Download presentation
Presentation is loading. Please wait.

1
Case Study : Hepato – Pancreatico Biliary Dr.J.A.Venter Dept.Imaging Sciences,Bloemfontein Academic Hospitals 13/04/2012

2
Me.N.B.Mes 20 year old female refered to UH from Kby Hospital post abdominal mass biopsy for further management. Prior history : Healthy until blunt abdominal trauma in 2010 through a kick in the epigastrium during a football game followed by episode of severe abdominal pain and vommitting for which she was hospitalized for 3 days after which it subsided. 2 nd similar episode with associated weight loss in 2011 not preceeded by trauma led to referral to the Kby hospital where a CT study of the abdomen and subsequent biopsy of a abdominal mass where performed on 24/12/2011.

3
Clinical/Special Examination Vitals normal,No JACCOL Distended abdomen due a large palpable epigastric mass extending into left and right hypochonrium. FBC,U+E,LFT normal. S- amylase never elevated No documented episodes of PUD, hypoglycemia or watery diarrhea

4
Surgical Findings : 08/02/2012 Large combined cystic and solid pancreatic tumor with associated multiple peritoneal and omental nodules which were debulked including a splenectomy and tranvers colon resection due to vascular compromise.

5
Differential diagnosis of cystic pancreatic neoplasms: Non Neoplastic - Pseudocyst/Infective SCN MCN Intraductal Neoplasms (IPMN) Epithelial Neoplasms of uncertain direction of differentiation -SPEN Cystic Pancreatic Endocrine Tumor(PET) Cystic Metastases Ductal Adenocarcinoma with cystic change Cystic Teratoma Lymphoepithelial cyst
 Epithelial Neoplasms of uncertain direction of differentiation -SPEN Cystic Pancreatic Endocrine Tumor(PET) Cystic Metastases Ductal Adenocarcinoma with cystic change Cystic Teratoma Lymphoepithelial cyst")
6
Cyst Morphology

