Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم Noushin Afshar Moghaddam, M.D
Associate Professor of Medicine Pathology Department Isfahan University of Medical Sciences

2
Fatty liver

3
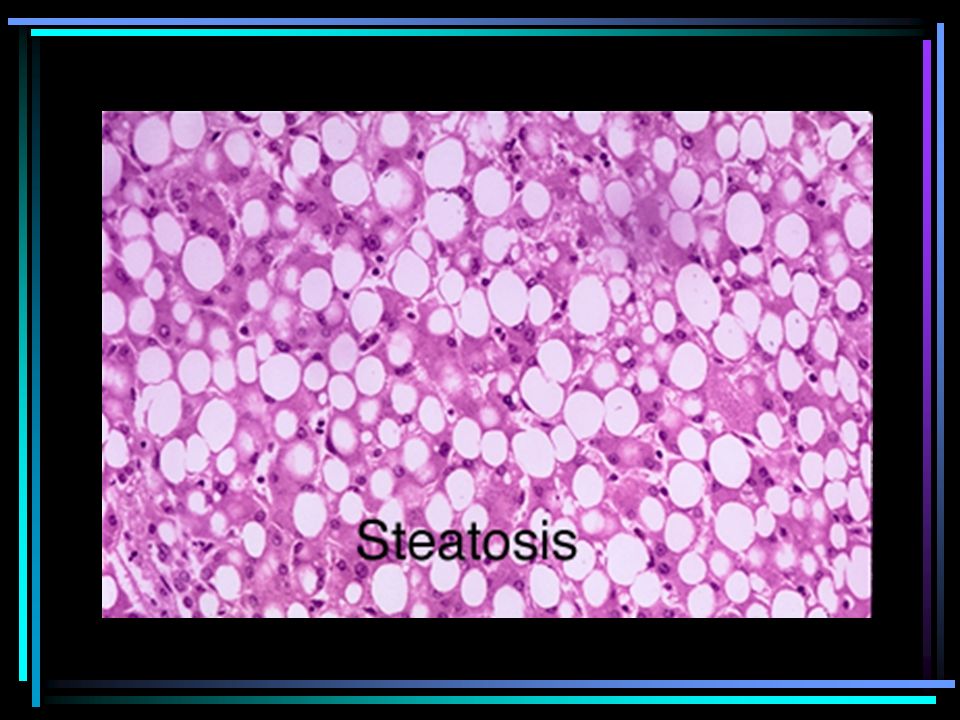
Steatosis Steatosis (fatty liver, fatty change) corresponds to accumulation of triglycerides in the cytoplasm of hepatocytes. It is a frequent finding and represents a manifestation of reversible cell injury
 corresponds to accumulation of triglycerides in the cytoplasm of hepatocytes. It is a frequent finding and represents a manifestation of reversible cell injury.")
4
Fatty Liver Any amount of fat in liver histology
Mirovesicular or macrovesicular With or without inflammation With or without fibrosis Associated with other disease or not Alcohol related or not Alcoholic fatty liver / Non alcoholic fatty liver

5
Steatosis is a nonspecific lesion induced by a variety of causes.
The degree of lipid accumulation is variable, ranging from occasional fat droplets to diffuse deposition involving most parenchymal cells. Minor amounts of steatosis are of uncertain significance, and occur more frequently in elderly people, possibly as part of the aging process. More extensive steatosis is seen in a variety of primary hepatic diseases and ,in several systemic conditions.

6
Histologic preparation
Histologically, in routinely fixed tissue, steatosis is represented by cytoplasmic vacuoles as the lipid is dissolved during processing. Very small droplet steatosis may be difficult to recognize. Lipid can be demonstrated in frozen sections using oil red 0, or Sudan black, or in tissue that has been postfixed in osmium tetroxide.

7
Patterns and distribution
Macrovesicular and microvesicular steatosis. Both may occur together to some extent in the same biopsy specimen, suggesting that large droplets form through coalescence of small lipid vacuoles.

