Download presentation
Presentation is loading. Please wait.

1
Maternal Child Health Nursing Module 1

2
Objectives – Day 1 Discuss the female reproductive system anatomy/physiology, disorders, medical treatment, nursing care.

3
Female Anatomy and Physiology
Female reproductive system Ovaries-produce estrogen and progesterone – and eggs or ova Fallopian tubes, sometimes called oviducts or uterine tubes - where fertilization takes place Uterus-3 layers (endo-, myo-, peri- metrium) fundus, corpus, cervix Vagina
 fundus, corpus, cervix. Vagina.")
5
Greater vestibular glands (Bartholin's) Vulva and perineum
Accessory Organs In females Oviducts Uterus Vagina Greater vestibular glands (Bartholin's) Vulva and perineum
 Vulva and perineum.")
6
Female reproductive system. The enlargement (right) shows ovulation.
 shows ovulation.")
7
Female Anatomy and Physiology
External genitalia-mons pubis, labia majora/minora, clitoris, and vestibule (a recess which contains the opening to the urethra) Accessory glands Skene’s glands-similar to prostate gland Bartholin’s glands-provide lubrication Perineum Mammary glands (breasts)
 Accessory glands. Skene’s glands-similar to prostate gland. Bartholin’s glands-provide lubrication. Perineum. Mammary glands (breasts)")
9
Female: superior inlet

10
Female: inferior outlet

13
Located in pelvic abdomen Held by ligaments
The Ovaries Located in pelvic abdomen Held by ligaments Attached to uterus and body wall Contain and release eggs during ovulation

15
Ovarian follicle (Graafian follicle) Holds ripening ova
The Ova and Ovulation Ovarian follicle (Graafian follicle) Holds ripening ova Secretes estrogen Ruptures to discharge egg cell (ovulation) Oviduct (aka Fallopian Tube) Tube that leads to uterus
 Holds ripening ova. Secretes estrogen. Ruptures to discharge egg cell (ovulation) Oviduct (aka Fallopian Tube) Tube that leads to uterus.")
16
The Corpus Luteum Formed from remains of follicle after ovum is expelled Secretes estrogen and progesterone Usually shrinks and is replaced by scar tissue unless pregnancy initiated Remains active during early pregnancy

17
The Oviducts: Fallopian Tubes
Extend from near ovary to uterus Not directly connected to ovary Fimbriae produce current that sweeps ova into oviduct Cilia in tube lining and peristalsis of tube move ova

18
The Uterus Organ where fetus develops to maturity Myometrium
Muscular wall Endometrium Specialized epithelium lining Corpus Body Cervix Neck Fundus Supporting ligaments

19
The Cervix

20
The Vagina Distal part of birth canal that opens to outside of body Fornix Posterior fornix Cul-de-sac (rectouterine pouch or pouch of Douglas) Hymen Greater vestibular (Bartholin's) glands
 glands.")
21
Female reproductive system (sagittal section)
Female reproductive system (sagittal section). This view shows the relationship of the reproductive organs to each other and to other structures in the pelvic cavity.
. This view shows the relationship of the reproductive organs to each other and to other structures in the pelvic cavity.")
22
The Vulva and the Perineum
Vulva: external parts of female reproductive system - Labia - Clitoris - Related structures - Obstetrical perineum

23
The Menstrual Cycle Controlled by pituitary hormones regulated by hypothalamus Cyclic pattern Regulated by hormonal feedback Averages 28 days

24
Several follicles in ovary begin to develop
Beginning of the Cycle Several follicles in ovary begin to develop Increased production of estrogen Thickens endometrium Elongates uterine secretion glands Inhibits release of FSH Stimulates pituitary to release LH

25
Luteinizing Hormone (LH) surge in blood Causes ovulation
Transforms ruptured follicle into corpus luteum that produces estrogen and progesterone Endometrium thickens Glands and blood vessels increase in size Follicle Stimulating Hormone (FSH) and LH are inhibited
 and LH are inhibited.")
26
If ovum is not fertilized, corpus luteum degenerates
The Menstrual Phase If ovum is not fertilized, corpus luteum degenerates Estrogen, progesterone levels decrease Endometrium degenerates, produces menstrual flow Endometrium begins to repair itself FSH released from anterior pituitary

28
Normal ovarian function declines Follicles stop ripening
Menopause Menstruation ceases Normal ovarian function declines Follicles stop ripening No appreciable amounts of estrogen produced Uterus, oviducts, vagina, vulva become somewhat atrophied Vaginal mucosa becomes thinner, dryer, more sensitive

