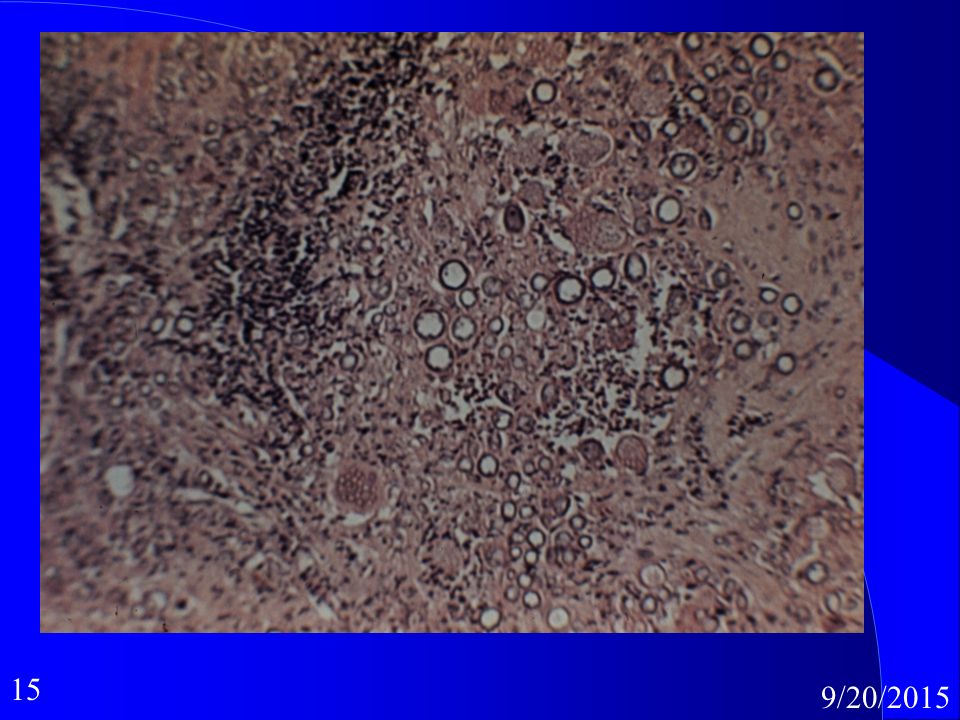
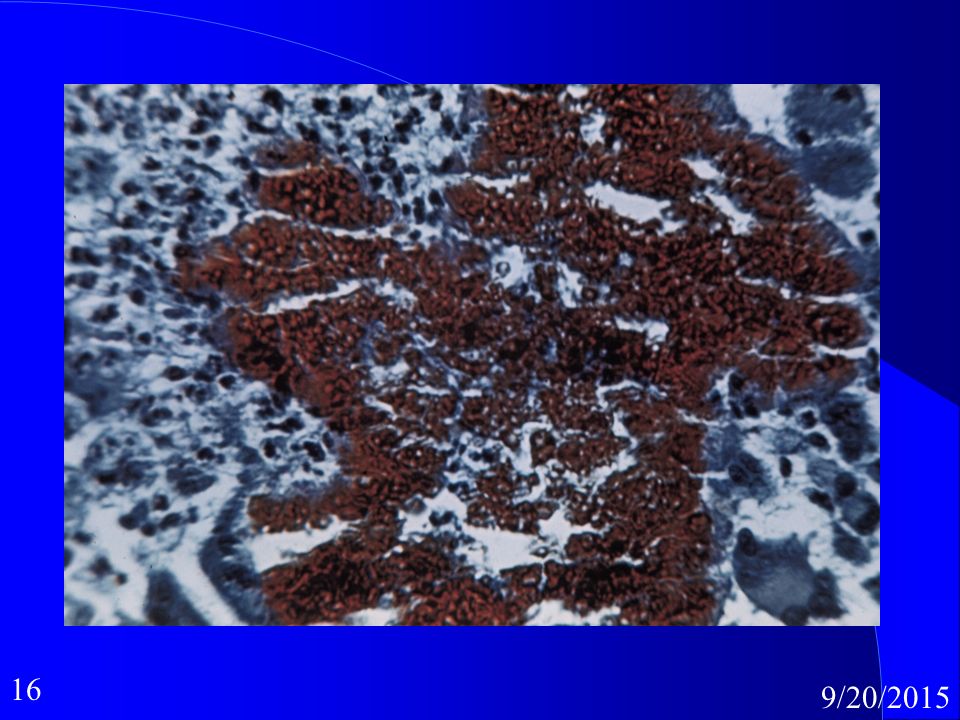
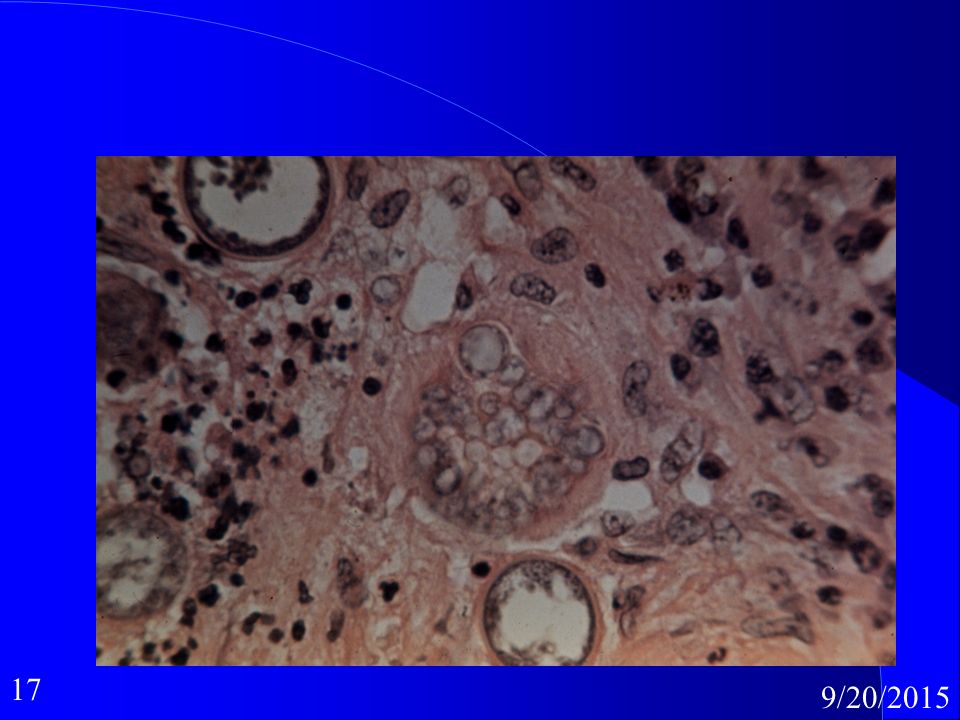
Before the appearance of HIV, approximately 95% of the cases reported of histoplasmosis capsulati where inapparent, subclinical, or benign and five percent of them where a chronic progressive lung disease with chronic cutaneous or systemic disease, or an acute fulminating fatal systemic disease. Histoplamosis capsulati Synonyms North American histoplasmosis Definition Before the appearance of HIV, approximately 95% of the cases reported of histoplasmosis capsulati where inapparent, subclinical, or benign and five percent of them where a chronic progressive lung disease with chronic cutaneous or systemic disease, or an acute fulminating fatal systemic disease. After the appearance of HIV the disease is almost always seen in HIV positive patients or other immunocompromised individuals. All stages of this disease may mimic tuberculosis. Histoplasmosis may coexist with actinomycosis, other mycoses, sarcoidosis, or tuberculosis. Forms of the disease Disseminated Pulmonary Prognosis and therapy Disseminated, chronic cavitary, mucocutaneous, or systemic disease require therapy. Amphotericin B is the drug of choice and recovery is typically fast with essentially no relapse if adequate drug is given and the patient has no underlying debilitating disease. Itraconazole and voriconazole can be considered. Fluconazole is used in AIDS patients. Histopathology The histopathological picture in acute disseminated histoplasmosis is different from that seen in the more chronic disease, and in solitary pulmonary nodules ("coin lesion"). In the first entity, Histoplasma capsulatum var. capsulatum is localized in histiocytes and