Download presentation
Presentation is loading. Please wait.

1
Metabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications for Preventive Cardiology Nathan D. Wong, PhD, FACC, FAHA Professor and Director Heart Disease Prevention Program Division of Cardiology University of California, Irvine

2
Overview of Diabetes in the United States

3
Diabetes Prevalence, 1990-1998

4
Age-adjusted prevalence of physician-diagnosed diabetes in Adults age 18 and older by race/ethnicity and sex (NHANES: 1999-2004). Source: NCHS and NHLBI. NH – non-Hispanic.

7
Risk of Cardiovascular Events in Diabetics Framingham Study Age-adjusted Biennial Rate Age-adjusted Per 1000 Risk Ratio Cardiovascular Event Men Women Men Women Coronary Disease 39 21 1.5** 2.2*** Stroke15 6 2.9*** 2.6*** Peripheral Artery Dis. 18 18 3.4*** 6.4*** Cardiac Failure 23 21 4.4*** 7.8*** All CVD Events 76 65 2.2*** 3.7*** Subjects 35-64 36-year Follow-up **P<.001,***P<.0001 _________________________________________________________________

8
Insulin Resistance

9
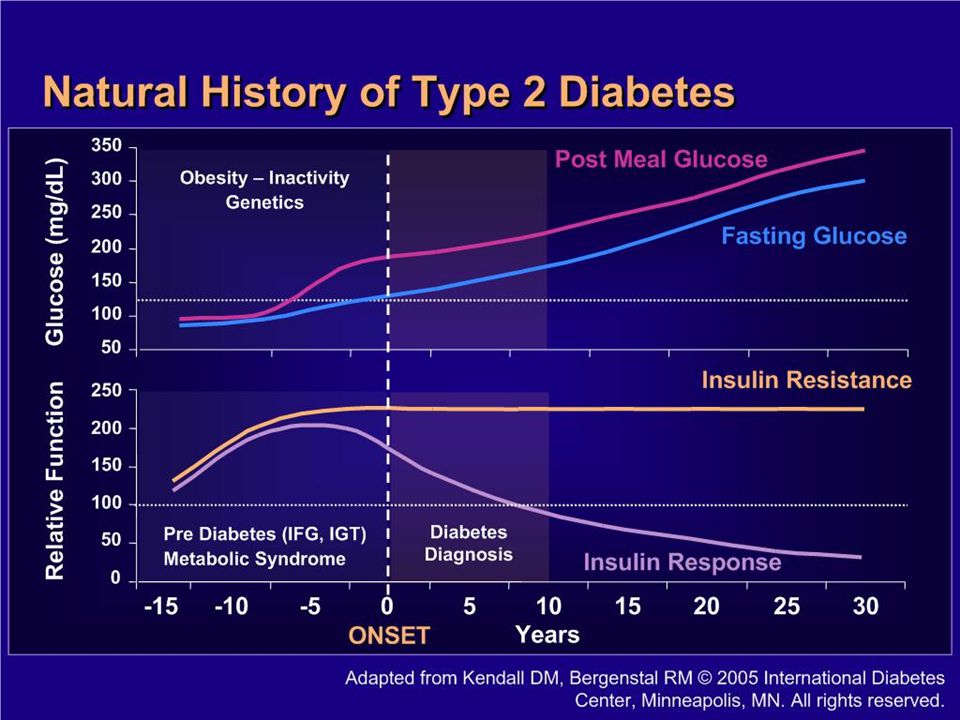
Natural History of Type 2 Diabetes

10
Development of Type 2 Diabetes

11
Hyperglycemia in Type 2 Diabetes Results From Three Major Metabolic Defects

12
Relationship Between Obesity and Insulin Resistance and Dyslipidemia

13
Insulin Resistance: Associated Conditions

14
New Cases of ESRD in the United States

15
New Cases of ESRD in the United States by Cause and Ethnicity, 1998

16
Microalbuminuria

17
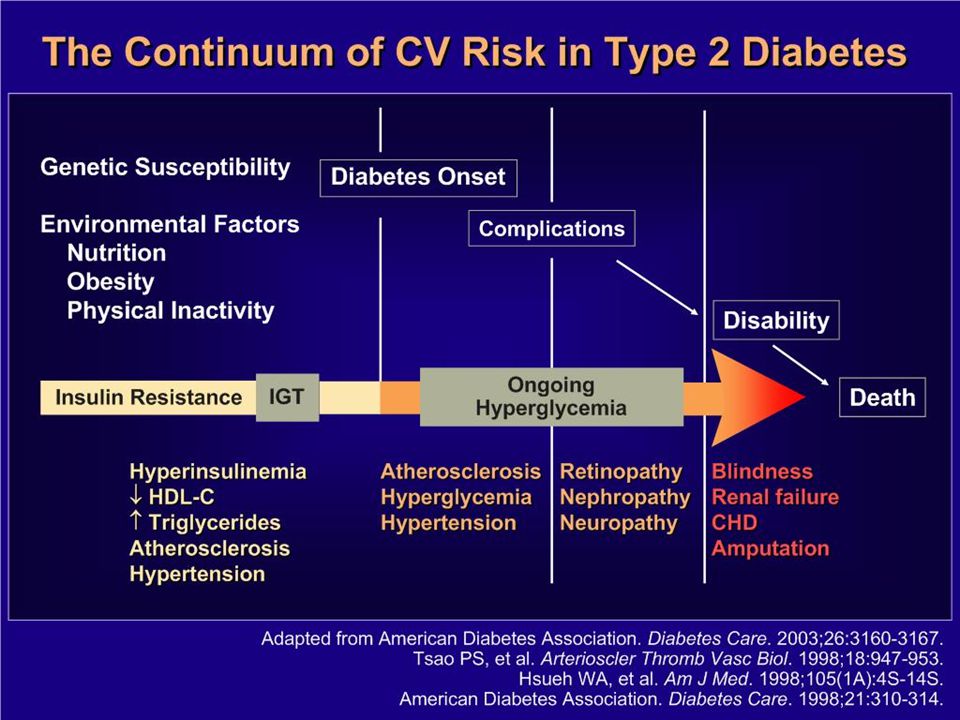
Cardiovascular Disease and Diabetes

18
Probability of Death From CHD in Patients With Type 2 Diabetes With or Without Previous MI

19