29
Increases breast cancer risk Increases thrombosis and embolism risk
Hormone Replacement Therapy Combination of estrogen with synthetic progesterone prescribed to relieve menopause discomfort Increases breast cancer risk Increases thrombosis and embolism risk Risks increase with duration of therapy

30
Common Diagnostic Tests
Laboratory Tests Radiologic Tests Surgical Tests Other Tests

31
Reproductive Lab Tests
Triple or Quad screen Cultures HCG Pap Smear Serum Alkaline Phosphatase Serum Calcium Segmented Bacteriologic Localization Culture

32
More lab tests Rubella immunity HIV antibody
Tests for sexually transmitted diseases Hepatitis B screen Varicella zoster viral screen TORCH panel Group B strep

33
Lab tests (cont’d) Glucose challenge test
Platelet count, H&H, Rh antibody screen Fetal fibronectin (fFN) Lecithin-sphingomyelin ratio Triple and Quad screens
 Lecithin-sphingomyelin ratio. Triple and Quad screens.")
34
Cultures Cultures and ‘smears’ are collected from exudates of the breast, vagina, rectum and urethra They can be used to examine and identify: Infectious processes Presence of abnormal cells Hormonal changes Spread the collected specimen on a slide with aseptic technique

35
Clean catch urine Frequently used to measure protein, glucose, WBCs and other elements in urine Have patient clean area around urethral opening with antiseptic wipe Have patient void some urine, stop stream and void urine into specimen cup and then finish urinating Nurse uses standard precautions

36
Human Chorionic Gonadotropin (HCG) in other contexts
Confirms pregnancy, threatened or incomplete abortion Produced by embryo to prompt corpus luteum to increase estrogen and progesterone Assists in the diagnostic of HCG – producing tumors, such as choriocarcinoma or hydatidiform moles

37
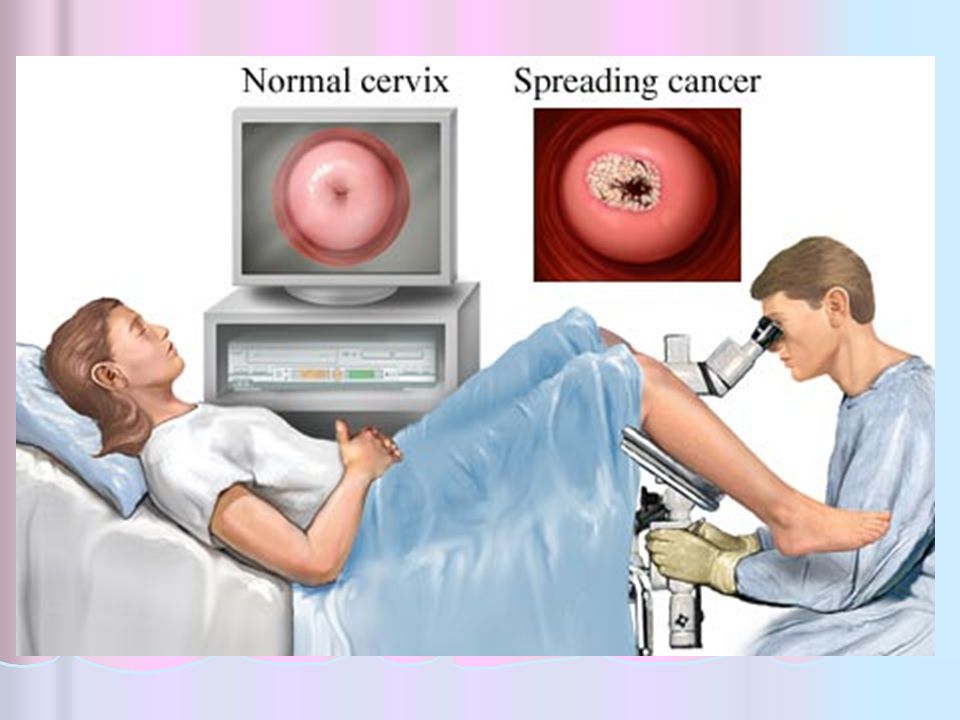
Papanicolaou (Pap) Test (Smear)
Used to screen for early detection of cervical cancer and/or infections (such as HPV) Examines scrapings of secretions and cells taken from the cervix Label slides with date and time of collection, LMP, and whether the woman is taking estrogens or BCP Women should have yearly Pap smears beginning at age 21 or three years after first sexual intercourse every 2-3 years. More frequent exams may be required for high risk factors.
 Examines scrapings of secretions and cells taken from the cervix. Label slides with date and time of collection, LMP, and whether the woman is taking estrogens or BCP. Women should have yearly Pap smears beginning at age 21 or three years after first sexual intercourse every 2-3 years. More frequent exams may be required for high risk factors.")
38
Radiology: Hysterosalpingogram
Study for visualizing the uterine cavity to confirm: Tubal abnormalities (adhesions and occlusions) The presence of foreign bodies Congenital malformation and leiomyomas (fibroids) Traumatic injuries
 The presence of foreign bodies. Congenital malformation and leiomyomas (fibroids) Traumatic injuries.")
39
Hysterosalpingogram Lithotomy position
Insertion of speculum into the vagina Cannula inserted through the speculum into cervical cavity Contrast medium injected through the cannula Uterus and oviducts then viewed by a fluoroscope and films taken