eticuloendothelial cells. The cells enlarge, but with no evidence of inflammation. The intracellular budding yeasts are approximately 3 µm in diameter , similar to Leishmania sp., but do not contain a kinetoplast. In addition, Leishmania does not stain with the special stains use for fungi. Older lesions are well-developed granulomata and have a central area of caseation resembling tuberculosis. The solitary pulmonary nodules are well organized and usually have a circumferential rim of calcification accounting for its visibility on chest X-ray. Fungi within these nodules are usually dead. Histoplasma capsulatum cells are found in the center of the lesions. Laboratory Direct examination The direct detection of fungi in clinical material such as bone marrow, sputum, and tissue is usually difficult. Material stained by the PAS, Giemsa, GMS or cellufluor methods are superior to KOH preparations. Isolation Inoculate the clinical material onto Inhibitory Mould agar and or yeast extract-phosphate agar and or BHI agar with 10% sheep blood and or a medium containing cycloheximide. Incubate cultures at 30° and do not discard until 12 weeks. Laboratory confirmation Confirmation is necessary to ensure that the fungus is not a species of Chrysosporium or Sepedonium. This can be accomplished by the mould to yeast convertion, exoantigen technique or by DNA probes. Mycology Histoplasma capsulatum var. capsulatum Ajellomyces capsulatus (sexual form)
. In the first entity, Histoplasma capsulatum var. capsulatum is. localized in histiocytes and eticuloendothelial cells. The cells enlarge, but with no. evidence of inflammation. The intracellular budding yeasts are approximately 3. µm in diameter , similar to Leishmania sp., but do not contain a