7
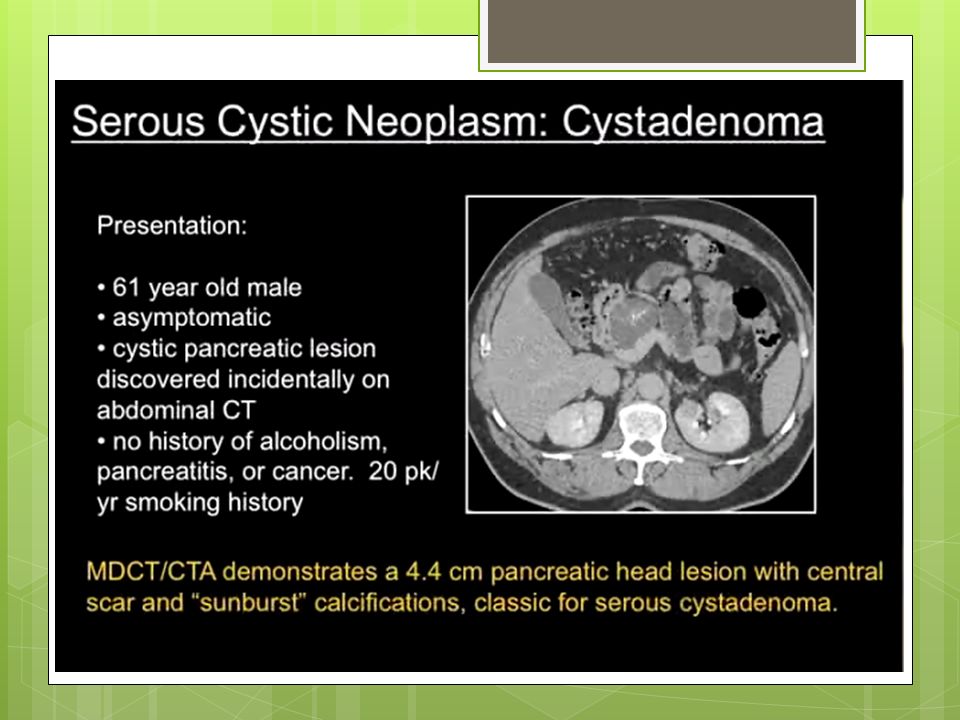
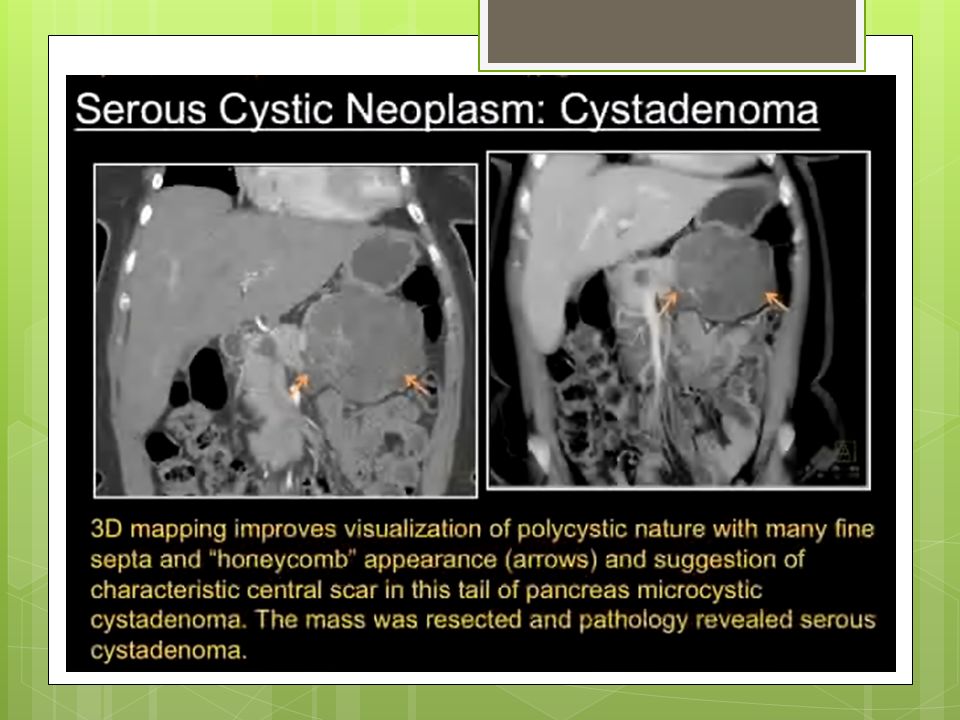
Serous Cystic Neoplasm(SCN) Women > 60 years – “ grandmother lesion” Slight predominance of occurrence in pancreatic head. Coarsely calcified central scar with a sunburst pattern. Can appear solid on CT – MRI most sensitive to detect fluid. Consist of multiple(>6) small cysts < 2 cm in diameter. Olygocystic variant 2 cm difficult to distinguish from MCN. Cyst fluid CEA < 192 ng/ml, Contain no mucin. Always benign – observation with serial imaging of small asymptomatic lesions should be considered.