9
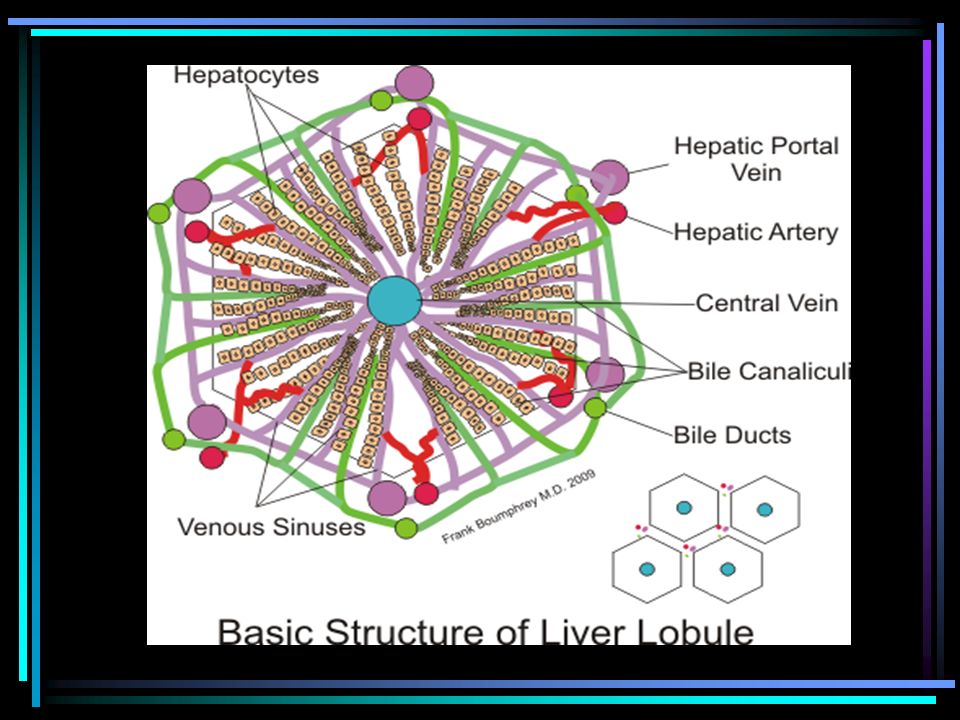
Normal liver 3 2 1

10
Normal liver

11
Normal liver

13
Acute fatty liver of pregnancy
Acute fatty liver of pregnancy. Detail of lobular parenchyma characterized by microvesicular steatosis and a small number of lymphocytes. (H&E)
")
14
Macrovesicular steatosis (large droplet fatty change)
It is the most common pattern. Uncomplicated macrovesicular steatosis used to be regarded as a benign and potentially fully reversible lesion, but this notion has been challenged Its zonal distribution is variable. It is most often centrolobular, :alcoholic liver disease, obesity, and diabetes. In more severe degrees, the steatosis may become panlobular. Steatosis in periportal zones is more commonly seen in cachexia and protein-energy malnutrition (kwashiorkor), in acquired immune deficiency syndrome (AIDS), after total parenteral nutrition, with phosphorus poisoning, and in steroid therapy.
, in acquired immune deficiency syndrome (AIDS), after total parenteral nutrition, with phosphorus poisoning, and in steroid therapy.")
15
There are exceptions to the rule,however, and it is not possible to define the etiology solely on the pattern of lipid distribution in the individual case. Identification of the cause requires close clinicopathologic correlation.

16
What’s the pathologist role?
The pathologist should provide information on severity by indicating the approximate amount of parenchyma involved (mild: less than one third; moderate: one third to two thirds; severe: more than two thirds). Further useful information for the clinician is the finding of a mixed pattern of macro- and microvesicular steatosis because this may be of prognostic importance in relation to alcoholic liver disease.
. Further useful information for the clinician is the finding of a mixed pattern of macro- and microvesicular steatosis because this may be of prognostic importance in relation to alcoholic liver disease.")
17
Pathogenesis The pathogenesis of steatosis is complex.
Alterations at many points of the complicated pathway of lipid metabolism can lead to accumulation of neutral fat within hepatocytes.