kinetoplast. In. addition, Leishmania does not stain with the special stains use for fungi. Older. lesions are well-developed granulomata and have a central area of caseation. resembling tuberculosis. The solitary pulmonary nodules are well organized and. usually have a circumferential rim of calcification accounting for its visibility on. chest X-ray. Fungi within these nodules are usually dead. Histoplasma. capsulatum cells are found in the center of the lesions. Laboratory. Direct examination. The direct detection of fungi in clinical material such as bone marrow, sputum, and tissue is usually difficult. Material stained by the PAS, Giemsa, GMS or. cellufluor methods are superior to KOH preparations. Isolation. Inoculate the clinical material onto Inhibitory Mould agar and or yeast. extract-phosphate agar and or BHI agar with 10% sheep blood and or a medium. containing cycloheximide. Incubate cultures at 30° and do not discard until 12. weeks. Laboratory confirmation. Confirmation is necessary to ensure that the fungus is not a species of. Chrysosporium or Sepedonium. This can be accomplished by the mould to yeast. convertion, exoantigen technique or by DNA probes. Mycology. Histoplasma capsulatum var. capsulatum. Ajellomyces capsulatus (sexual form)")
5
Histoplasmosis After HIV
Now the disease is almost always seen in HIV positive patients or other immunocompromised individuals. All stages of this disease may mimic tuberculosis. Histoplasmosis may coexist with actinomycosis, other mycoses, sarcoidosis, or tuberculosis.

6
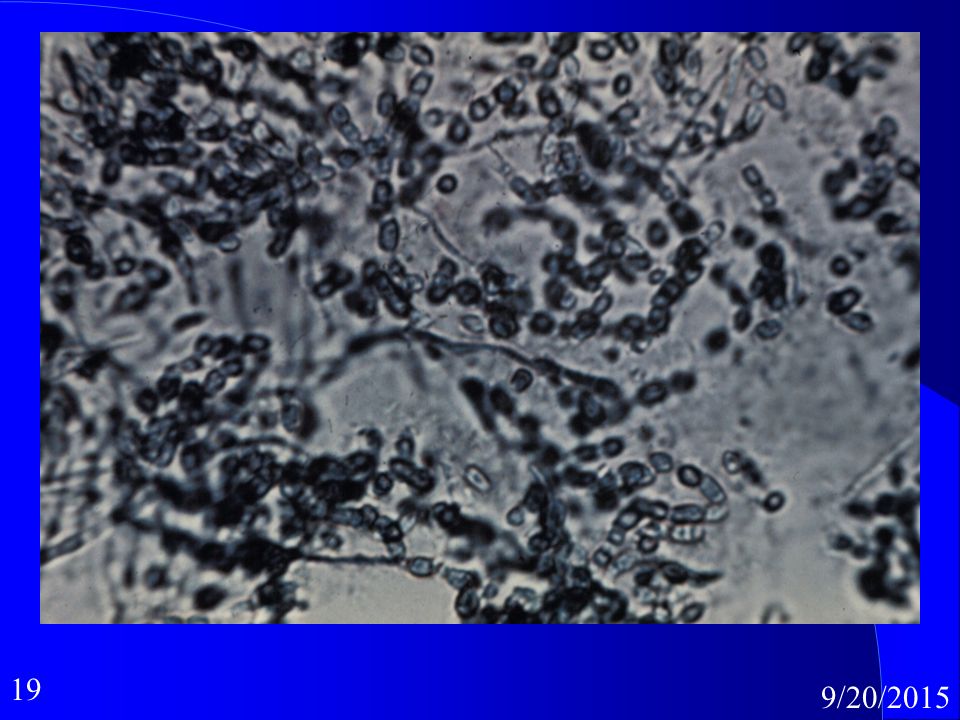
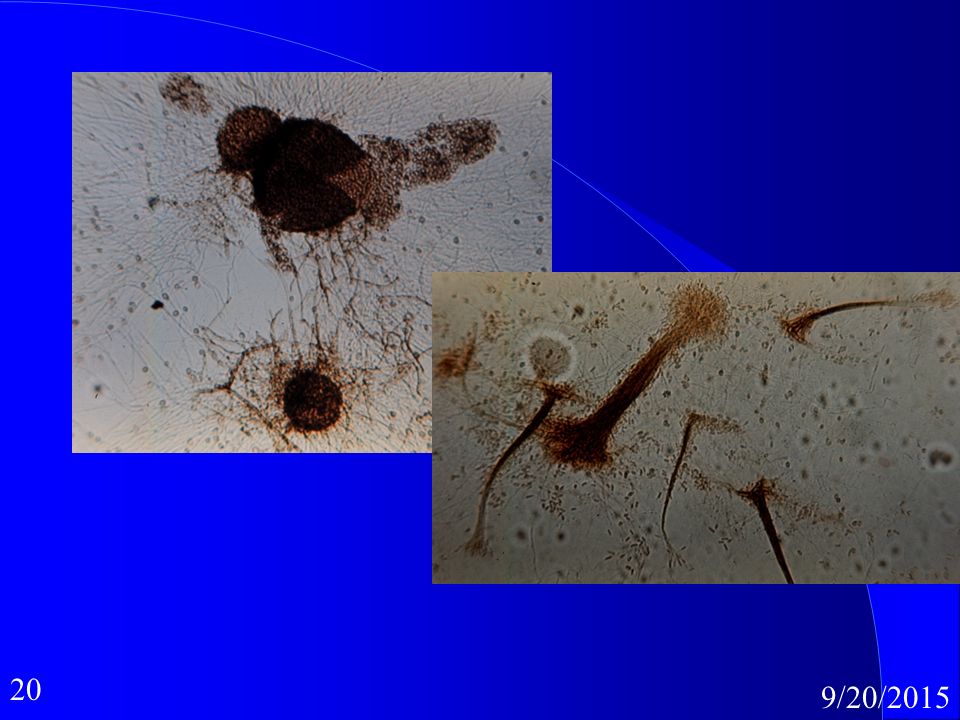
Histoplasmosis Histoplasma capsulatum Ohio,Mississippi valleys

8
v

9
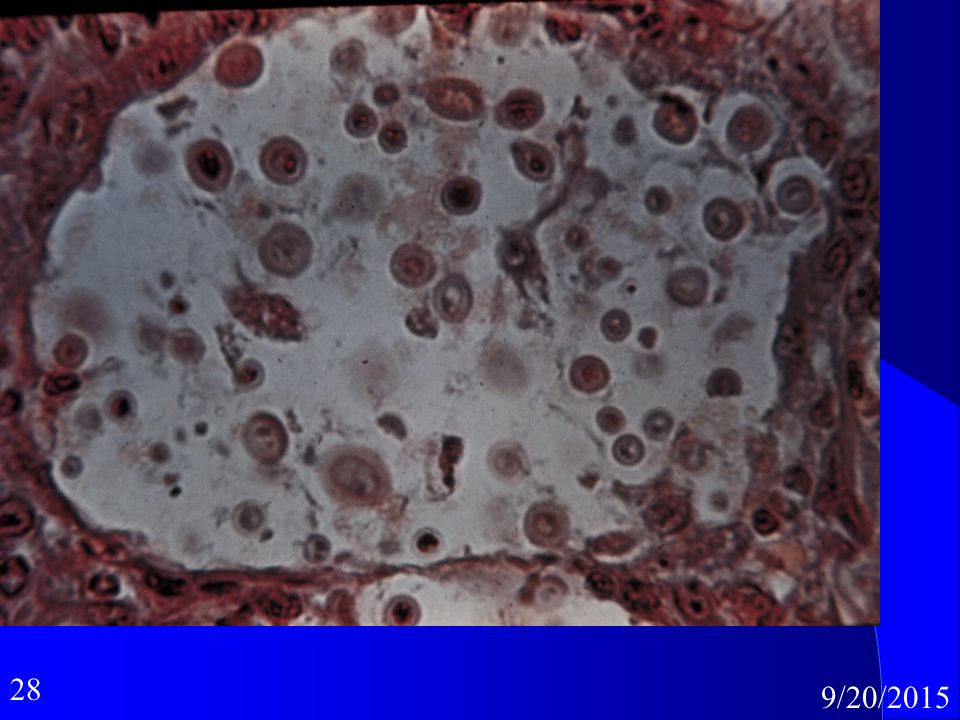
Coccidiomycosis SW deserts, San Joaquin Coccidioides immitus
