Download presentation
Presentation is loading. Please wait.

1
Human Herperviruses Subfamily Alphaherpesvirinae
Herpes simplex virus 1 (HSV-1) Herpes simplex virus 2 (HSV-2) Varicella-zoster virus (VZV=HHV-3) Subfamily Betaherpesvirinae Cytomegalovirus (CMV=HHV-5) Human herpes viruses 6, 7 (HHV-6, HHV-7) Subfamily Gammaherpesvirinae Epstein-Barr virus (EBV=HHV-4) Human herpes virus 8 (HHV-8)
 Herpes simplex virus 2 (HSV-2) Varicella-zoster virus (VZV=HHV-3) Subfamily Betaherpesvirinae. Cytomegalovirus (CMV=HHV-5) Human herpes viruses 6, 7 (HHV-6, HHV-7) Subfamily Gammaherpesvirinae. Epstein-Barr virus (EBV=HHV-4) Human herpes virus 8 (HHV-8)")
2
Alpha herpesviruses Short reproductive cycle; Rapid spread;
Multiplication in epithelial cells; Latent in sensory ganglia; Destruction of infected cells HSV 1 and 2 VZV

3
Beta herpesviruses Long reproductive cycle; Slow infectivity;
Latent in monocytes, salivary glands, tonsils, kidneys; Infected cells become large. CMV HHV6 HHV7

4
Gamma herpesviruses Infection specific to T or B lymphocytes;
Latent in lymphoid tissue, lymphocytes, salivary glands, epithelial cells of mouth and pharynx. Proliferation of B-lymphocytes. EBV HHV 8

5
Herpes Simplex Viruses
- Herpetic gingivostomatitis; - Herpes labialis (cold sore); - Herpetic keratoconjunctivitis; - Skin manifestations; - HS meningitis and encephalitis; - Genital herpes; - Neonatal herpes.
; - Herpetic keratoconjunctivitis; - Skin manifestations; - HS meningitis and encephalitis; - Genital herpes; - Neonatal herpes.")
6
Herpes virus structure
Ds linear DNA enveloped virus with icosahedral capsid. Tegument contains viral proteins and enzymes for replication.

7
Glycoprotein "spikes" on the HSV surface.
Glycoprotein B (gB) is clearly visualised in clusters of spikes about 10 nm in length. Between the capsid and the envelope is an ill-defined layer of proteins, collectively known as the tegument.
 is clearly visualised in clusters of spikes about 10 nm in length. Between the capsid and the envelope is an ill-defined layer of proteins, collectively known as the tegument.")
8
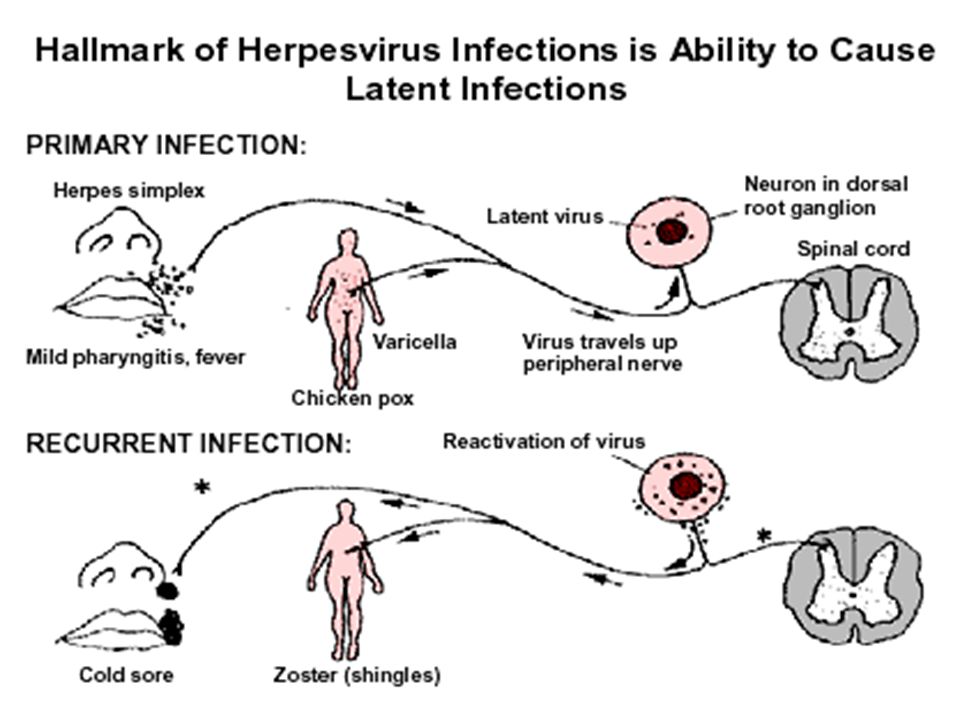
Pathogenesis Transmission: - Contact of infected lesions;
- HSV 1 = oral-oral; oral-genital; - HSV 2 = primarily genital-genital. Local multiplication: - Mucous membranes; - No systemic illness. Virus spread along neurons Latent infection – sensory cranio-spinal ganglia

