Download presentation
Presentation is loading. Please wait.

1
Final Exam Tuesday, 6/5, 2 PM Closed book – Essay and MC/TF Determining Energy Needs – p234-246 – Indirect calorimetry – Be able to do the calculations given RQ table, VO2, VCO2 – Principles of indirect calorimetry – Don’t memorize H-B or WHO equations

2
Final Exam Protein status – AMA (will give you equations, 233-234) – Biochemical assessments (321-327) Iron status (327-332) – Know markers (and their rationale) of iron status – Be able to interpret lab values Glucose (fasting & GTT) (303-307) – principle & interpretation Lipoproteins & CHD (262-272) – Assessment only, not treatment – CHD risk assessment using ATP III – Know cut points
 – Biochemical assessments ( ) Iron status ( ) – Know markers (and their rationale) of iron status – Be able to interpret lab values Glucose (fasting & GTT) ( ) – principle & interpretation Lipoproteins & CHD ( ) – Assessment only, not treatment – CHD risk assessment using ATP III – Know cut points")
3
Update: Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) David L. Gee, PhD Professor of Food Science and Nutrition Central Washington University

4
National Cholesterol Education Program (NCEP) History Adult Treatment Panel I (ATP I) – 1988 – strategy for primary prevention of CHD – established cutoff values for TC, HDL-C, LDL-C and CHD risk factors
 History Adult Treatment Panel I (ATP I) – 1988 – strategy for primary prevention of CHD – established cutoff values for TC, HDL-C, LDL-C and CHD risk factors")
5
National Cholesterol Education Program (NCEP) Children’s Treatment Panel – 1991 ATP II – 1993 – reaffirmed ATP I – secondary prevention of CHD
 Children’s Treatment Panel – 1991 ATP II – 1993 – reaffirmed ATP I – secondary prevention of CHD")
6
National Cholesterol Education Program (NCEP) ATP III – May 2001 – reaffirms ATP I, II New features – primary prevention in persons with multiple risk factors – modifies lipid classifications – modifies implementation of prevention measures
 ATP III – May 2001 – reaffirms ATP I, II New features – primary prevention in persons with multiple risk factors – modifies lipid classifications – modifies implementation of prevention measures")
7
Initial CHD Risk Assessment Fasting lipoprotein profile – adults > 20 yrs old – every 5 years – TC, LDL-C, HDL-C, TG Non-fasted blood sample – only TC and HDL-C usable – LDL-C = TC - HDL-C - (TG/5)
")
8
ATP III Classification of LDL- Cholesterol (mg/dl) LDL Cholesterol – < 100 optimal – 100-129near/above optimal – 130-159borderline high – 160-189high – >190very high
 LDL Cholesterol – < 100 optimal – near/above optimal – borderline high – high – >190very high")
9
ATP III Classification of Total and HDL Cholesterol (mg/dl) Total Cholesterol – <200desirable – 200-239borderline high – >240high HDL Cholesterol – <40low (bad) – >60high(good)
 Total Cholesterol – <200desirable – borderline high – >240high HDL Cholesterol – <40low (bad) – >60high(good)")
10
LDL Cholesterol Goals and Cutpoints for Therapeutic Lifestyle Changes (TLC) and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: 130 10-year risk <10%: 160 130<130 2+ Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category
 and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: year risk <10%: 160 130< Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category")
11
CHD Risk Equivalents Have risk of major coronary event equal to that of established CHD Other forms of atherosclerotic disease – peripheral arterial disease – abdominal aortic aneurysm – symptomatic carotid artery disease Diabetes Multiple risk factors that confer a 10- year risk for CHD > 20%

12
LDL Cholesterol Goals and Cutpoints for Therapeutic Lifestyle Changes (TLC) and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: 130 10-year risk <10%: 160 130<130 2+ Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category
 and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: year risk <10%: 160 130< Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category")
13
Major Risk Factors that Modify LDL-Goals Cigarette smoking hypertension (BP>140/90 or on anti-hypertensive medication) low HDL-C (<40mg/dl) – high HDL-C (>60mg/dl) “negative risk factor” family history of premature CHD – 1 o male relative < 55yrs – 1 o female relative <65yrs age – men > 45 yrs – women > 55 yrs
 low HDL-C (<40mg/dl) – high HDL-C (>60mg/dl) negative risk factor family history of premature CHD – 1 o male relative < 55yrs – 1 o female relative <65yrs age – men > 45 yrs – women > 55 yrs")
14
Estimating 10-Year CHD Risk Framingham Risk Score Short Term Risk (10-yr) for myocardial infarction – Based on: Age Total Cholesterol Smoking status HDL Systolic BP
 for myocardial infarction – Based on: Age Total Cholesterol Smoking status HDL Systolic BP")
15
Spreadsheet for determining Framingham 10-yr risk. Downloadable at: – http://hin.nhlbi.nih.gov/atpiii/riskcalc.htm Palm III Operating System download at: – http://hin.nhlbi.nih.gov/atpiii/atp3palm.htm – includes other information from ATP III