Coccidioidomycosis Synonyms San Joaquin Valley fever, Valley fever Definition Coccidioidomycosis is a respiratory infection that typically resolves rapidly. The mycosis can become acute, chronic, severe, or fatal. The disease may result in a chronic pulmonary condition or disseminate to the meninges, bones, joints, and subcutaneous and cutaneous tissues. The initial tissue response in rapidly disseminating disease is suppuration, whereas chronic and advancing infections are characterized by a granulomatous reaction with some areas being a mixed-type cellular response. It is believed that recovery results in immunity to reinfection. Approximately 60% of patients with primary infections are asymptomatic, 40% have mild to acute pulmonary disease and approximately 0.5% develop serious disease. About 25% of the patients with disseminated disease have meningitis. Forms of the disease Primary ( Pulmonary , Cutaneous), Secondary ( Pulmonary , Disseminated ) Prognosis and therapy Primary coccidioidomycosis is treated with bed rest and restricted activity. Steroids may be used to control allergic reactions. Untreated secondary disease has a grave prognosis. The drug of choice is amphotericin B. Meningitis usually requires intrathecal as well as intravenous administration of amphotericin B. 5-Fluorocytosine has little value in the treatment of coccidioidomycosis. Itraconazole, fluconazole, ketoconazole and voriconazole should be considered. Histopathology The tissue reaction is acute suppurative and granulomatous inflammation. Acute suppuration is usually present around the arthroconidia and after a spherule ruptures. Granulomatous inflammation usually occurs around developing spherules. Hyphae may be present in