Download presentation
Presentation is loading. Please wait.

1
DIFFUSE MALIGNANT MESOTHELIOMA GENERAL THORACIC SURGERY CHAPTER 65

2
Diffuse malignant pleural mesothelioma Uncommon and lethal cancer. Currently no standard treatment. Asbestos exposure is major risk factors. Important for thoracic surgeons to be knowledgeable about mesothilioma – Because they are often called on to make the diagnosis and to recommend treatment.

3
Epidemiology — Asbestos Asbestos belongs to the family of silicate fiber. Include two mineralogical groups: Amphibole and Serpentine.

4
Amphibole fibers Narrow and straight fibers. Migrate through the lymphatics of pulmonary parenchyma and accumulate in interstitial space and subpleural region. Crocidolite asbestos ( blue asbestos ) -- The most associate with malignant mesothelioma.
 -- The most associate with malignant mesothelioma..")
5
Serpentine fibers Large, curly shaped fiber. do Not travel beyond the major airways. Chrysotile ( white asbestos, the only member of Serpentin ) -- More associate with lung cancer.
 -- More associate with lung cancer..")
6
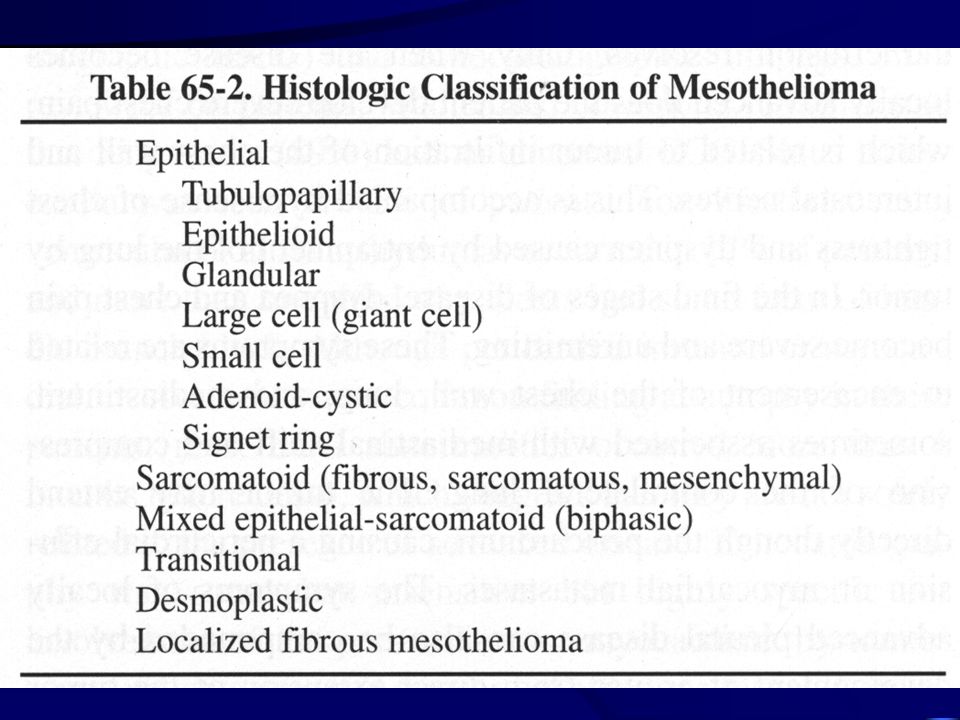
Diffuse malignant pleural mesothelioma Peak age—6 th decade. Men. Long latency period ( at least 20 years ). Incidence—men 15/million, women 3/million. Histology—Table 65-2.
. Incidence—men 15/million, women 3/million. Histology—Table")
8
Clinical presentation Nonspecific, Chest pain, dyspnea, pleural effusion, pericardial effusion, weight loss, cough, anorexia, weakness, fever, hemoptysis. Horner’s syndrome. Spontaneous pneumothorax.

