Download presentation
Presentation is loading. Please wait.

1
Osteoarthritis Typically affects the fingers, spine, hips and knees

2
BY INT. KAMOLWAN INT. KAMOLWAN

3
OA KNEE Chronic, degenerative disorder of multifactorial aetiology, characterised by loss of articular cartilage and periarticular bone remodelling, particularly large weight-bearing joints Common in older patients but can occur in younger patients ( genetic mechanism, previous joint trauma )
")
4
Pathophysiology Degenerative alterations primarily begin in the articular cartilage External forces accelerate the catabolic effects of the chondrocytes and disrupt the cartilaginous matrix Enzymatic destruction increases cartilage degradation ↓ proteoglycans and collagen synthesis Decreased strength of the cartilage is compounded by adverse alterations of the collagen Reduced contact area of the cartilage

5
Pathophysiology Loss of cartilage results in the loss of the joint space Progressive erosion of the damaged cartilage occurs until the underlying bone is exposed Subchondral bone responds with vascular invasion and increased cellularity, at areas of pressure

6
Pathophysiology The traumatized subchondral bone may undergo cystic degeneration At nonpressure areas along the articular margin → irregular outgrowth of new bone (osteophytes)
")
8
Normal joint hinge joint formed

9
Surface layer of cartilage break down and wears away,causes the bones under the cartilage to rub together Pain, swelling, and loss of motion result formation of bone spurs

10
Incidence Incidence increases with age USA approximately 80-90% of individuals older than 65 years have evidence of primary osteoarthritis After age 55 years, the prevalence increases in women in comparison with men

11
Incidence Equivalent prevalence occurs in men and women aged 45-55 years (↑dramatically after the age of 50 years) Most adults older than 55 years show radiographic evidence of osteoarthritis No significant correlation exists between incidence of OA and race
 Most adults older than 55 years show radiographic evidence of osteoarthritis No significant correlation exists between incidence of OA and race")
12
Causes Primary OA Idiopathic Defective gene

13
Causes Secondary OA –Obesity –Repetitive use (ie, jobs requiring heavy labor and bending) –Previous trauma (ie, posttraumatic OA) –Infection
 –Previous trauma (ie, posttraumatic OA) –Infection")
14
Causes –Crystal deposition –Acromegaly –Previous rheumatoid arthritis (ie, burnt-out rheumatoid arthritis) –Heritable metabolic causes (eg, alkaptonuria, hemochromatosis, Wilson disease)
 –Heritable metabolic causes (eg, alkaptonuria, hemochromatosis, Wilson disease)")
15
Causes –Hemoglobinopathies (eg, sickle cell disease, thalassemia) –Underlying orthopedic disorders (eg, congenital hip dislocation, slipped femoral capital epiphysis) –Disorders of bone (eg, Paget disease, avascular necrosis)
 –Underlying orthopedic disorders (eg, congenital hip dislocation, slipped femoral capital epiphysis) –Disorders of bone (eg, Paget disease, avascular necrosis)")
16
History Insidious throbbing arthralgias with activity Initially, resting relieves the pain Eventually, the pain occurs even at rest Morning stiffness ≥ 30 minutes Intermittent joint swelling

17
Symptoms Pain Stiffness Gelling Instability

18
Signs Pain Tenderness Swelling Effusion Crepitus Limitation of movement and muscle wasting

19
Physical Early –Joints may appear normal –Gait may be antalgic if weight-bearing joints are involved

20
Physical Later –Visible osteophytes may be noted –Joints may be warm to palpation –Palpable osteophytes frequently are noted –Joint effusion frequently is evidenced in superficial joints

21
Physical –Range-of-motion limitations, because of bony restrictions and/or soft tissue contractures, are characteristic –Crepitus with range of motion is not uncommon

23
Imaging Plain radiographs Bone scans may be helpful in early diagnosis of OA of the hand

24
The space between the bones of the upper and lower leg is smaller Bony spurs (osteophytes) Increase bone density at the margin of the joint
 Increase bone density at the margin of the joint")
25
x-ray findings –Joint space narrowing –Osteophytes –Subchondral sclerosis : ↑ bone density, frequently found adjacent to joint space –Subchondral cysts : fluid-filled sacs which extrude from the joint

26
Diagnosis On the basis of the initial history and examination X-rays

27
PROGRESS Osteoarthritis begins when the joint cartilage starts to become worn down → decreases the ability of the cartilage to work as a shock-absorber to reduce the impact of stress on the joints The remaining cartilage wears down faster → bones to grind against one another Bone spurs may form