pulmonary cavities and meningeal lesions without arthroconidia, which can lead to confusion wih the hyphae of an Aspergillus sp. Laboratory Direct examination Directo examination of clinical specimens, such as fluids, sputa, and tissue, in 10% KOH may show spherules um in diameter with a thick wall (up to 2 um) and endospores 2-5 um in diameter characteristic of Coccidioides immitis. Endospores are released when the wall of the spherule ruptures. Endospores that are no longer in a spherule may remain closely appressed to each other, resulting in a potential confusion with the yeast cells of Blastomyces dermatitidis. This is especially true if the spherule wall is no longer visible and the clinical specimen has been homogenized. Isolation Isolation involves inoculating the clinical material onto IMA agar, BHI agar with 10% sheep blood and a medium containing cycloheximide and incubate at 30C. Cultures should be kept 4 weeks before discarding as negative. The fungus is fast growing and readily produces barrel-shaped arthroconidia 2.5-4 x 3-6 um with a disjunctor cell between each arthroconidium. Coccidioides immitis is a dangerous fungus and should be handled at all times with due respect in a Class II or III biological safety cabinet. It is classified as a BSL-3 agent. Laboratory confirmation of C. immitis is required because other fungi, such as members of the Gymnoascaceae, may develop an anamorph similar to Coccidioides. In vitro procedures including special conversion media, exoantigen test or DNA probes. Slide cultures should not be set up when Coccidioides immitis is suspected due to its dangerous nature. Mycology Coccidioides immitis Natural habitat Alkaline soil of the Lower Sonoran Life Zone in North, Central, and South America.