 small cysts < 2 cm in diameter. Olygocystic variant 2 cm difficult to distinguish from MCN. Cyst fluid CEA < 192 ng/ml, Contain no mucin. Always benign – observation with serial imaging of small asymptomatic lesions should be considered..")
10
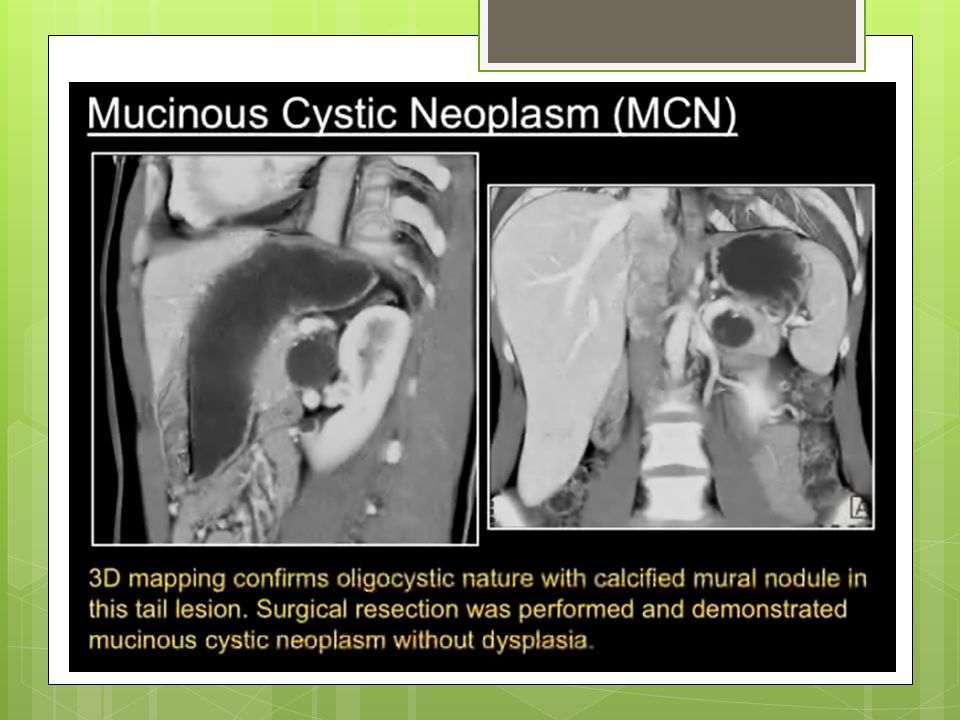
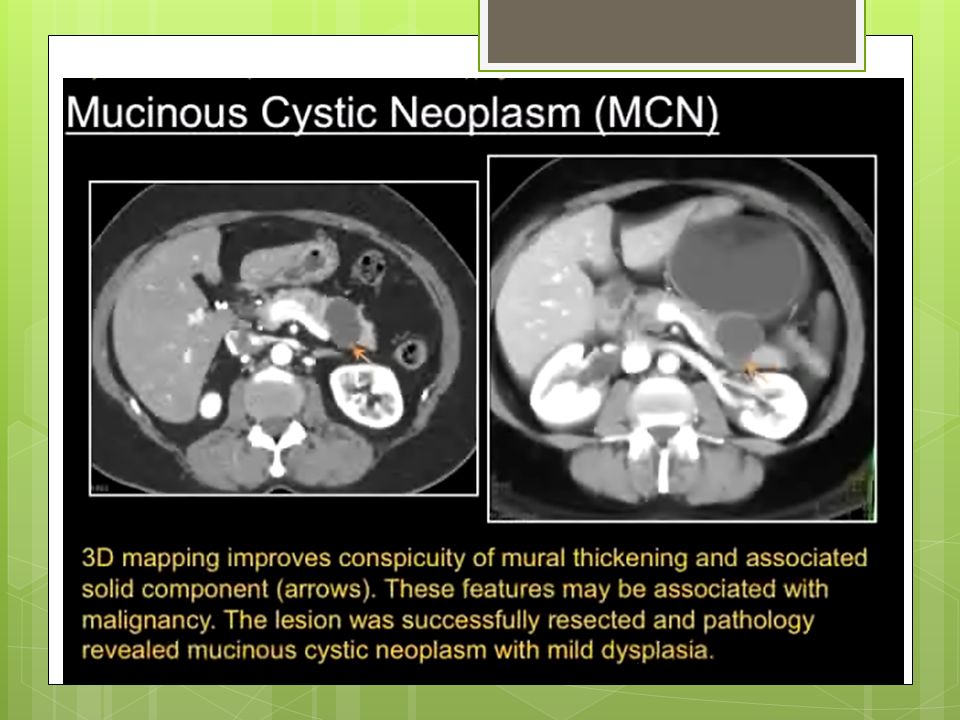
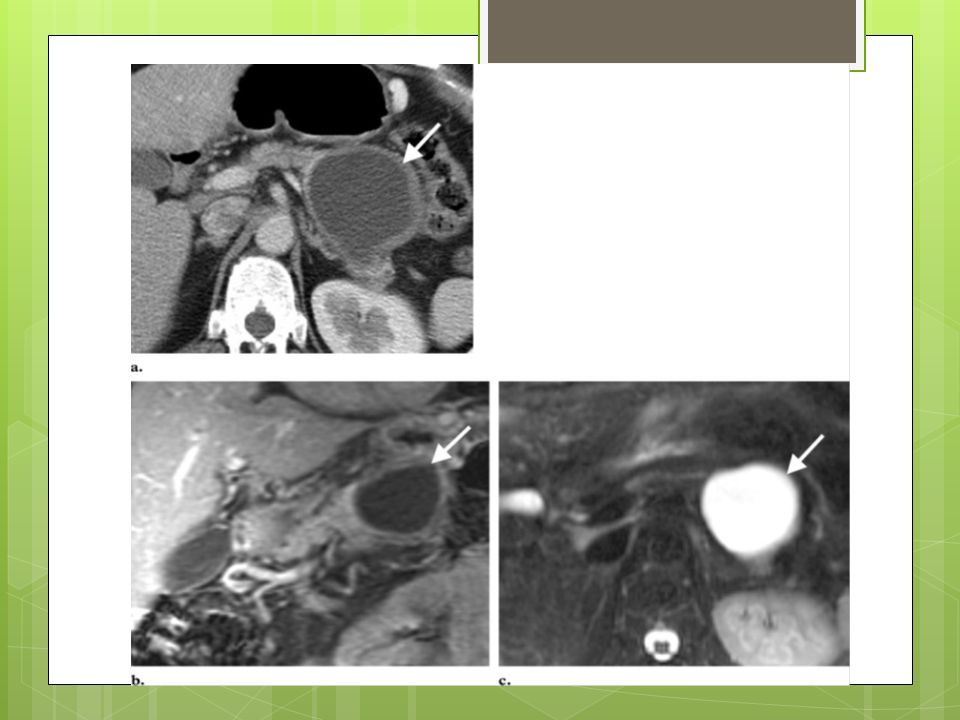
Mucinous Cystadenoma(MCN) Woman 50 years of age – “mothers lesion” Most common location in pancreatic tail Cysts typically > 2cm, < 6 Peripheral curvilinear calcifications and mural nodules on CT. Biopsy unreliable – benign appearing epithelium adjacent to invasive carcinoma. Graded pathologically by degree of dysplasia – always surgical management. CEA > 192 ng/ml