18
Microvesicular steatosis (small droplet fatty change)
It is often more difficult to recognize, and its demonstration may require histochemistry. It is generally a serious lesion associated with impairment of β-oxidation of lipids and frequently accompanied by disturbed liver function and coma.

19
Microvesicular steatosis (small droplet fatty change)
The causes are multiple. Acute fatty liver of pregnancy Reye's syndrome Salicylates Sodium valproate Intravenous high dose tetracycline Ethanol (in a small proportion of patients) Inborn errors of mitochondrial fatty acid β-oxidation Inherited urea cycle disorders
 Inborn errors of mitochondrial fatty acid β-oxidation. Inherited urea cycle disorders.")
21
Classification of fatty liver disease
Alcoholic steatohepatitis or ASH Non-alcoholic steatohepatitis or NASH

22
ASH vs. NASH No qualitative histologic differences.
When large groups of patients compared: alcoholics tend to develop more severe disease. NASH usually associated with: more: fat nuclear glycogen less: hepatocellular damage inflammation fibrosis Mallory bodies

23
Non-Alcoholic Fatty Liver Disease (NAFLD)
Defined as: Deposition of fat droplets in hepatocytes AND the absence of significant alcohol intake Generally defined as less than ( 140gr ) ethanol per week NAFLD is a range of conditions from near normal liver to cirrhosis
 ethanol per week. NAFLD is a range of conditions from near normal liver to cirrhosis.")
24
Other Terms Simple non-alcoholic fatty liver disease (NAFLD)
Only deposition of fat in liver No inflammation or fibrosis Non-Alcoholic Steatohepatitis (NASH) NAFLD with inflammation (lobular or portal), hepatocyte ballooning, or fibrosis Absence of serologic evidence of infection with hepatitis B or hepatitis C, … Exclude viral hepatitis,autoimmune and metabolic diseases
 NAFLD with inflammation (lobular or portal), hepatocyte ballooning, or fibrosis. Absence of serologic evidence of infection with hepatitis B or hepatitis C, … Exclude viral hepatitis,autoimmune and metabolic diseases.")
25
NAFLD—Spectrum of Disease
Steatosis Steatohepatitis (NASH) NASH with Fibrosis Cirrhosis NAFLD
 NASH with Fibrosis. Cirrhosis. NAFLD.")
26
NAFLD, simple steatosis
Fatty Liver Only deposition of fat in liver No inflammation No fibrosis Not believed to progress to cirrhosis Up to 25 % of some populations!

27
NAFLD—Steatosis

28
Histological section of a murine liver showing severe steatosis
Histological section of a murine liver showing severe steatosis. The clear vacuoles would have contained lipid in the living cells, however the histological fixation caused it to be dissolved and hence only empty spaces remain

29
Deficiency of glucose-6-phosphatase results in accumulation of glycogen in hepatocytes. The liver is enlarged. The hepatocytes are swollen and a mosaic histological pattern with compression of the sinusoids is seen. Macro- and/or microvesicular steatosis can be present

30
Histological features considered necessary for the diagnosis of NASH
Steatosis of varying morphology: Predominantly macro vesicular Mixed lobular inflammation Hepatocellular ballooning generally in zone 3 Other findings: Perisunuzoidal fibrosis Mallory’s bodies,fat cysts,glycogented nuclei Acidophil bodies in kuppfer cells Megamitochondria Lipogranuloma