Framingham Heart Study 30-Year Follow-Up: CVD Events in Patients With Diabetes (Ages 35-64) 10 9 20 11 9638 19 3* 30 0 2 4 6 8 10 Age-adjusted annual rate/1,000 MenWomen Total CVD CHDCardiac failure Intermittent claudication Stroke Risk ratio P<0.001 for all values except *P<0.05. Wilson PWF, Kannel WB. In: Hyperglycemia, Diabetes and Vascular Disease. Ruderman N et al, eds. Oxford; 1992.

20
Presentation Name: WJC Age: 54 years old Professional: former chief executive Personal: wife lives principally in Washington, DC; he has a personal cook in his suburban NY home Lifestyle: –Occasional use of cigars –has had a long-term weight problem –likes to play golf

21
Presentation (cont’d) Examination: –Height: 6 ft 2 in –Weight: 220 lb (BMI 28 kg/m 2 ) –Waist circumference: 41 in –BP: 150/88 mm Hg –P: 64 bpm –RR: 12 breaths/min Cardiopulmonary exam: normal
 Examination: –Height: 6 ft 2 in –Weight: 220 lb (BMI 28 kg/m 2 ) –Waist circumference: 41 in –BP: 150/88 mm Hg –P: 64 bpm –RR: 12 breaths/min Cardiopulmonary exam: normal")
22
Presentation (cont’d) Medications: –sildenafil 50 mg prn –amlodipine 5 mg/d Laboratory results: –TC: 220 mg/dL –HDL-C: 36 mg/dL –LDL-C: 140 mg/dL –TG: 220 mg/dL –FBS: 120 mg/dL
 Medications: –sildenafil 50 mg prn –amlodipine 5 mg/d Laboratory results: –TC: 220 mg/dL –HDL-C: 36 mg/dL –LDL-C: 140 mg/dL –TG: 220 mg/dL –FBS: 120 mg/dL")
23
The Metabolic Syndrome Insulin Resistance Hypertension Type 2 Diabetes Disordered Fibrinolysis Complex Dyslipidemia TG, LDL HDL Endothelial Dysfunction Systemic Inflammation Athero- sclerosis Visceral Obesity Adapted from the ADA. Diabetes Care. 1998;21:310-314; Pradhan AD et al. JAMA. 2001;286:327-334.