13
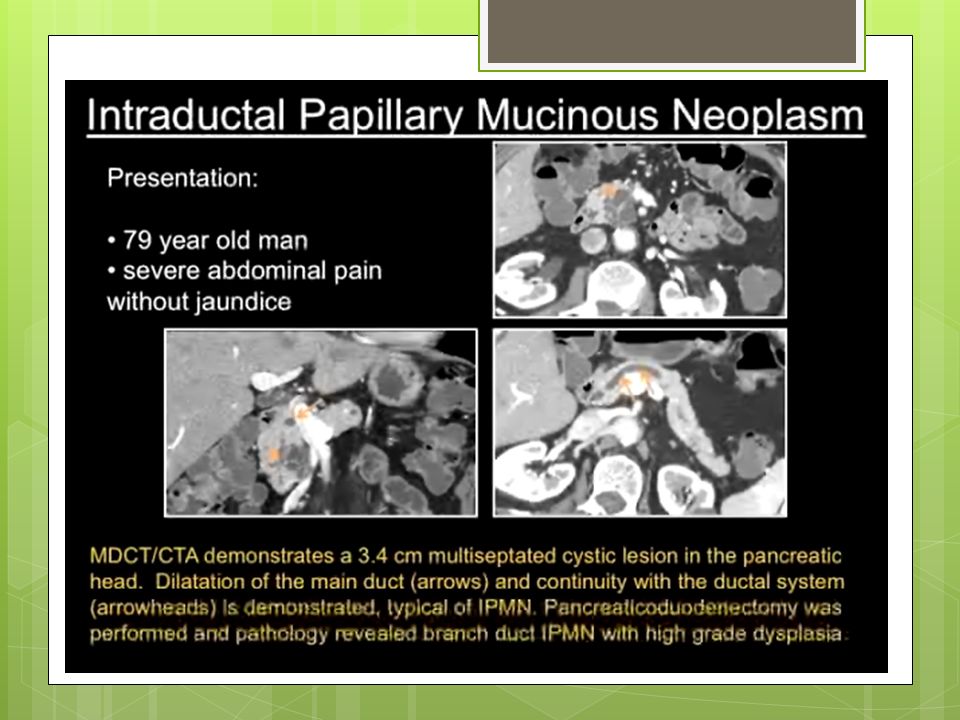
Intraductal Papillary Mucinous Neoplasms(IPMN) Equally common in men and women. Main duct and side branch duct or combined variants.Can be multiple. Main duct variant lead to dilatation of pancreatic duct to > 10 mm even if discrete lesion is not visualized, and has high malignant potential – surgical lesions Side duct variant typically situated in uncinate process,does not dilate the main duct and has lesser tendency to become malignant – < 3cm can be followed. Adenoma – Carcinoma sequence – slow growing. Diagnosis based on demonstration of connection with ductal system – MRCP. Patulous papil with mucin pouring from it a typical endoscopic finding during ERCP. > CEA and Amylase (communicate with pancreatic duct)
.")
15
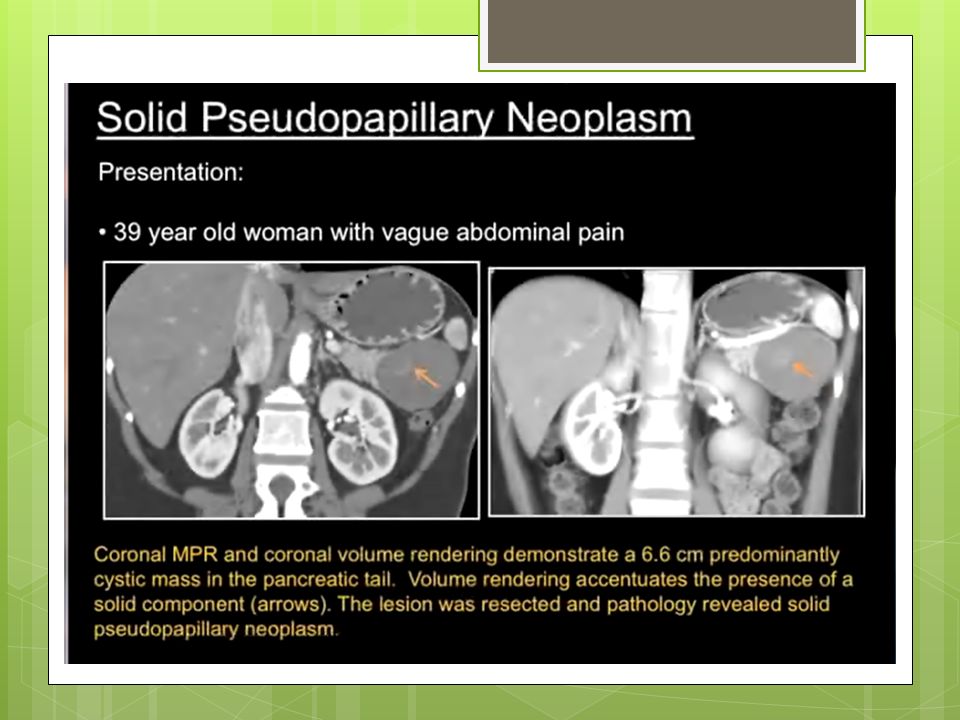
SPEN(Solid Pseudopapillary Epithelial Neoplasm) Tumor of younger woman(20 - 30 years ) – “daughter lesion” Benign – low grade malignant tumor growing slowlly, but can rarely disseminate. Encapsulated, large cystic - solid mass. Hypodense areas on CT represent necrosis/bleeding in tumor. Excellent survival rates post resection - warrant aggressive surgical approach.