31
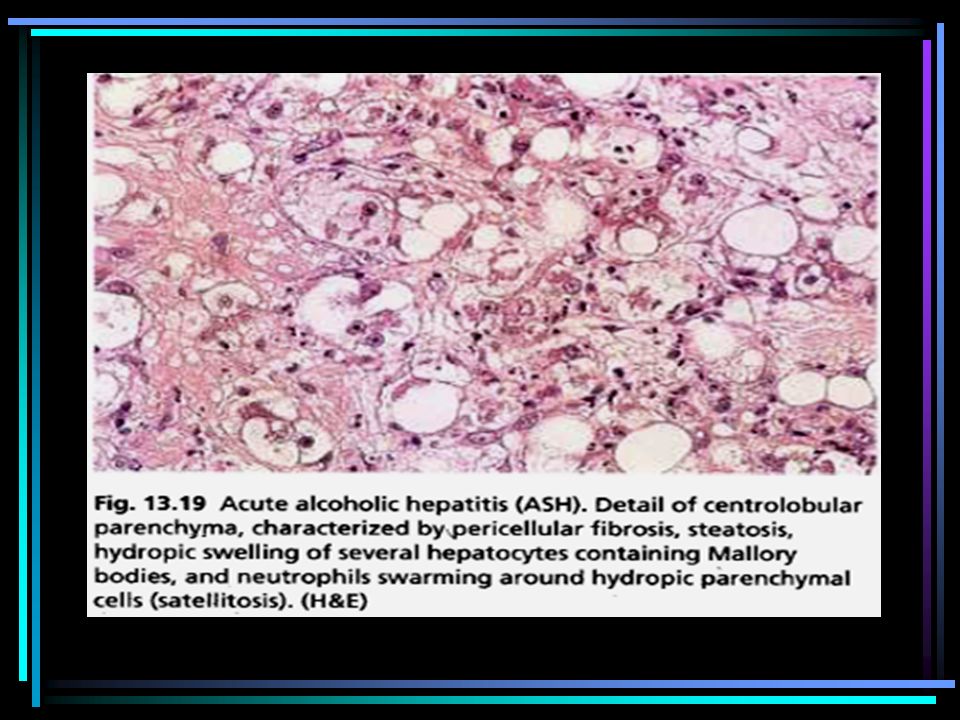
Alcoholic steatohepatitis with neutrophilic acute hepatitis

33
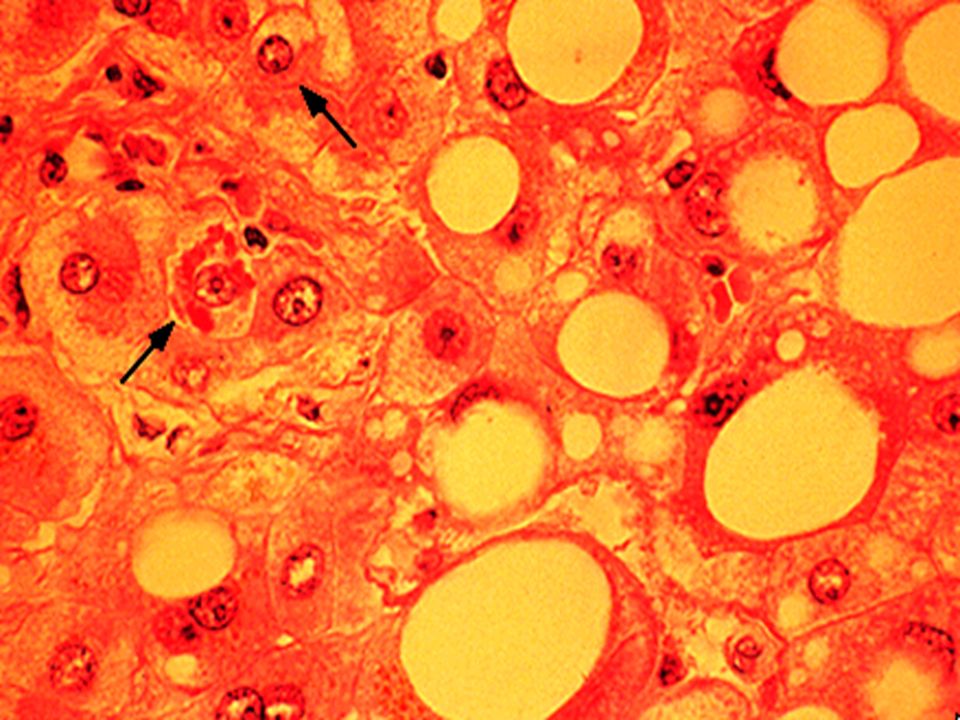
macrovesicular steatosis and ballooning

34
Ballooning degeneration

35
Mallory Body

36
Mallory bodies:homogenous eosinophilic perinuclear
inclusions of variable size and shape. It composed of hyperphosphorylated CK (7, 18, 19) together with Ubiquitin heat shock protein.
 together with. Ubiquitin heat shock protein.")
38
NAFLD—NASH (without fibrosis)
Source: Ibdah 2003