41
Radiology: Mammography
soft tissue of the breast identification of various benign and neoplastic processes, especially those not palpable on exam Mammograms should be performed yearly after age 40 (American Cancer Society). High-risk women should also get an annual breast MRI
. High-risk women should also get an annual breast MRI.")
42
Surgery: Breast Biopsy
Used to differentiate benign or malignant tumors Needle biopsy ~ local anesthetic, biopsy taken from the breast. Pressure applied to site to stop bleeding. Open biopsy ~ general or local anesthetic, incision into breast to expose suspicious tissue and then specimens obtained. Sutures and dressing applied to incision.

43
Surgery: D & C Dilation and Curettage – scraping of material from the wall of a cavity or other surface; performed to remove tumors or other abnormal tissue for microscopic study General anesthesia, the cervix is dilated, and the walls of the uterus scraped with a curette

44
Used for dilation of cervix
Modern speculum Used for dilation of cervix

45
Surgery: Endometrial biopsy
Tissue collection: diagnosis of endometrial cancer and analysis for infertility studies. Performed at time of menstruation, as cervix is partially dilated and cells are more easily obtained Cervix is locally anesthetized, a curette (loop) is inserted and tissue is obtained
 is inserted and tissue is obtained.")
46
Surgery: Laparoscopy Visualizes abdominal cavity
Uterus, adnexa small incision beneath the umbilicus Foley Catheter inserted to keep bladder decompressed General anesthesia C02 to inflate abdomen Gas, referred pain to shoulder

47
Nursing care: surgery Ensure urinary elimination
Foley catheter may be needed until patient able to void Discharge instructions should include safety No lifting more than 10 lbs until cleared by physician Teach s/s infection, how to clear any drains and monitor dressings and sites

49
Colposcopy Mounted, lighted instrument exams cervix, vagina
Indications: Follow-up of abnormal Pap abnormal bleeding or pain during intercourse sores on the vulva

51
Pelvic Exam Exam of the: Often done with a Pap test
vulva, vagina, uterus, rectum and pelvis, including the ovaries masses or growths. Often done with a Pap test Insertion of one or two gloved fingers into the vagina, hand pressure to lower abdomen slight discomfort or pressure normal

53
Patient Education for Pelvic Exam
No douching for at least 2-3 days prior No sex for 24 hours prior to the exam Try to schedule when not on period Need empty bladder Gown only, provide drape for modesty Lithotomy position

55
Ultrasound Transducer: high-pitched sound waves
Moved over abdomen with aid of gel Scan of fetus and uterine or abdominal structures form picture (sonogram) on monitor screen Predictive for normal pregnancy or abnormalities Nursing: educate about procedure and purpose, avoid making patient anxious
 on monitor screen. Predictive for normal pregnancy or abnormalities. Nursing: educate about procedure and purpose, avoid making patient anxious.")
57
Vaginal ultrasound Vaginal ultrasound:
Transducer placed in vagina Clearer imaging Useful for obese patients to reduce amount of tissue between transducer and tissues to be scanned Also useful early in pregnancy if clear resolution of young fetus necessary Nursing care: explain procedure and expected result, provide modesty and comfort

58
Inflammatory: Mastitis
Breast infection S. aureus or streptococci Late pregnancy or lactation Cracked nipple, infant infection Obstructs milk flow Tender, inflamed, engorged breast Important to express milk or decrease production – keep breastfeeding Nursing care: anti-infective, comfort measures, reassurance and education

59
Pelvic inflammatory disease (PID)
pathogenic invasion of the fallopian tubes and/or ovaries, as well as any vascular or supporting structures within the pelvis, except the uterus Gonorrhea; streptococcus; staphylococcus; Chlamydia; tubercle bacilli May cause adhesions or sterility Fever and chills, severe abdominal pain, malaise, nausea, vomiting, purulent exudate Nursing care: infection control, education