17
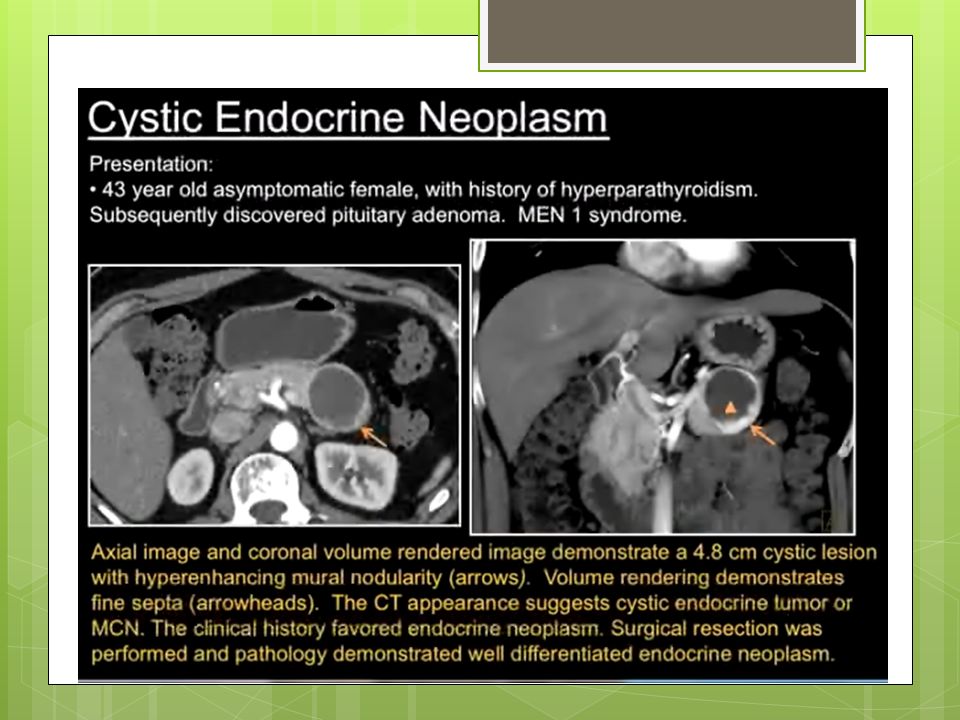
Cystic Endocrine Tumor Syndromic or Non Syndromic. Peripheral rim enhancement – look for hypervascular lesions in the liver. Should be differentiated from cystic adeno carcinoma as aggressive surgery has a much better prognosis.