, Secondary ( Pulmonary , Disseminated ) Prognosis and therapy. Primary coccidioidomycosis is treated with bed rest and restricted activity. Steroids may be used to control allergic reactions. Untreated secondary. disease has a grave prognosis. The drug of choice is amphotericin B. Meningitis usually requires intrathecal as well as intravenous administration of. amphotericin B. 5-Fluorocytosine has little value in the treatment of. coccidioidomycosis. Itraconazole, fluconazole, ketoconazole and voriconazole. should be considered. Histopathology. The tissue reaction is acute suppurative and granulomatous inflammation. Acute suppuration is usually present around the arthroconidia and after a. spherule ruptures. Granulomatous inflammation usually occurs around. developing spherules. Hyphae may be present in pulmonary cavities and. meningeal lesions without arthroconidia, which can lead to confusion wih the. hyphae of an Aspergillus sp. Laboratory. Direct examination. Directo examination of clinical specimens, such as fluids, sputa, and tissue, in. 10% KOH may show spherules um in diameter with a thick wall (up to. 2 um) and endospores 2-5 um in diameter characteristic of Coccidioides. immitis. Endospores are released when the wall of the spherule ruptures. Endospores that are no longer in a spherule may remain closely appressed to. each other, resulting in a potential confusion with the yeast cells of. Blastomyces dermatitidis. This is especially true if the spherule wall is no. longer visible and the clinical specimen has been homogenized. Isolation. Isolation involves inoculating the clinical material onto IMA agar, BHI agar. with 10% sheep blood and a medium containing cycloheximide and incubate. at 30C. Cultures should be kept 4 weeks before discarding as negative. The. fungus is fast growing and readily produces barrel-shaped arthroconidia x 3-6 um with a disjunctor cell between each arthroconidium. Coccidioides. immitis is a dangerous fungus and should be handled at all times with due. respect in a Class II or III biological safety cabinet. It is classified as a BSL-3. agent. Laboratory confirmation of C. immitis is required because other fungi, such as members of the Gymnoascaceae, may develop an anamorph similar to. Coccidioides. In vitro procedures including special conversion media, exoantigen test or DNA probes. Slide cultures should not be set up when. Coccidioides immitis is suspected due to its dangerous nature. Mycology. Coccidioides immitis. Natural habitat. Alkaline soil of the Lower Sonoran Life Zone in North, Central, and South. America.")
10
Valley Fever

21
Blastomycosis Blastomyces dermatitidi as histo but rarer.
Canada- Manitoba and St.Lawrence river valley Disease in horses. Veternarians at risk. Blastomycosis Synonyms Chicago disease, Gilchrist's disease, North American Blastomycosis Definition Blastomycosis may be a benign and self-limiting infection or a chronic granulomatous and suppurative mycosis in which the primary infection is initiated in the lungs with frequent, subsequent dissemination to other body sites, especially the skin and bone. The disease is most prevalent in males years of age and in children. Blastomycosis may coexist with bronchogenic carcinoma, histoplasmosis, severe pulmonary disease, or tuberculosis. Forms of the disease Chronic cutaneous and osseous Primary pulmonary Systemic Prognosis and therapy Therapy is necessary. Amphotericin B is the drug of choice, and at least 1.5 gm must be given to avoid relapse. Hydroxystilbamidine has been used with success in treating the cutaneous form of the disease, but is of limited value in treating other forms of blastomycosis. Itraconazole and voriconazole should be considered. Histopathology The tissue response is a combination of acute suppurative and granulomatous inflammation. These