Download presentation
Presentation is loading. Please wait.

1
Dr Ian Chandler February 2013
Liver Pathology Made Easy and Understandable II – Patterns of Inflammation Dr Ian Chandler February 2013 With acknowledgements to Prof S Hubscher, Birmingham

2
Patterns of Inflammation in the Liver
Portal inflammation Most chronic liver diseases (e.g. viral, autoimmune) Also seen in acute hepatitis Lobular inflammation Main pattern in acute hepatitis Varying degrees of lobular inflammation also commonly present in chronic viral and autoimmune hepatitis Predominant pattern in some chronic liver diseases (e.g. fatty liver disease) Mixed portal and lobular
 Also seen in acute hepatitis. Lobular inflammation. Main pattern in acute hepatitis. Varying degrees of lobular inflammation also commonly present in chronic viral and autoimmune hepatitis. Predominant pattern in some chronic liver diseases (e.g. fatty liver disease) Mixed portal and lobular.")
3
Zone 3 (perivenular or centrilobular)
Normal Liver Liver Zones Zone 1 (periportal) Zone 2 (mid-zonal) Zone 3 (perivenular or centrilobular)
 Zone 2 (mid-zonal) Zone 3 (perivenular or centrilobular)")
4
Portal Inflammation – Histological Assessment
Aetiology Known (e.g. hepatitis B & C) Assess disease severity inflammation grade – interface hepatitis fibrosis stage Identify co-existent disease (e.g. NAFLD) Aetiology Suspected (e.g. autoimmune hepatitis) Identify features supporting suspected diagnosis (absence of features suggesting an alternative diagnosis) Aetiology Uncertain/Unknown Pattern & composition of inflammatory infiltrate (and other associated features) may provide diagnostic clues
 Assess disease severity. inflammation grade – interface hepatitis. fibrosis stage. Identify co-existent disease (e.g. NAFLD) Aetiology Suspected (e.g. autoimmune hepatitis) Identify features supporting suspected diagnosis. (absence of features suggesting an alternative diagnosis) Aetiology Uncertain/Unknown. Pattern & composition of inflammatory infiltrate (and other associated features) may provide diagnostic clues.")
5
Composition of Inflammatory Cells in Portal Tracts
In most conditions, most lymphocytes in portal tracts are T cells B cell rich lymphoid aggregates will be found in HCV infection and also other conditions such as PBC and AIH Plasma cells are characteristic of AIH, and also PBC/PSC. They are less common in HCV and NASH

6
Hepatitis C 2 cases, different severity

7
Autoimmune Hepatitis

8
Composition of Inflammatory Cells in Portal Tracts
Granulomas are common in sarcoid and PBC, but can be found in PSC, HCV and drug reactions Portal tract neutrophils are mostly associated with a ductular reaction, in acute biliary obstruction, chronic biliary disease, and also acute hepatitis Eosinophils: drug reaction, biliary obstruction, PBC & PSC, parasitic infestation, acute allograft rejection

9
Granuloma in HCV

10
Eosinophils in acute rejection
Eos, biliary damage, endotheliitis

11
Interface Hepatitis (“piecemeal necrosis”)
Inflammation at the interface between connective tissue (portal tract, fibrous septa) and the liver parenchyma Severity classified according to : extent around individual portal tracts/septa (focal vs diffuse) proportion of portal tracts involved (e.g.<50% vs > 50%) Autoimmune Hepatitis Chronic hepatitis with severe activity Hepatitis C Chronic hepatitis with mild activity
 and the liver parenchyma. Severity classified according to : extent around individual portal tracts/septa (focal vs diffuse) proportion of portal tracts involved (e.g.<50% vs > 50%) Autoimmune Hepatitis Chronic hepatitis with severe activity. Hepatitis C Chronic hepatitis with mild activity.")
12
Interface hepatitis in AIH

13
Interface Hepatitis (“piecemeal necrosis”)
Periportal hepatocyte ballooning (Autoimmune Hepatitis) Periportal fibrosis (HVG) Severity of interface hepatitis: Predicts subsequent development of fibrosis/cirrhosis (HCV, AIH, PBC) Guides therapeutic decisions (AIH, ?PBC/PSC – “overlap syndromes”)
 Periportal fibrosis (HVG) Severity of interface hepatitis: Predicts subsequent development of fibrosis/cirrhosis (HCV, AIH, PBC) Guides therapeutic decisions (AIH, PBC/PSC – overlap syndromes )")
14
PBC & PSC – Changing Role of Liver Biopsy EASL Clinical Practice Guidelines – J Hepatol 2009; 51: AASLD Practice Guidelines – Lindor. Hepatology 2009; 50: Establishing a diagnosis Liver biopsy no longer required in cases with other typical features Still important in the diagnosis of atypical cases e.g. AMA-negative PBC, small duct PSC-, IgG4-associated SC Diagnostic duct lesions only present in liver biopsies from: 30-50% of PBC cases (Wiesner 1985, Drebber 2008) 12% of PSC cases (Wiesner 1985)
 12% of PSC cases (Wiesner 1985)")
15
PBC 2 cases, more and less obvious