16
Categories of Risk and LDL-C Goals

17
LDL Cholesterol Goals and Cutpoints for Therapeutic Lifestyle Changes (TLC) and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: 130 10-year risk <10%: 160 130<130 2+ Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category
 and Drug Therapy in Different Risk Categories 190 (160–189: LDL- lowering drug optional) 160<1600–1 Risk Factor 10-year risk 10–20%: year risk <10%: 160 130< Risk Factors (10-year risk 20%) 130 (100–129: drug optional) 100<100 CHD or CHD Risk Equivalents (10-year risk >20%) LDL Level at Which to Consider Drug Therapy (mg/dL ) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dL) LDL Goal (mg/dL)Risk Category")
18
Therapeutic Lifestyle Changes in LDL-lowering Therapy TLC Diet Therapeutic options to lower LDL-C – plant stanols/sterols (2g/d) – viscous soluble fiber (10-25 g/d) Weight reduction Increase physical activity
 – viscous soluble fiber (10-25 g/d) Weight reduction Increase physical activity")
19
TLC diet SFA: < 7% of Calories PUFA: up to 10% of Calories MUFA: up to 20% of Calories Total Fat: 25-35% of Calories CHO: 50-60% of Calories fiber: 20-30g/d Cholesterol: < 200mg/d

20
Reinforce reduction in saturated fat and cholesterol Consider adding plant stanols/sterols Increase fiber intake Consider referral to a dietitian Initiate Tx for Metabolic Syndrome Intensify weight management & physical activity Consider referral to a dietitian 6 wks Q 4-6 mo Emphasize reduction in saturated fat & cholesterol Encourage moderate physical activity Consider referral to a dietitian Visit I Begin Lifestyle Therapies Visit 2 Evaluate LDL response If LDL goal not achieved, intensify LDL-Lowering Tx Visit 3 Evaluate LDL response If LDL goal not achieved, consider adding drug Tx A Model of Steps in Therapeutic Lifestyle Changes (TLC) Monitor Adherence to TLC Visit N
 Monitor Adherence to TLC Visit N")
21
Beyond LDL Lowering: Metabolic Syndrome as a Secondary Target of Therapy Cluster of risk factors Associated with insulin resistance Enhance risk of CHD at any LDL-C level

22
Diagnosis of Metabolic Syndrome Three or more of the following: Abdominal Obesity – men > 40” waist circumference – women > 35” waist circumference Hypertriglyceridemia (>150 mg/dl) Low HDL – men < 40 mg/dl – women < 50 mg/dl Hypertension (>130/>85 mmHg) Hyperglycemia (> 110 mg/dl)
 Low HDL – men < 40 mg/dl – women < 50 mg/dl Hypertension (>130/>85 mmHg) Hyperglycemia (> 110 mg/dl)")
23
Prevalence of the Metabolic Syndrome Among US Adults JAMA 287:356-359 (2002) NHANES III (8814 adults) Prevalence – 23.7% of adult population 47 million Americans – increases with age 6.7% of 20-29 yr olds 43.5% of 60-69 yr olds – overall, prevalence similar in men and women African-American women 57% higher Mexican-American women 26% higher
 NHANES III (8814 adults) Prevalence – 23.7% of adult population 47 million Americans – increases with age 6.7% of yr olds 43.5% of yr olds – overall, prevalence similar in men and women African-American women 57% higher Mexican-American women 26% higher")
24
Management of Metabolic Syndrome Control LDL-cholesterol Weight Control – enhances LDL-C lowering – reduces all risk factors of metabolic syndrome Physical Activity – reduces VLDL-TG – increases HDL-C – lowers LDL-C – lowers BP – reduces insulin resistance

25
ATP III Guidelines - Application Step 1 – Determine lipoprotein levels from fasted blood sample LDL-cholesterol – primary target of therapy – Total cholesterol – HDL-cholesterol

26
ATP III Guidelines - Application Step 2 – Identify presence of clinical atherosclerotic disease that confer high risk – Clinical CHD – CHD risk equivalents