may vary proportionately from one person to another and from one site to another in the same individual. The lung generally has widespread granulomatous inflammation with small areas of abscess formation. Fungi are usually demonstratable at the edge of the abscess. Skin involvement typically shows pseudoepitheliomatous hyperplasia with focal microabscesses in the papillary dermis. The yeast cells are globose to ovoid in shape and approximately 8-15 um in diameter. The single blastoconidium is attached by a broad base to the parent cell. In most instances, predominantly single cells without attached blastoconidia are seen. The cell wall of the yeast is thick and appears doubly refractile. Laboratory Direct examination Clinical material, such as fluids, prostate fluid, sputa, or tissue, is examined in 10% KOH . The fungus usually occurs as a thick-walled, globose yeast that measures 8-15 um in diameter. Some yeast cells have been reported to be up to 30 um in diameter. The fungus may also form yeast cells that are less than 8 um in diameter. Each blastoconidium is attached to the parent cell by a broad base. Owing to their size, Blastomyces dermatitidis could be confused with Coccidioides immitis or Cryptococcus neoformans under some circumstances. Isolation Inoculate the clinical material onto Sabouraud glucose agar, brain heart infusion agar, yeast-extract-phosphate agar, and a medium with cycloheximide, and then incubate at 30C. The cultures should be kept 4 weeks before discarding as negative. Blastomyces dermatitidis grows best on the yeast extract agar or agar containing yeast extract such as Mould Inhibitory Agar (IMA). Laboratory confirmation The mould form to yeast form conversion is necessary to ensure that the fungus suspected to be B. dermatitidis is not a similar fungus, such as a species of Chrysosporium or Sepedonium. The mould to yeast conversion can be readily accomplished by inoculating Kelley's agar or blood agar supplemented with glutamine and then incubating the inoculated tubes at 37C. The yeast form will begin to develop within a few days. The entire colony does not have to be converted to the yeast form in order to consider the fungus to be B. dermatitidis. An exoantigen technique and a DNA culture confirmation kit are available. Mycology Blastomyces dermatitidis Ajellomyces dermatitidis (sexual form) Natural habitat Unknown Sensitivity Testing
. Laboratory confirmation. The mould form to yeast form conversion is necessary to ensure that. the fungus suspected to be B. dermatitidis is not a similar fungus, such as a species of Chrysosporium or Sepedonium. The mould to. yeast conversion can be readily accomplished by inoculating. Kelley s agar or blood agar supplemented with glutamine and then. incubating the inoculated tubes at 37C. The yeast form will begin to. develop within a few days. The entire colony does not have to be. converted to the yeast form in order to consider the fungus to be B. dermatitidis. An exoantigen technique and a DNA culture. confirmation kit are available. Mycology. Blastomyces dermatitidis. Ajellomyces dermatitidis (sexual form) Natural habitat. Unknown. Sensitivity Testing.")
27
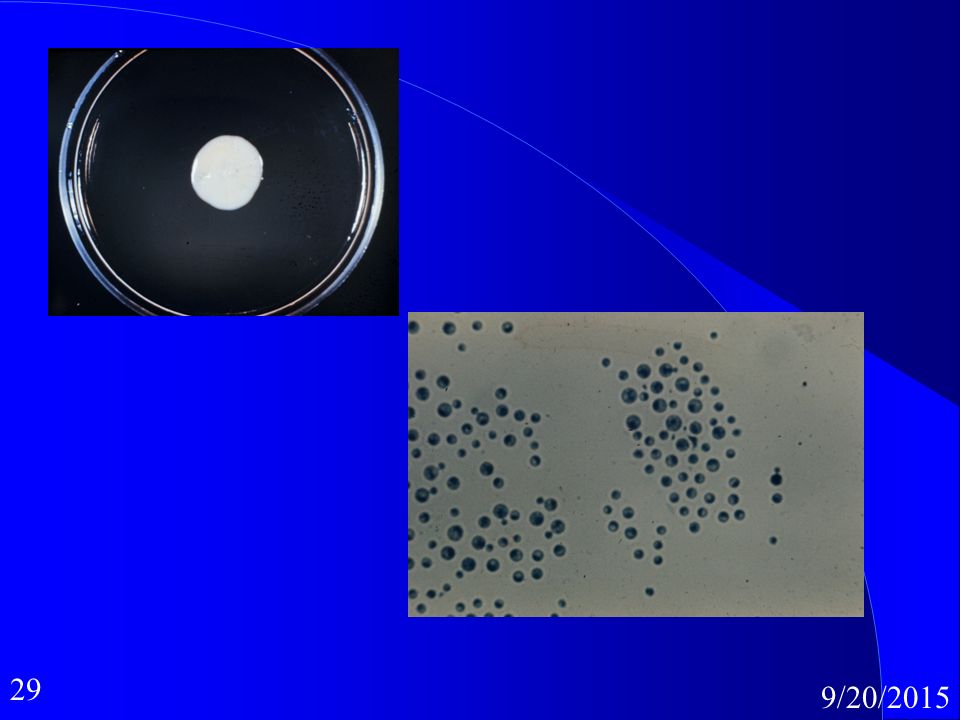
Cryptococcosis Cryptococcus neoformans Sporadic Pigeons