16
Primary Biliary Cirrhosis Significance of Inflammatory Activity
Severity of inflammatory activity (periportal and lobular) Predictive for subsequent progession to fibrosis /cirrhosis & liver failure Moderate or severe interface hepatitis also used as a diagnostic criterion for PBC/AIH “overlap syndrome” (PBC with “hepatitic features”) % of PBC have additional features supporting a diagnosis of AIH (biochemical, immunological and histological) PBC with “hepatitic features” - worse outcome than “pure” PBC May benefit from treatment with immunosuppression Normalisation of ALT levels Less severe fibrosis progression Similar comments apply to PSC
 Predictive for subsequent progession to fibrosis /cirrhosis & liver failure. Moderate or severe interface hepatitis also used as a diagnostic criterion for PBC/AIH overlap syndrome (PBC with hepatitic features ) 10-15% of PBC have additional features supporting a diagnosis of AIH (biochemical, immunological and histological) PBC with hepatitic features - worse outcome than pure PBC. May benefit from treatment with immunosuppression. Normalisation of ALT levels. Less severe fibrosis progression. Similar comments apply to PSC.")
17
Referred Biopsy – Diagnosis Chronic Hepatitis ? Cause
Raised Alk Phos. Autoantibody screen negative. Portal inflammation and interface hepatitis Biliary features not conspicuous Orcein - Periportal copper-associated protein Keratin 7 Immunostaining “intermediate hepatobiliary cells” Repeat autoantibody testing = AMA-positive

18
Role of Liver Biopsy in Acute Hepatitis
Many of the classical morphological studies of acute hepatitis were carried out before the main causes had been discovered Most cases of acute hepatitis now diagnosed on the basis of clinical, biochemical and serological findings and liver biopsy is rarely indicated Liver biopsy may still be carried out in cases where the clinical presentation is atypical or the cause is uncertain Distinguish severe acute hepatitis from decompensated chronic liver disease Determine disease severity Identify possible aetiological factors (including cases of acute liver injury not related to hepatitis)
")
19
Changes tend to be most marked in perivenular regions (zone 3)
Acute (and chronic) Hepatitis Histological Findings in Liver Parenchyma Inflammatory Infiltration mainly lymphocytes ( T cells >> B cells) plasma cells (esp in AIH) neutrophils (esp in alcoholic hepatitis) - eosinophils (esp in drug reactions) Hepatocellular Damage ballooning bile pigment accumulation (bilirubinostasis) - lobular disarray cell death (apoptosis and/or necrosis) Changes tend to be most marked in perivenular regions (zone 3)
 Hepatitis Histological Findings in Liver Parenchyma. Inflammatory Infiltration - mainly lymphocytes ( T cells >> B cells) - plasma cells (esp in AIH) - neutrophils (esp in alcoholic hepatitis) - eosinophils (esp in drug reactions) Hepatocellular Damage - ballooning - bile pigment accumulation (bilirubinostasis) - lobular disarray - cell death (apoptosis and/or necrosis) Changes tend to be most marked in perivenular regions (zone 3)")
20
Liver Cell Death in Lobular Hepatitis (acute or chronic)
Pattern of Cell Death Histological Features Spotty necrosis Apoptosis of individual hepatocytes (acidophil bodies) Confluent necrosis (zone 3) Loss of groups of adjacent liver cells Bridging necrosis Confluent necrosis linking vascular structures (central-central or central-portal bridging) Panacinar necrosis Loss of hepatocytes in an entire acinus Multiacinar necrosis Panacinar necrosis involving several adjacent acini Apoptosis > necrosis (in mild forms)
 Confluent necrosis. (zone 3) Loss of groups of adjacent liver cells. Bridging necrosis. Confluent necrosis linking vascular structures. (central-central or central-portal bridging) Panacinar necrosis. Loss of hepatocytes in an entire acinus. Multiacinar necrosis. Panacinar necrosis involving several adjacent acini. Apoptosis > necrosis (in mild forms)")
21
Acidophil body AIH

22
Multiacinar Necrosis Normal vascular relationhips Prominent ductular reaction (resembling biliary obstruction)
 .")
23
Could this be cirrhotic?