28
Treatment

29
Goals of managing OA Controlling pain Maintaining and improving the range of movement and stability of affected joints Limiting functional impairment

30
Treatment Education and behavioural intervention - Aim is to provide patients with an understanding of the disease process, its prognosis and the rationale and implications of managing their condition Weight loss - Weight loss (< 5 kg) has significant short- term and long-term reduction in symptoms of OA
 has significant short- term and long-term reduction in symptoms of OA")
31
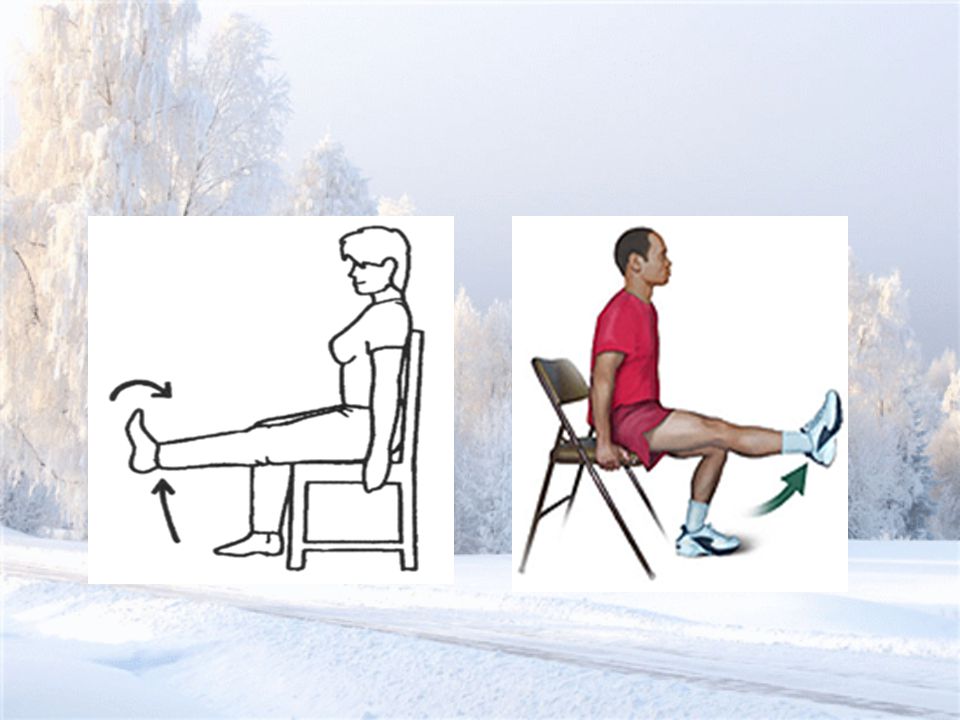
Treatment Mechanical aids - Wear shock-absorbing footwear with good mediolateral support, adequate arch support and calcaneal cushion Exercise -Aim of exercise is to reduce pain and disability by strengthening muscle, improving joint stability, increasing the range of movement and improving aerobic fitness

34
Treatment Medication - Acetaminophen (Tylenol®) is a mild pain reliever with few side effects -Anti-inflammatory medication, such as ibuprofen and aspirin -COX-2 inhibitors -Glucosamine and Chondroitin sulfate
 is a mild pain reliever with few side effects -Anti-inflammatory medication, such as ibuprofen and aspirin -COX-2 inhibitors -Glucosamine and Chondroitin sulfate")
35
Treatment Intra-articular injection - Glucocorticoids injection - Hyaluronic Acid (HA) and similar hyaluronan preparations (eg, Synvisc)
 and similar hyaluronan preparations (eg, Synvisc)")
36
Treatment Surgery -Arthroscopy (including debridement,and lavage/irrigation) -Proximal Tibial Osteotomy -Artificial Knee Replacement -Osteotomy -Arthroplasty or Joint Replacement
 -Proximal Tibial Osteotomy -Artificial Knee Replacement -Osteotomy -Arthroplasty or Joint Replacement")
Similar presentations






 Primary Joint Classifications Functional NameStructural NameDegree of Movement Example SynarthrosesFibrousImmovableSutures.>")

 OA is the most common form of arthritis and the most common joint disease Over 10 million Americans suffer from OA.>")






 is one of the oldest and most common forms of arthritis. Known as the “wear and tear” kind of arthritis.>")






. Topics to be covered in this lecture: Arthritis–arthrosis Fibromyalgia and myofascial pain syndrome Osteoporosis Fractures–post-traumatic.>")