60
Inflammatory: Endometriosis
growth of endometrial tissue within pelvic cavity ovarian hormones during menses cause bleeding and inflammation adhesions, organ fusion, bladder dysfunction, or sterility

61
Inflammatory: Vaginitis
Simple: E. coli, staphylococcal, streptococcal, T. vaginalis, C. albicans, Gardnerella Vaginal discharge, itching, burning Obtain accurate history Nursing care focus: rebalance acid/base, treat sexual partners, control/prevent infection

62
Inflammatory: cervicitis
Common reproductive disease Caused by vaginal infection or STD May follow lacerations from childbirth or abortion S/S: backache, whitish exudate, menstrual irregularities TX: anti-infective

63
Inflammatory: Toxic shock syndrome
S. aureus Usually seen after superabsorbent tampon use Overgrowth of bacteria releases toxins Fever, vomiting, diarrhea, myalgia, hypotension, s/s septic shock, sore throat, H/A, red rash and desquamation, oliguria, elevated BUN

64
Nursing care: genital tract infection/inflammation
Assessment: s/s infection Response to treatment Education Cause Prevention/control How to use treatment

65
Benign neoplasms Fibrocystic breast: Cysts in mammary ducts
Increases risk for breast cancer Often bilateral, multiple, soft, tender, moveable Related to ovarian activity Mammography, biopsy Diet change, Danazol, vit. E

66
Benign neoplasms Ovarian cysts:
May arise from dermoid cells in uterus, cystic corpus luteum or Graafian follicle May disturb menstrual cycle or cause slight vaginal bleeding, feeling “heavy” Ovarian cystectomy May be present in Polycystic Ovarian Syndrome (PCOS)
")
67
Breast cancers Breast cancer Unknown cause, hormonal influence
Small, solitary, irregular-shaped, firm, non-tender, and non-mobile tumor Change in skin color, puckering or dimpling of tissue, nipple discharge, retraction of nipple, axillary tenderness Radiation, chemotherapy and/or surgery most common treatments

68
Breast cancers Risk factors: genetics, more than 2 alcoholic drinks/day, late or no childbirth, estrogen exposure, radiation during breast development Nursing care: teach breast self exam, educate and support, assess acceptance and understanding of surgery/treatments Lumpectomy Mastectomy Partial Simple Modified radical

69
Breast cancers Breast self-exam
Done 7-8 days after the last day of the menstrual cycle Examine visually in mirror Palpate in routine and systematic way, using circular motion Include the axillae Compress nipple and areola to check for discharge Report changes to provider

70
Breast cancers Nursing care:
emotional and physical support of treatment side effects pre/post operative care Arm exercises after mastectomy to relieve edema assessment of psychosocial adjustment to physical changes and illness

71
Cervical cancer Usually squamous cell carcinoma
Pap smears help detect preinvasive lesions; early stages “silent” Linked to sexual risk factors, smoking, DES use in mom, multiple births, HPV Leukorrhea, irregular vaginal bleeding, spotting, changes in vaginal exudate with disease progression Surgical removal of area

72
Ovarian cancer Fourth most common cause of cancer death in women
High risk: infertile; anovulatory; nulliparous; habitual aborters; high-fat diet; exposure to industrial chemicals, close genetic relationship > 5 years’ oral contraceptive use may decrease risk Early S/S: Vague abdominal discomfort, flatulence; mild gastric disturbance

73
Nursing care: reproductive CA
Assessment: pain, function, psychosocial state, bleeding, V/S, pre/post operative status Nursing care: pain management, referral, control bleeding, monitor vital signs and physical status, prepare for surgery and monitor post-operatively, report changes in baseline status

74
Normal menses - review Sign of puberty
Body becomes capable of supporting a pregnancy Occurs from 9-17 years of age; average is 12 ½ Cycle varies from days; average 28 Flow lasts from 1-8 days; average 3-5 Flow amount mL; average 35 mL

75
Normal menses- review Menopause Normal decline in female fertility
Average age 51 Atrophy of the vulva, vaginal dryness, loss of skin turgor and elasticity, shrinkage of reproductive structures Fertility may remain as long as there is ovulation of any pattern