24
Recent Post-Necrotic Collapse versus Longstanding Fibrosis - Use Of Connective Tissue Stains
Material Demonstrated Distribution In Normal Liver Changes In Liver Disease Reticulin Type III collagen fibres Portal tracts, hepatic sinusoids Collapse of reticulin framework in areas of recent liver cell necrosis. (few days) Haematoxylin Van Gieson Type I collagen fibres Portal tracts, walls of hepatic veins Increased in hepatic fibrosis (weeks/months) Orcein Elastic fibres Portal tracts, walls of hepatic veins Found in long-standing fibrosis/cirrhosis (months/years)
 Haematoxylin. Van Gieson. Type I collagen fibres. Portal tracts, walls of hepatic veins. Increased in hepatic fibrosis. (weeks/months) Orcein. Elastic fibres. Portal tracts, walls of hepatic veins. Found in long-standing fibrosis/cirrhosis. (months/years)")
28
Acute Hepatitis - Common Causes
Viral Hepatitis viruses – A,B,C,D, E Other viruses – e.g. CMV, EBV Drugs Autoimmune Unknown Seronegative hepatitis (“non-A, non-B, non-C hepatitis”)
")
29
Acute Hepatitis - Aetiological Considerations
Liver biopsy rarely identifies a previously unsuspected aetiology Biopsies mostly obtained from people in whom main recognised causes have been excluded (“seronegative hepatitis”) Biopsy sometimes provides pointers to a previously unsuspected aetiology Aetiology Suggestive Histological features Drugs Disproportionately severe necrosis/unusually prominent cholestasis (relatively little inflammation – lobular and/or portal) Eosinophils Granulomas Autoimmune hepatitis Plasma cell rich infiltrate (also seen in hepatitis A) Prominent periportal inflammation (interface hepatitis) Prominent centrilobular inflammation (“central perivenulitis”) Lymphoid aggregates
 Biopsy sometimes provides pointers to a previously unsuspected aetiology. Aetiology. Suggestive Histological features. Drugs. Disproportionately severe necrosis/unusually prominent cholestasis. (relatively little inflammation – lobular and/or portal) Eosinophils. Granulomas. Autoimmune hepatitis. Plasma cell rich infiltrate (also seen in hepatitis A) Prominent periportal inflammation (interface hepatitis) Prominent centrilobular inflammation ( central perivenulitis ) Lymphoid aggregates.")
30
Role of Liver Biopsy in Fatty Liver Disease
Establishing a morphological diagnosis Distinction between steatosis and steatohepatitis Recognition of portal tract changes Aetiological pointers AFLD versus NAFLD cases with a dual pathology (e.g. HCV and NAFLD) Biopsy may help to identify the main cause of liver injury Assessing disease severity grading of fat, ballooning, inflammation staging of fibrosis
 Biopsy may help to identify the main cause of liver injury. Assessing disease severity. grading of fat, ballooning, inflammation. staging of fibrosis.")
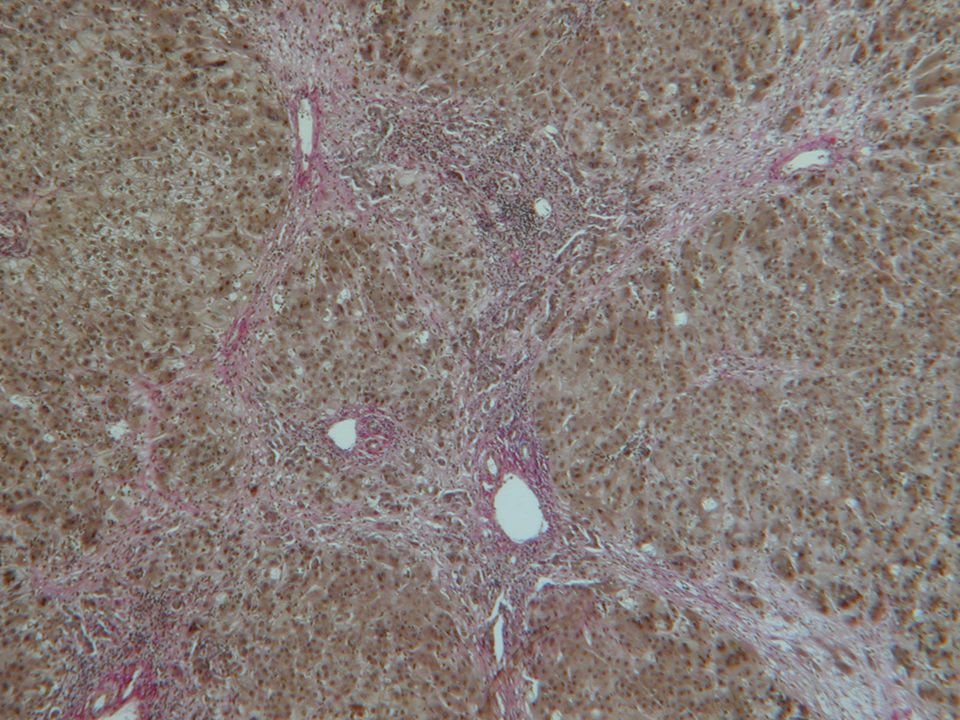
31
Alcoholic steatohepatitis with cirrhosis
DOG IN KENNELS in capitals in the letter!!

32
HCV with fat ?cause Fat ? ASH/NASH/HCV/methotrex from psoriasis

33
Phnom Penh

Similar presentations




 inflammatory lesions 3.Changes in late post-transplant biopsies Banff 2001 ->")



>")











 Chapters: The Liver and the Biliary Tract The Pancreas.>")
/Hx of icter(-)>")