Download presentation
Presentation is loading. Please wait.

1
TECHNIQUE OF PLEURAL PNEUMONECTOMY IN DIFFUSE MESOTHELIOMA GENERAL THORACIC SURGERY CHAPTER 66

2
Extrapleural pneumonectomy Improvement in operative mortality since 1970 ( 30% to 6% ). Patient selection, preoperative preparation, intraoperative management, postoperative care with this extremely complex disease.

3
Staging Use the Butchart staging system— Surgical resection only appropriate for stage I disease. Brigham stage I and II as potentially respectable. Table 66-2.

5
Patient selection Karnofsky performance status higher than 70. Normal liver and liver function, ABG – Room air PCO 2 less than 45 mmHg, PO 2 more than 65 mmHg. Lung function and ventilation–perfusion scan normal. Echocardiography, CT and MRI– For determine the presence of transdiaphragmatic extention or mediastinal invasion.

6
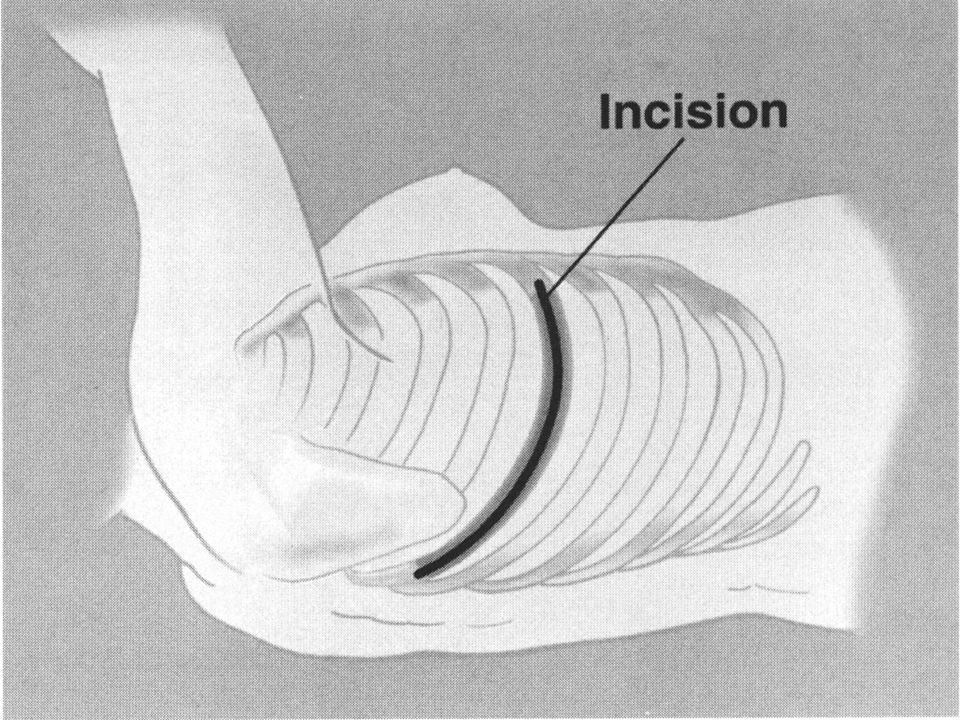
Technique of right side extrapleural pneumonectomy Before thoracotomy, limited subcostal incision– Explore the possible transdiaphragmatic involvement. (May laparoscopic exploration). If peritoneal invasion, the thoracotomy should be terminated. Left lateral decubitus position, extended right posterolateral thoracotomy, N.G. tube.
. If peritoneal invasion, the thoracotomy should be terminated. Left lateral decubitus position, extended right posterolateral thoracotomy, N.G. tube..")
7
Technique of right side extrapleural pneumonectomy Sixth ribs is excised. Widely based extrapleural blunt and sharp dissection. Superiorly toward the apex and anterior component. Posterior latterly after adequate exposure of anterior side which can provide safe view of mediastinal structure.