9
HSV1 can set up a primary infection in the lips, move to the trigeminal ganglion where it can remain latent. Virus can subsequently reactivate, move to the original site of infection and result in cold sores. Reactivation: physical or psychological stress, infection, fever, irradiation; including sunlight, and menstruation.

10
Site at which HSV-1 and HSV-2 cause disease in humans

11
Clinical manifestation
Gingivostomatitis occurs most frequently in children less than 5 years of age. Symptoms: fever, sore throat, pharyngeal edema and erythema, vesicular or ulcerative lesions on the oral and pharyngeal mucosa. Recurrent HSV infections of the oropharynx - herpes labialis (cold sores), usually appear on the vermillion border of the lip. Gingivostomatitis looks different from a cold sore, occurs only once
, usually appear on the vermillion border of the lip. Gingivostomatitis looks different from a cold sore, occurs only once.")
12
Genital Herpes is caused by HSV 2 and HSV 1.
Primary infection usually involves: In women: the vulva, vagina, and cervix. In men: the glans penis, prepuce or penile shaft. Clinical manifestation: fever, malaise, anorexia, bilateral inguinal lymphadenopathy, dysuria and urinary retention due to urethral involvement. As many as 10 % of individuals develop an aseptic meningitis. Recurrence – 60%. The complete healing takes several weeks.

13
Clinical manifestation
Herpetic Keratitis It is usually caused by HSV 1 and is accompanied by conjunctivitis. The characteristic lesions are dendritic ulcers. Deep stromal involvement may result in visual impairment. Skin Manifestations At any skin site. Lesions on abraded skin of the fingers, known as herpetic whitlows. Wrestlers because of physical contact may develop herpes gladiatorum. Herpes Simplex Encephalitis hemorrhagic necrosis of the inferiomedial portion of the temporal lobe. clinical manifestations: headache, fever, altered consciousness, and abnormalities of speech and behavior. mortality rate %.

14
Neonatal Herpes Simplex Virus Infection
It usually results from contact of the fetus with infected maternal genital secretions at the time of delivery. Manifestations: 1) Skin, eye and mouth disease consists of cutaneous lesions and does not involve other organ systems. 2) Encephalitis. 3) Disseminated infection involves multiple organ systems and can produce disseminated intravascular coagulation, hemorrhagic pneumonitis, encephalitis, and cutaneous lesions. The mortality rate: - zero for skin, eye and mouth disease; - 15 % for encephalitis; - 60 % for neonates with disseminated infection.
 Skin, eye and mouth disease consists of cutaneous lesions and does not involve other organ systems. 2) Encephalitis. 3) Disseminated infection involves multiple organ systems and can produce disseminated intravascular coagulation, hemorrhagic pneumonitis, encephalitis, and cutaneous lesions. The mortality rate: - zero for skin, eye and mouth disease; - 15 % for encephalitis; - 60 % for neonates with disseminated infection.")
15
Neonatal herpes infection

16
Laboratory Diagnosis Direct Detection:
Tzanck smear (multinucleated giant cells). Immunofluorescence of skin scrappings. PCR. Virus Isolation on cell culture Identification: IF, ELISA Serology: ELISA. Used to document to recent infection. CPE of HSV in cell culture: Note the ballooning of cells.
. Immunofluorescence of skin scrappings. PCR. Virus Isolation on cell culture. Identification: IF, ELISA. Serology: ELISA. Used to document to recent infection. CPE of HSV in cell culture: Note the ballooning of cells.")
17
Varicella-zoster virus
Differs from HSV: - Respiratory secretions transmission; - Systemic disease; - Rash itches; - Latent in multiple sensory ganglia. Live attenuated vaccine

18
Major Diseases Associated with HZV
Varicella or chicken pox Zoster or shingles Post-infectious encephalitis Neonatal infection

20
The incubation period - from 11 to 23 days.
Varicella Varicella or chickenpox is the manifestation of primary varicella-zoster virus infection. The incubation period - from 11 to 23 days. The rash begins on the face and trunk and spreads to the extremities. The average duration of lesion formation is 3 to 5 days in the normal child; however, it is usually longer in adolescents, adults and in the immunocompromised Latency - in the cerebral or posterior root ganglia.