24
Revised ATP III Metabolic Syndrome Oct 2005 *Diagnosis is established when 3 of these risk factors are present. † Abdominal obesity is more highly correlated with metabolic risk factors than is BMI. ‡ Some men develop metabolic risk factors when circumference is only marginally increased. <40 mg/dL <50 mg/dL or Rx for ↓ HDL Men Women >102 cm (>40 in) >88 cm (>35 in) Men Women 100 mg/dL or Rx for ↑ glucose Fasting glucose 130/ 85 mm Hg or on HTN Rx Blood pressure HDL-C 150 mg/dL or Rx for ↑ TG TG Abdominal obesity † (Waist circumference ‡ ) Defining LevelRisk Factor
 >88 cm (>35 in) Men Women 100 mg/dL or Rx for ↑ glucose Fasting glucose 130/ 85 mm Hg or on HTN Rx Blood pressure HDL-C 150 mg/dL or Rx for ↑ TG TG Abdominal obesity † (Waist circumference ‡ ) Defining LevelRisk Factor.")
25
International Diabetes Federation Definition: Abdominal obesity plus two other components: elevated BP, low HDL, elevated TG, or impaired fasting glucose

32
Prevalence of the Metabolic Syndrome Among US Adults NHANES 1988-1994 Prevalence (%) 0 5 10 15 20 25 30 35 40 45 20-2930-3940-4950-5960-69> 70 Men Women Age (years) Ford E et al. JAMA. 2002(287):356. 1999-2002 Prevalence by IDF vs. NCEP Definitions (Ford ES, Diabetes Care 2005; 28: 2745-9) (unadjusted, age 20+) NCEP : 33.7% in men and 35.4% in women IDF: 39.9% in men and 38.1% in women
: Prevalence by IDF vs. NCEP Definitions (Ford ES, Diabetes Care 2005; 28: ) (unadjusted, age 20+) NCEP : 33.7% in men and 35.4% in women IDF: 39.9% in men and 38.1% in women.")
33
Prevalence of the NCEP Metabolic Syndrome: NHANES III by Sex and Race/Ethnicity Prevalence, % Men Ford ES et al. JAMA 2002;287:356-359. Women White African American Mexican American Other25% 16% 28% 21% 23% 26% 36% 20%

34
Cardiovascular Disease (CVD) and Total Mortality: US Men and Women Ages 30-74 (age, gender, and risk-factor adjusted Cox regression) NHANES II Follow- Up (n=6255)(Malik and Wong, et al., Circulation 2004; 110: 1245-1250 ) * p<.05, ** p<.01, **** p<.0001 compared to none * *** ** ***
 and Total Mortality: US Men and Women Ages (age, gender, and risk-factor adjusted Cox regression) NHANES II Follow- Up (n=6255)(Malik and Wong, et al., Circulation 2004; 110: ) * p<.05, ** p<.01, **** p<.0001 compared to none * *** ** ***")
36
Metabolic Syndrome, CVD Events, and Mortality European cohort studies (6156 men and 5356 women): Modified WHO definition of MetS associated with all- cause mortality (RR=1.44 [1.17-1.84] in men and 1.38 [1.02-1.87] in women) and CVD mortality (RR=2.26 [1.61- 3.17] in men and 2.78 [1.57-4.94 in women) (Hu et al. Arch Intern Med 2004; 164: 1066-76) Atherosclerosis Risk in Communities (ARIC) study (12,089 men and women): 11 year follow-up, ATP III MetS associated with 1.5-2-fold greater likelihood of developing CHD and stroke, but MetS did not improve prediction over FRS (McNeill et al. Diab Care 2005; 28: 385-90) Cardiovascular Health Study (CHS) (2,175 elderly subjects): ATP III definition associated with 38% increased risk (p<0.01) of coronary/cerebrovascular events (Scuteri et al., Diab Care 2005; 28: 882-7)
![Metabolic Syndrome, CVD Events, and Mortality European cohort studies (6156 men and 5356 women): Modified WHO definition of MetS associated with all- cause mortality (RR=1.44 [ ] in men and 1.38 [ ] in women) and CVD mortality (RR=2.26 [ ] in men and 2.78 [ in women) (Hu et al.](http://images.slideplayer.com/20/5983422/slides/slide_36.jpg "Arch Intern Med 2004; 164: ) Atherosclerosis Risk in Communities (ARIC) study (12,089 men and women): 11 year follow-up, ATP III MetS associated with fold greater likelihood of developing CHD and stroke, but MetS did not improve prediction over FRS (McNeill et al. Diab Care 2005; 28: ) Cardiovascular Health Study (CHS) (2,175 elderly subjects): ATP III definition associated with 38% increased risk (p<0.01) of coronary/cerebrovascular events (Scuteri et al., Diab Care 2005; 28: 882-7).")
Similar presentations








 describes relative weight for height: weight (kg)/height (m 2 ) Overweight = 25–29.9 BMI Obesity = >30 BMI.>")




? and why is it so dangerous? - Diagnosing PAD in the primary care.>")








![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")