39
glycogen "in" hepatocyte nuclei

40
Steatohepatitis:Some hepatocyte nuclei show glycogen vacuolation

42
Lipogranuloma.

43
Lipogranuloma.

44
periportal hepatic steatosis, as may be seen due to steroid
use. Trichrome stain

45
NAFLD—NASH (with fibrosis)
Source: Ibdah 2003

46
Micrograph of inflamed fatty liver (steatohepatitis)
")
47
Pericellular collagen and Mallory bodies (asterisks) in ballooned hepatocytes are stained blue. Chromotrope Aniline Blue stain.

48
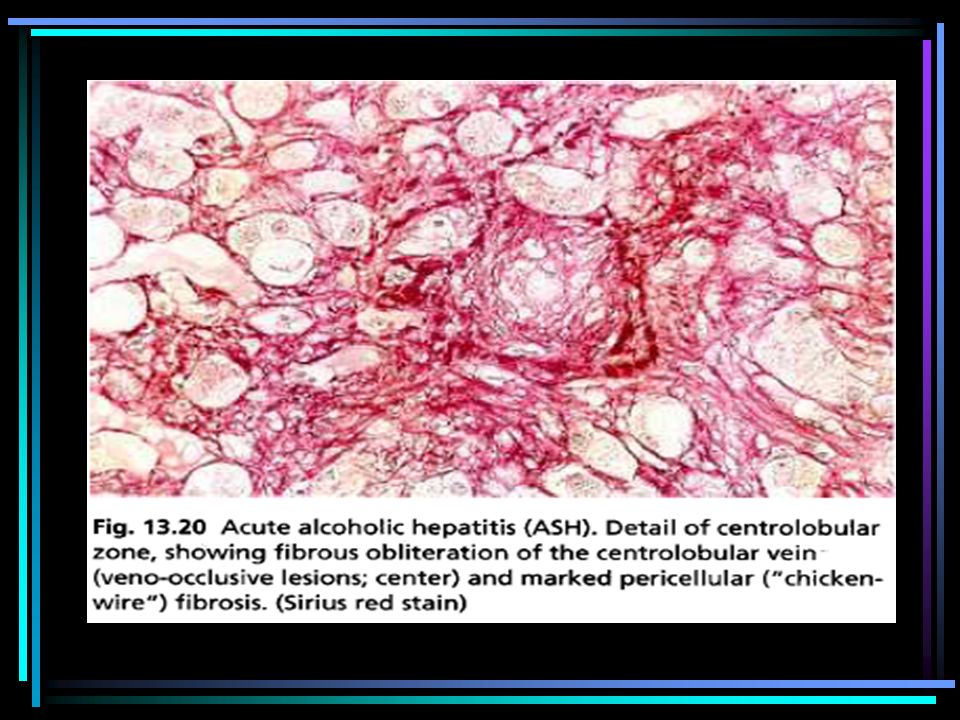
(zone 3) sinusoidal fibrosis, typical of alcoholic
 sinusoidal fibrosis, typical of alcoholic")
50
Steatohepatitis with cirrhosis.

51
Cirrhosis

52
NAFLD—Histological Spectrum
Cirrhosis Time Progression Fibrosis Lobular Inflammation Macrovesicular Steatosis

54
Grading and staging the histopathologic
Lesions of NASH

55
Grade 1(Mild) Steatosis:predominantly macrovesicular,involves ‹33% up to 66% of the lobules Ballooning: occasionally observed in zone 3 Lobular inflammation:scattered and mild acute (PMNs) inflammation and occasional chronic inflammation (mononuclear cells) Portal inflammation:none or mild
 inflammation and occasional chronic inflammation (mononuclear cells) Portal inflammation:none or mild.")
56
Grade 2 (Moderate) Steatosis: any degree and usually mixed macrovesicular, and microvesicular Ballooning: obvious and present in zone 3 Lobular inflammation: PMNs may be noted with ballooned hepatocytes and pericellular fibrosis; mild chronic inflammatory cells may be seen. Portal inflammation: mild to moderate