76
Menstrual disorders Dysmenorrhea Amenorrhea Polymenorrhea
Oligomenorrhea Menorrhagia Metrorrhagia

77
Menstrual disorders (cont’d)
abnormal uterine bleeding premenstrual syndrome

78
dysmenorrhea Pain during menses that interrupts daily life activities
Primary: not related to disease, usually starts when ovulation established (<20 years old), often declines/disappears with pregnancy or by late 20s Secondary: r/t disease (PID, endometriosis, etc), usually >20 years old
, often declines/disappears with pregnancy or by late 20s. Secondary: r/t disease (PID, endometriosis, etc), usually >20 years old.")
79
dysmenorrhea Endocrine imbalance, increased prostaglandins, or chronic illness, fatigue and anemia Diagnostics: pelvic exam, laparoscopy, D&C, hysterosalpingography Nursing care depends upon causative factors: post-operative or procedural; supportive nutrition and symptom suppression

80
amenorrhea Primary: delayed onset of menses by 17 or 18
Causes – congenital defect Secondary - menarche occurred but has ceased Causes – pregnancy, frequent, vigorous exercise, or emotional disorders, anorexia

81
amenorrhea No menstrual flow for at least three months
number of periods missed and drugs/medications Diagnostic: Pelvic exam, blood, urine, and hormone analysis, assessment of presence of tumors, Pap test

82
Menorrhagia A form of abnormal menstrual bleeding
Excessive menstrual flow Younger women: endocrine disturbance Older women: inflammation or tumors Pad or tampon count

83
Premenstrual syndrome
30%-50% women ages 25-45 Unrelated to ovulation Probably r/t neuroendocrine events in anterior pituitary gland Possibly caused by estrogen/progesterone imbalances, B6 or magnesium deficiency 7-10 days before menses Diagnosed after other disorders ruled out

84
Premenstrual syndrome
Treatment: symptom suppression; physical, emotional, nutrition support. May include medicines (anxiolytics, antidepressants), alternative therapies, exercise, B6/calcium/magnesium supplements, avoidance of triggers (caffeine, alcohol, nicotine), self-care and stress minimization
, alternative therapies, exercise, B6/calcium/magnesium supplements, avoidance of triggers (caffeine, alcohol, nicotine), self-care and stress minimization.")
85
Structural disorders Fistulas Cystocele Urethrocele Rectocle
Prolapsed uterus Relaxed pelvic muscles

86
Vaginal fistulas Abnormal opening between vagina and
Urethra Bladder rectum Results from cancer, radiation, weakened tissues from pregnancy, surgery, necrosis in drastically prolonged labor

87
Cystocele Displacement of the bladder into the vagina r/t childbearing, multiple births, cervical tears Urinary urgency, frequency, and incontinence; fatigue; pelvic pressure Treatment: bladder suspension Nursing care: teaching, care r/t urinary flow, post-surgical care

88
Prolapsed uterus Prolapse of the uterus through the pelvic floor and vaginal opening Rated as first, second, or third degree Stress incontinence, bowel/bladder problems, protrusion of cervix/vaginal walls into perineum

89
Prolapsed uterus

90
Nursing care: structural disorder
Assess for pain, bleeding, vital signs, urine or feces retention, elimination pattern, H&P, protrusion of tissues Comfort, tissue protection, control bleeding, monitor vital signs, pre/post operative care, monitor I&O, report changes from normal baseline

91
Infertility The inability to conceive after 1 year of sexual intercourse without birth control Primary: no history of conception Secondary: inability to conceive after hx conception Factors: age, impaired sperm/ova production, interruption in reproductive system preventing fertilization

92
Infertility: factors Men: most fertile in teens and early 20s
Women: most fertile ages 20-29, decreases ages and ends with menopause Female infertility most often due to history of infections or inflammatory disorders of reproductive system

93
Infertility: testing Male infertility in 40% cases and testing simpler, so man may be tested first Semen analysis Endocrine imbalance Underlying systemic issues Women’s testing: Ovulation function of reproductive organs

94
Infertility: treatment
Hormone therapy to induce/support ovulation (Clomid, Pergonal, Parlodel) Surgery for blocked structures Support of cervical mucus quality by treating inflammation (cauterization) or giving estrogens Reducing physical, psychological stressors to support efforts
 Surgery for blocked structures. Support of cervical mucus quality by treating inflammation (cauterization) or giving estrogens. Reducing physical, psychological stressors to support efforts.")
95
Infertility: treatment
Intrauterine insemination with partner or donor sperm In-vitro fertilization Artificial Reproductive Therapies

Similar presentations














- Organs mature, pubic and armpit hair, regulates release of.>")









 to most offensive (5) Explain why you chose your number.>")