27
ATP III Guidelines - Application Step 3 – Determine presence of major risk factors (other than LDL) cigarette smoking hypertension or anti HPT meds low HDL family history age
 cigarette smoking hypertension or anti HPT meds low HDL family history age")
28
ATP III Guidelines - Application Step 4 – If 2+ risk factors (other than LDL) without CHD or CHD equivalent, assess 10-year CHD risk – Framingham tables > 20% = CHD risk equivalent
 without CHD or CHD equivalent, assess 10-year CHD risk – Framingham tables > 20% = CHD risk equivalent")
29
ATP III Guidelines - Application Step 5 – Determine risk category CHD or CHD Risk Equivalent 2+ Risk Factors 1-1 Risk Factors Establish LDL goal Determine need for TLC based on LDL Determine level for drug consideration

30
ATP III Guidelines - Application Step 6 – Initiate TLC if LDL is above goal TLC diet Weight management Increase physical activity

31
ATP III Guidelines - Application Step 7 – consider adding drug therapy if LDL exceeds recommended levels Drugs + TLC simultaneously if CHD or CHD equivalent Add drugs to TLC after 3 months for other risk categories

32
ATP III Guidelines - Application Step 8 – Identify metabolic syndrome and treat, if present after 3 months of TLC Clinical identification – abdominal obesity – hypertriglyceridemia – low HDL – hypertension – hyperglycemia

33
ATP III Guidelines - Application Step 8 (cont.) Treat underlying causes – weight management – physical activity Treat risk factors if they persist despite TLC – treat hypertension – use asprin – treat hypertriglyceridemia, low HDL
 Treat underlying causes – weight management – physical activity Treat risk factors if they persist despite TLC – treat hypertension – use asprin – treat hypertriglyceridemia, low HDL")
34
ATP III Guidelines - Application Step 9 – Treat elevated triglycerides primary aim is to reach LDL goals intensify weight management increase physical activity consider TG lowering drugs if TG > 500mg/dl, 1st lower TG to prevent pancreatitis (VLFD)
")
35
ATP III Guidelines - Application Step 9 (cont.) – Treatment of low HDL first reach LDL goal intensify weight management and increase physical activity consider drug treatment if TG normal
 – Treatment of low HDL first reach LDL goal intensify weight management and increase physical activity consider drug treatment if TG normal")
36
Thanks! The End!

37
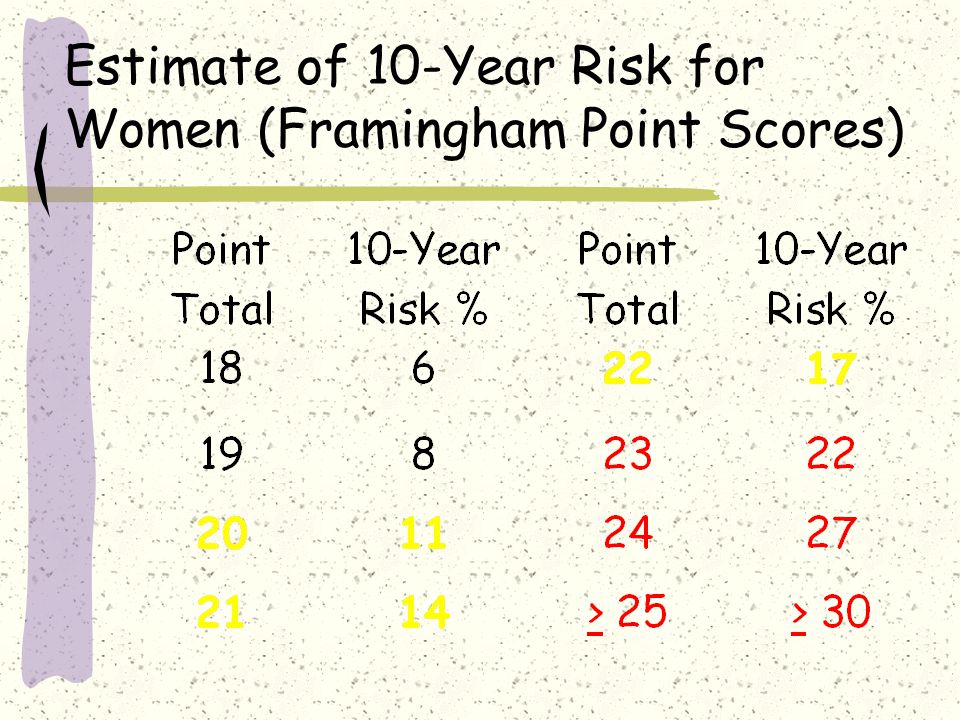
Estimate of 10-Year Risk for Women (Framingham Point Scores)
")
44
Who, me worry ???

Similar presentations










 Causes and Diagnosis Genetic disorders –Monogenic.>")





” 2004 Focus = multiple risk factor assessment.>")


 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")

![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")

 Guidelines>")