9
Clinical presentation Abnormal ECG– Sinus tachycardia (42%). Echocardiographic findings. No specific tumor marker. Rise serum hyaluronan. CA-125 (20%).
..")
10
Radiographic appearance Chest-x ray— Variable and related to stage of tumor. Large pleural effusion, pleural thickening, pleural- based mass. Encasement of lung and obliteration of pleural space. Involve pericardium and pericardial effusion. Chest wall invasion, invasion through diaphragm. CT— Most accurate noninvasive way to stage. PET scan.

11
Diagnosis Thoracentesis, cytology ( positive rate 30-50% ). Percutaneous pleural biopsy. Thoracoscopy. Open pleural biopsy. AVOID Exploratory thoracotomy. Bronchoscopy. Meidastinoscopy. Bone scans.

12
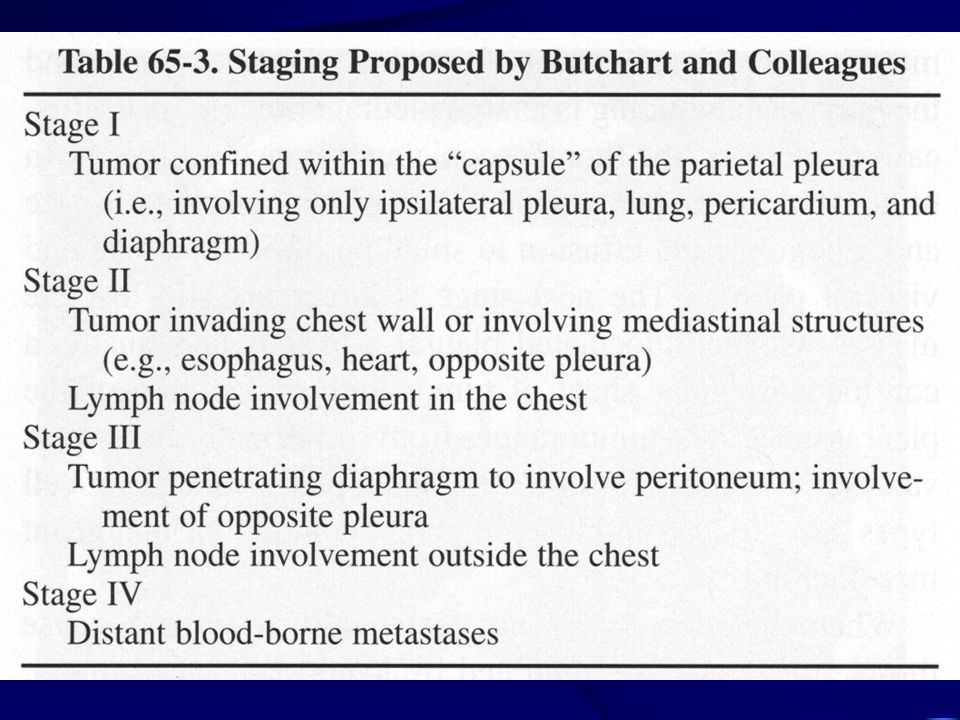
Staging Not an accurate, universally accepted staging system. Butchart (1976). Table 65-3. TNM system. Table 65-4. Liver is the most common site of distal metastasis, the contralateral lung is second.
. Table TNM system. Table Liver is the most common site of distal metastasis, the contralateral lung is second..")
15
Treatment Patient with malignant mesothelioma face a dual problem— Control of the locoregional tumor throughout the course of their disease, prevention of distant metastases as late manifestation of their cancer. Choice of treatment – Location and extent of he tumor, the general medical condition of patient. Surgery, radiation, chemotherapy, immunotherapy, supportive care.

16
Radiation therapy Difficult to evaluate the success of radiation therapy as the only treatment. Usually given in conjunction with surgical resection or chemotherapy. Limited by the volume of primary tumor that invole entire hemithorax, proximity of the tumor to many vital structures that intolerant high doses of radiation. 4500 cGy. Adjuvant treatment after surgical resection of gross tumor.