57
Grade 3 (Severe) Steatosis:>66%(panacinar);commonly mixed type Ballooning: predominantly in zone 3;marked Lobular inflammation: scattered acute and chronic inflammation;PMNs may appear concentrated in zone 3 areas of ballooning and perisinozoidal fibrosis. Portal inflammation: mild to moderate

58
Staging Fibrosis in NASH

59
NASH staging Stage 1:Zone 3 perivenular perisinozoidal/ pericellular fibrosis, focal or extensive Stage 2:As above with focal or extensive periportal fibrosis Stage 3:Bridging fibrosis,focal or extensive Stage 4:Cirrhosis

60
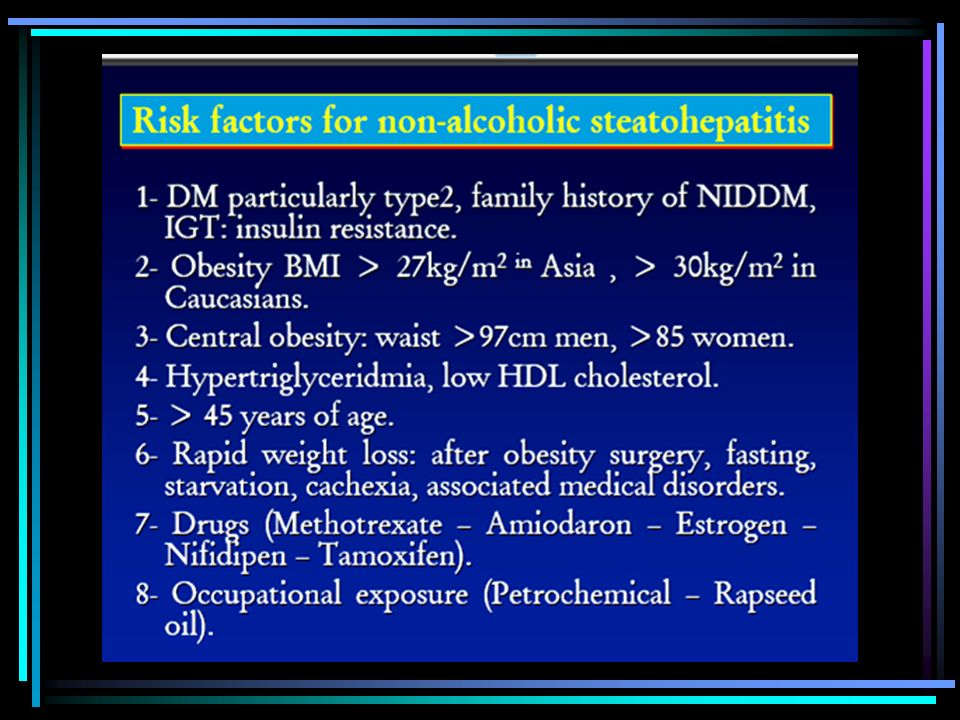
NASH/causes jejunoileal bypass surgery, gastroplasty
rapid and profound weight loss in obese subjects total parenteral nutrition drugs' (amiodarone,perhexiline maleate, estrogens and estrogen receptor ligands, methotrexate) occupational hepatotoxicity disorders characterized by extreme insulin resistance In most cases the etiopathogenesis of NASH appears multifactorial (obesity, type 2 diabetes,and hypertriglyceridemia) the hepatic consequence of the metabolic syndrome or cardiovascular dysmetabolic syndrome or syndrome X
 occupational hepatotoxicity. disorders characterized by extreme insulin resistance. In most cases the etiopathogenesis of NASH appears multifactorial (obesity, type 2 diabetes,and hypertriglyceridemia) the hepatic consequence of the metabolic syndrome or cardiovascular dysmetabolic syndrome or syndrome X.")
61
Risk Factors for NAFLD in Children
Presence of Insulin Resistance Diabetes Consumption of foods high in sugar and calories Soft drinks /cola Fast and junk food High Fructose intake Lack of exercise Time spent on TV/video games