Meningitis form fatal Cryptococcosis Synonyms European blastomycosis, torulosis Definition Cryptococcosis is a chronic, subacute to acute pulmonary, systemic, or meningitic disease. The primary infection is in the lungs. Following inhalation of the fungus, the primary infection may remain localized or disseminate. On dissemination, the fungus usually shows a predilection for the central nervous system. Primary pulmonary infections have no diagnostic symptoms and usually are asymptomatic. Central nervous system disease is in the form most frequently diagnosed. Forms of the disease Central nervous system Cutaneous and mucocutaneous Osseous Pulmonary Visceral Prognosis and therapy Localized pulmonary lesions in noncompromised patients have a good prognosis. They usually heal without treatment. Hematogenous spread to the central nervous system has a grave prognosis unless treated immediately. Systemic infections are usually fatal, especially in debilitated patients, whereas primary cutaneous or mucocutaneous lesions typically resolve spontaneously. Chronic disease is usually characterized by alternating intervals of remission and exacerbation, but eventually is fatal. Amphotericin B is the drug of choice. Chronic pulmonary lesions and osteal lesions may be managed by surgical excision. Many strains rapidly develop resistance to 5-fluorocytosine during chemotherapy, hence susceptibility testing is required. 5-Fluorocytosine and amphotericin B are used concurrently in the treatment of meningitis. Fluconazole has use in AIDS for meningitis. Histopathology The tissue reaction is initially a myxoid degeneration with the area of inflammation assuming a gelatinous appearance. Large numbers of round yeast cells are found in the mucoid matrix. As the lesion progresses, a granulomatous reaction ensues. Organisms decrease numerically and are usually found in giant cells and histiocytes. In old healed granulomata, the yeasts are usually dead with disintegrated capsules. They may be difficult to see in H & E stained slides. The yeasts are round, typically encapsulated, and 5-15 um in diameter. The blastoconidia are attached by a narrow neck. The capsules stain pink by the mucicarmine technique. Laboratory Direct examination Globose yeast cells are easily seen in most clinical materials, such as cerebrospinal fluid and pulmonary tissue mounted in 10% KOH or India ink. A capsule may or may not be present. Isolation Inoculate aspirates and tissue (processed in tissue homogenizer) onto Sabouraud glucose agar, Inhibitory Mould agar and or Brain heart infusion agar and incubate at 30C. Cryptococcus neoformans is sensitive to cycloheximide. Growth is usually present in 2-5 days. Spinal fluid should be processed by a filtration or centrifugation technique. Mycology Cryptococcus norformans Filobasidiella neoformans (sexual form) Natural habitat Fruit, pigeon manure, plants Sensitivity Testing
 onto Sabouraud glucose agar, Inhibitory Mould agar and or Brain. heart infusion agar and incubate at 30C. Cryptococcus neoformans. is sensitive to cycloheximide. Growth is usually present in 2-5 days. Spinal fluid should be processed by a filtration or centrifugation. technique. Mycology. Cryptococcus norformans. Filobasidiella neoformans (sexual form) Natural habitat. Fruit, pigeon manure, plants. Sensitivity Testing.")
31
Click on image for more details
Click on image for more details

32
Systemic Mycoses: Disease Patterns
Subacute respiratory infection Acute infection Severe disseminated infection

33
Systemic Mycoses: Subacute Respiratory Infection
Low fever Non-productive cough Mild & self limiting

34
Systemic Mycoses: Acute Infections
Productive cough purulent sputum pain in chest Weight loss. night sweats X-ray positive one,many lesions consolidation Differential diagnosis: pneumonia, tumour.

35
Systemic Mycoses: Severe Disseminated Infections
Acute Infections + spread to other organs chronic Differential diagnosis t.b.

36
Systemic Mycoses: Diagnosis
X-ray Immunochemical skin test serology Microscopy Sputum biopsy autopsy

37
Systemic Mycoses: Transmission
Fungal spores inhaled ...pneumonitis..no human to human transmission Primary source bird and bat droppings and roosts. If roosts disturbed- dust, aerosol . Chickens, Pigeons,starlings.

38
Systemic Mycoses: Treatment
Amphotericin B and/or 5-fluorocytosine

Similar presentations