21
Lesions appear in “crops’ on successive
days, so (unlike most rashes) all stages of rash can be present at once: papules, vesicles, scabs
 all stages. of rash can be present at once: papules, vesicles, scabs.")
22
Chicken pox

23
Herpes Zoster or shingles
is the recurrent form of varicella-zoster virus. It is a reactivation of latent virus, manifests as a localized vesicular rash with a dermatomal distribution. The virus reactivates in the ganglion and tracks down the sensory nerve to the area of the skin innervated by the nerve. It is accompanied by intensive pain which may last for months (postherpetic neuralgia)
")
24
Shingles

25
Chickenpox of the newborn
The infant contracted chickenpox from her infected mother. Congenital varicella syndrome: Scarring of skin Hypoplasia of limbs CNS and eye defects Death in infancy normal

26
Laboratory diagnosis of varicella zoster virus infections
Direct detection in skin lesions: Tzanck smear (multinucleated giant cells with nuclear inclusions). Immunofluorescence. PCR in the diagnosis of VZV meningoencephalitis from CSF. Virus isolation from vesicle fluid on cell culture CPE Identification: IF Serology (IgG in paired acute and convalescent sera; IgM tests are likely to prove invaluable in determining the nature of congenital varicella infections): ELISA, IF, CFT.
. Immunofluorescence. PCR in the diagnosis of VZV meningoencephalitis from CSF. Virus isolation from vesicle fluid on cell culture. CPE Identification: IF. Serology (IgG in paired acute and convalescent sera; IgM tests are likely to prove invaluable in determining the nature of congenital varicella infections): ELISA, IF, CFT.")
27
Cytomegalovirus Asymptomatic shedding: • Urine • Oral secretions
• Cervical secretions • Semen • Breast milk No destruction of infected cells. Cytomegaly.

28
Pathogenesis of cytomegalovirus
Routs of transmission: - direct contact with infected body fluids: saliva, breast milk, urine; - sexual intercourse; - blood transfusions; - respiratory; - fecal-oral; - trancplacentally; - organ transplantation. Infects epithelial cells and leukocytes. Spread to all organs. Virus shed in body fluids many years. Latent in neutrophils, monocytes, salivary glands, tonsils, kidneys.

29
Clinical manifestation
Congenital cytomegalovirus infection - 1 % of all live births. Children acquire infection through: contact with infected maternal genital secretions, transplacentally, breast milk. Severe symptomatic disease: hepatosplenomegaly, myocarditis, optic atrophy, deafness, pneumonitis, involvement of the CNS.

30
Clinical manifestation
Mononucleosis-like syndrome. in approximately 10 % of primary infections in older children and adults; Manifestations: fever, malaise, atypical lymphocytosis, pharyngitis, rarely, cervical adenopathy or hepatitis.

31
Clinical manifestation
Cytomegalovirus infection in severely immunocompromised individuals - life-threatening disease from either primary or reactivated infection. Infection can involve: lungs, gastrointestinal tract, liver, retina, CNS. Individuals at high risk for severe disease (CMV pneumonia): organ transplant recipients, particularly bone marrow transplant recipients, individuals with human immunodeficiency virus infection.
: organ transplant recipients, particularly bone marrow transplant recipients, individuals with human immunodeficiency virus infection.")
32
Laboratory diagnosis of cytomegalovirus infection
Specimens: blood, breast milk, urine, saliva, liquor. Methods: - Nuclear inclusions (owl’s eyes) are surrounded by a clear halo that extends to the nuclear membrane - PCR. - Cultivation. Identification: IF, ELISA. - Serology: IF, CFT, NtT.
 are surrounded by a clear halo that extends to the nuclear membrane. - PCR. - Cultivation. Identification: IF, ELISA. - Serology: IF, CFT, NtT.")
33
Epstein-Barr virus Infectious mononucleosis.
Associated with human tumors: Burkitt’s lymphoma; Nasopharyngeal carcinoma; B-lymphoma; Hodgkin's lymphoma; Hair-like oral leukoplakia

34
Pathogenesis Epstein-Barr virus infection
Transmission: by contact with saliva, in particularly through kissing, transfusions and organ transplantation can spread infected leukocytes. Virus multiplies in: epithelial cells of mouth, local lymph tissue, T- and B-lymphocytes. Carriers shed virus for lifetime.