17
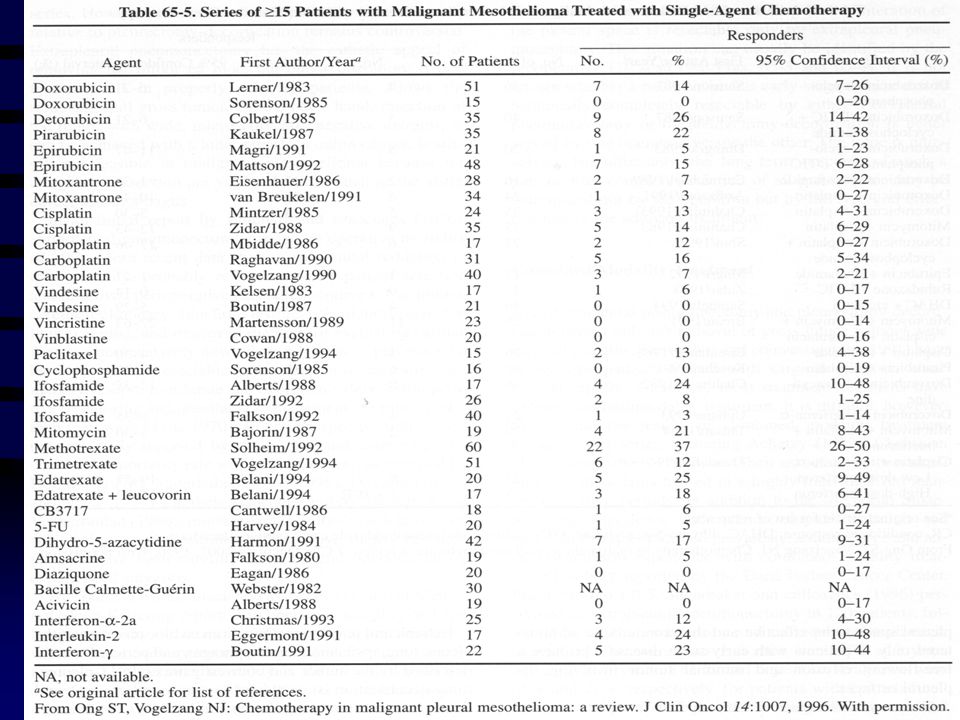
Chemotherapy Table 65-5. Combination treatment. Table 65-6. Response rate 30-40%

20
Immunotherapy Interferon– As antiproliferative effect on mesothelioma cell line. Human interferon-α-2a combined with mitomycin C. Interferon-γ – As an intrapleural treatment in early-stage diaseas ( 40x106U infused into pleural space twice weekly for 2 months ), 56% response. Intrapleural interleukin 2.
, 56% response. Intrapleural interleukin 2..")
21
Intrapleural gene therapy Herpessimplex virus thymidine kinase ( HSVtk ) gene– Transfer to tumor via adenovirus. Administration of antiviral drug– Ganciclovir– Led the tumor death.

22
Surgery Still the mainstay of treatment. Three operation– (1). Extrapleural pneumonectomy. ( pleuropneumonectomy ) (2). Pleurectomy-decortication. (3). Palliative limited pleurectomy.
 (2). Pleurectomy-decortication. (3). Palliative limited pleurectomy..")
23
Extrapleural pneumonectomy En bloc resection of pleura, lung, ipsilateral hemidiaphragm, pericardium, Value– Controversial. Operative mortality 6- 30%. Preoperative CT, lung function, ventilation- perfusion scan, cardiac function evaluate.

24
Pleurectomy-decortication Remove all gross pleural disease, without removing underlying lung. Also remove hemidiaphragm and pericardium.

25
Palliative limited pleurectomy Resection parietal pleura to control pleural effusion. Thoracoscopy and talc poudrage — High effective in controlling effusion.

Similar presentations