63
(related to obesity and insulin resistance)
Ludwig(et.al) proposed a subclassification to include etiopathogenesis: Primary NASH (related to obesity and insulin resistance) Secondary NASH (post bypass surgery, drugs, and toxins)
 proposed a subclassification to include etiopathogenesis: Primary NASH. (related to obesity and insulin resistance) Secondary NASH. (post bypass surgery, drugs, and toxins)")
64
Pathogenesis

65
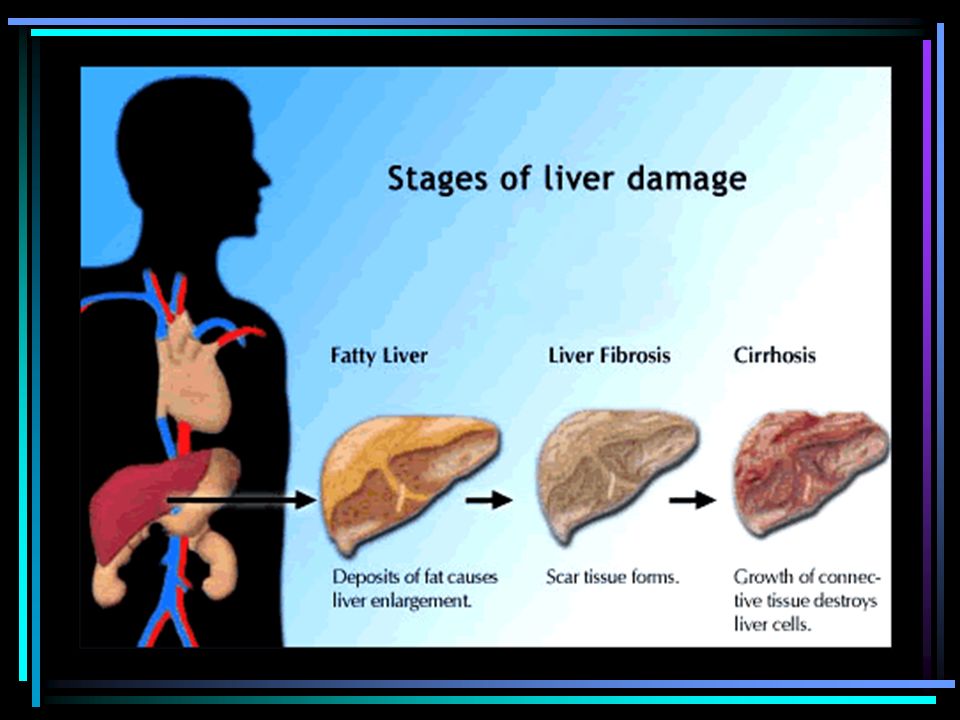
Multiple Hit Theory Normal Liver Fatty Liver Steatohepatitis Cirrhosis
Hit 1: ? Insulin resistance, endotoxins, … Fat accumulation Fatty Liver Hit 2: ? Oxidative stress, … Inflammation Steatohepatitis Hit 3: ? Oxidative stress, … Fibrosis Cirrhosis May loose fat

66
NASH, Diagnosis Most patients are asymptomatic.
Hepatomegaly is the most common physical finding. ALT / AST > 1, usually not so high Ultrasound will demonstrate a fatty or “bright liver.” In CT, the liver is darker than the spleen Liver biopsy is required

67
Summary The prevalence of NASH (2-3%) is comparable to the prevalence of hepatitis B, and much larger than the prevalence of hepatitis C Since hepatitis B is being vaccinated for, we will be seeing less of this disease in the future But obesity is on the rise. (as is hepatitis C) It can be concluded that in the near future, NASH and hepatitis C will be the major liver diseases we will be facing in Iran
 It can be concluded that in the near future, NASH and hepatitis C will be the major liver diseases we will be facing in Iran.")
Similar presentations














 to fatty liver associated with inflammation (steatohepatitis). This condition can occur.>")





, NAFLD, ASH J. Horák Department od Medicine I Department od Medicine I Third Faculty of Medicine Third Faculty of Medicine.>")