35
Clinical manifestation
Infectious mononucleosis. The predominant findings: malaise, fever, pharyngitis, cervical adenopathy, splenomegaly. A conjunctival hemorrhage of the right eye of a patient with infectious mononucleosis

36
Main symptoms of infectious mononucleosis

37
Burkitt's Lymphoma

38
Burkitt's Lymphoma B-lymphoma

39
Host cell pathology No cytopathic effects. No inclusion bodies.
Virus can transform B cell cultures (proliferation)
")
40
Host immune response Stimulated (infected) B cells produce:
Polyclone immunoglobulins (heterphile Abs); Viral membrane antigens. Increase in activated T cells: “Atypical lymphocytes”; Abnormal lymphocytes in blood (Downy cells). Cytotoxic T cells reduce number infected B cells. Immunosuppression = lymphomas.
; Viral membrane antigens. Increase in activated T cells: Atypical lymphocytes ; Abnormal lymphocytes in blood (Downy cells). Cytotoxic T cells reduce number infected. B cells. Immunosuppression = lymphomas.")
41
Diagnosis EBV Histology: Downy cells (atypical lymphocytes).
Detection of heterophile antibodies: Agglutinate sheep RBCs; Serology: Ig M against the Capsid Antigen = early; Raising of the titer of the anti-EBV Nuclear Antigen. 3-6 weeks post infection

42
HHV-6 and 7 Transmission: through contact with saliva and breast feeding. The main target cells are the T-lymphocyte and B-lymphocytes. HHV-6 and HHV-7 become latent following primary infection and are reactivated from time to time, especially during periods of immunosuppression. HHV-6 infection is firmly associated with: roseala infantum, meningitis, encephalitis, symptoms in transplant recipients such as fever, liver and CNS manifestations. HHV-6 and 7 is associated with chronic fatigue syndrome: fatigue, arthralgia, sweating, lymphadenopathy.

43
Rosealla infantum most common in children age 6 months to 2 years. The symptoms are respiratory illness, followed by a high fever (which can trigger seizures) for up to eight days. Fevers abruptly end and are followed by a rash on the trunk, then the extremities.
 for up to eight days. Fevers abruptly end and are followed by a rash on the trunk, then the extremities.")
44
Human Herpes Virus 8 Is associated with Kaposi’s sarcoma, malignancies such as Castleman’s disease and primary effusion lymphomas. HHV-8 DNA is found in almost 100% of cases of Kaposi’s sarcoma. Most patients with KS have antibodies against HHV-8. The seroprevalence of HHV-8 is low among the general population but is high in groups of individuals susceptible to KS, such as homosexuals.

45
Kaposi’s Sarcoma (HHV 8)
KS is a systemic disease that can present with cutaneous lesions with or without internal involvement. KS can involve the oral cavity, lymph nodes, and viscera of gastrointestinal and respiratory tract. Morphologies of cutaneous lesions: macular, patch, plaque, nodular. The AIDS-related KS lesions affect the upper trunk, face, and oral cavity Transmission: through saliva (by kissing), organ transplantation, blood transfusion.
, organ transplantation, blood transfusion.")
46
Treatment of herpesviruses infections
Acyclovir is the treatment of choice for: mucocutaneous HSV infections, herpes simplex encephalitis, neonatal HSV infections, varicella-zoster virus infections in the immunocompromised individuals. Valaciclovir, and famciclovir is the treatment for shingles. Ganciclovir and foscarnet are used for the treatment of cytomegalovirus infection in immunocompromised individuals.

47
Mechanism of action of acyclovir
In cell acyclovir develops in mono-, dy- and three phosphate. The first step is induced by viral timidinkinase, following phosphorilation cellular kinase induce. Produced acycloguanosinthreephosphate inhibits viral DNA-polymerase and so nucleic acid synthesis. Hence, acyclovir does not inhibit DNA synthesis in noninfected cells because of absence of its active form.

Similar presentations






>")




>")


 DNA virus HSV 1 and HSV 2.>")