8
Technique of right side extrapleural pneumonectomy Brachial triangle is exposed carefully– To avoid avulsion of subclavian artery and vein Protected internal mammary artery. Open pericardium with resection posterior to hilum. Diaphragm is dissected off the peritoneum by blunt dissection using sponge stick.

9
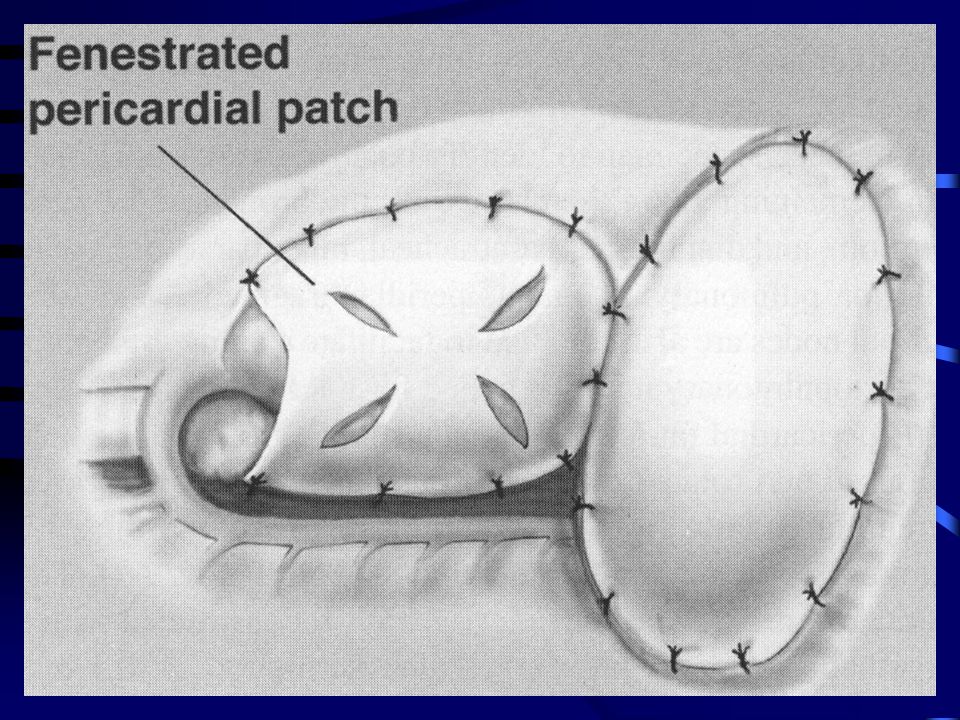
Technique of right side extrapleural pneumonectomy Ligated the right main pulmonary artery, superior and interior pulmonary vein, right main stem bronchus. Pericardial fat-pad– Cover the cutting end of bronchus. Radical lymph node dissection. Right side pericardium is reconstructed by prothetic patch to prevent cardiac herniation. Diaphragm reconstructed by prosthetic impermeable patch.

10
Technique of left side extrapleural pneumonectomy Dissection is less difficult. Dissection the posteromedial aspect – Should entering correct plane in preaortic region – To prevent avulsion intercostals vessels. Assessment of aorta is critical step on left side pleuropneumonectomy. Protect esophagus. Pericardium is NOT routinely reconstructed– Because of risk of cardiac herniation is low.

11
Technique of extrapleural pneumonectomy Hemostasis— Intra-operative blood loss 750 for right side and 500 for left side. Use argon beam coagulator and electrocautery for the numerous small vessels in extrapleural plane.

12
Postoperative management Control pain. Minimize intravascular volume change ( 1- L, 24hour fluid restriction for 3-5 days ). DVT prophylaxis. Bed rest 48 hours– To facilitate mediastinal stability.
. DVT prophylaxis. Bed rest 48 hours– To facilitate mediastinal stability..")
13
Result Mortality 3.8% ( 1999 ). 2-year survival – 38%. 5-year survival – 15%.
. 2-year survival – 38%. 5-year survival – 15%.")
Similar presentations