19
Cystic Metastases Sarcomas,Ovarian CA,Melanoma metastases to pancreas RCC

21
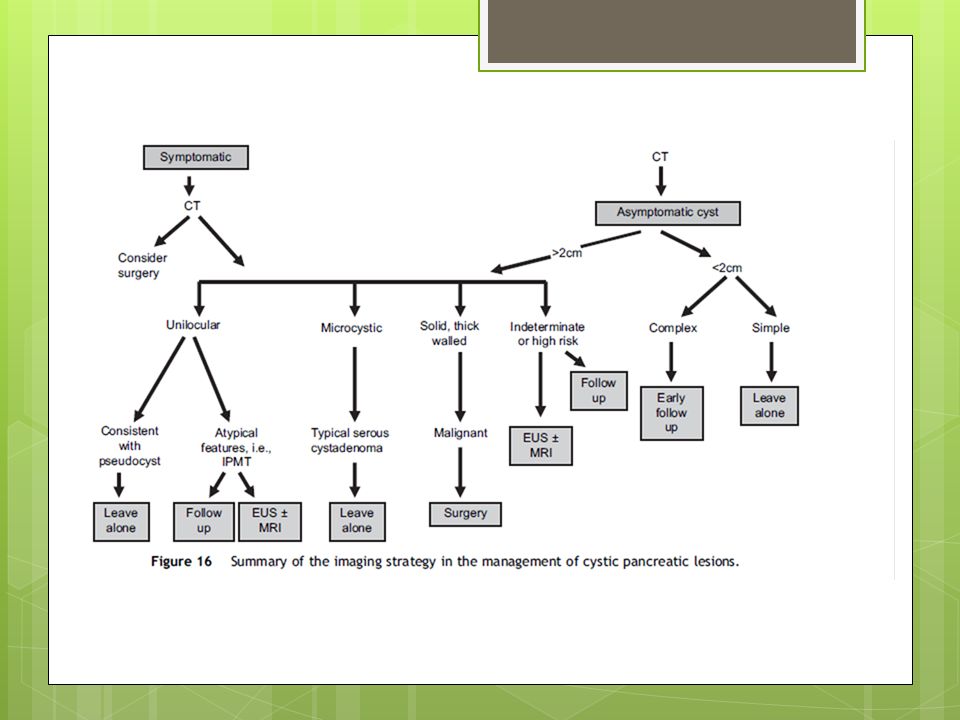
Pseudocyst Typical unilocular cysts in/adjacent to pancreas following a episode of acute pancreatitis or in the background of chronic pancreatitis. Smooth non enhancing wall. Content ussualy rich in amilase > 250ng/dl May resolve with time compared to neoplastic cysts that persists – follow in 4-6 weeks if uncertain.

24
References Clinical Radiology (2007) 62, 930-937 An evidence- based review for the management of cystic pancreatic lesions :A.C. Planner, E.M. Anderson*, A. Slater, J. Phillips-Hughes,H.K. Bungay, M. Betts Cystic Tumors of the Pancreas: Ultrasound, Computed Tomography, and Magnetic Resonance Imaging Features Seminars in Ultrasound, CT, and MRI, Volume 28, Issue 5, October 2007, Pages 339-356 Cystic Tumors of the Pancreas: Ultrasound, Computed Tomography, and Magnetic Resonance Imaging Features Radiographics 11/2005 1471 -1484 :Cystic Pancreatic Lesions: A Simple Imaging-based Classification System for Guiding Management Evaluation of Cystic Pancreatic Tumors over 3 cm in size – the role of 3D mapping in lesion definition,differential diagnosis and patient management – Ctisus.com - accessed 04/04/2012

Similar presentations





 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")








: Principal.>")

: Principal Modality (2): Faculty.>")


