Download presentation
Presentation is loading. Please wait.

3
Physician Multidisciplinary Discharge Routine Training Guide June 2015

5
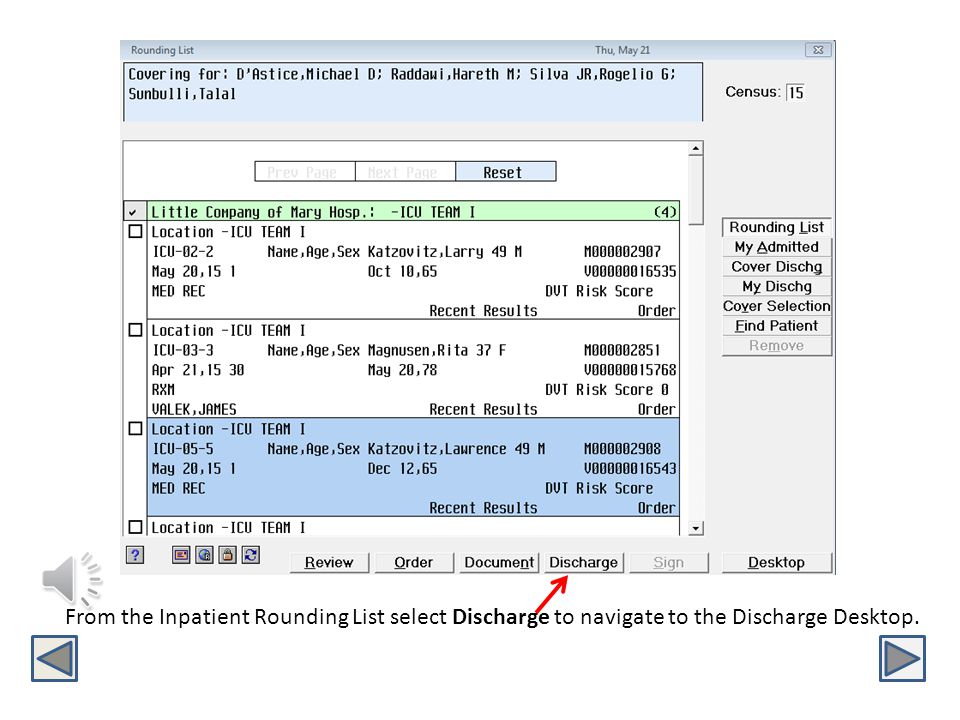
From the Inpatient Rounding List select Discharge to navigate to the Discharge Desktop.

7
Manage Patient Problems Create Discharge Orders Document Discharge Instructions Create Referrals to Providers and Community Resources Update and Reconcile Medications Physician Discharge Desktop

9
ADDING AND MANAGING PROBLEMS

11
Managing the Problem List 1.Select Discharge from Clinical Review or the Online Rounding List 2.Click blue EDIT box next to Patient Problems

13
Adding a Problem Start Typing patient problem by name(choices will begin appearing), or Click ICD Code button and start typing desired code. Name ICD 9

15
CREATING A DISCHARGE ORDER

17
1. Click Blue ADD Order button 1 2. Select appropriate Discharge Order 2

19
Follow current process to complete Discharge Order. Referrals should be entered in the Follow Up/Referral box

21
Capture of National Quality Measure Data If “yes” is selected on the second page of the Discharge Order, confirming this is stroke or AMI patient, these therapy questions will be answered. Click Ok to submit Discharge Order

23
CREATING DISCHARGE INSTRUCTIONS

25
1. Click Blue ADD PDoc button 1 2. Select appropriate PDoc template 2

27
Document free text entries for Hospital Course and Instructions. Instructions entered on this screen will carryover to the instructions on the Discharge Order.

29
Submitting and Signing PDoc 1.Select Submit 2.Select Signed

31
DISCHARGE MEDICATION RECONCILIATION

33
On the former paper medication reconciliation process, Home Meds and Inpatient Meds were displayed side by side on the Discharge Med Rec document. The updated electronic format will display as follows: Inpatient Medication will display first in blue Home Meds will display under the Inpatient Medication in black Medications ordered after the admission medication reconciliation appear only once in blue during the discharge medication reconciliation process. Inpatient Home New Inpt.

35
To begin Discharge medication reconciliation select the red Edit button next to Medications.

37
1.Choose Continue (CONT) or Stop on the Home Medications (black entries) 2.If continuing an Inpatient medication (blue entries): a) Stop the home medication b) Select Convert (CONV) to continue the medication at home 3. Select Submit to save the medication reconciliation 3

39
Converting an Inpatient Medication to a Home Medication Converted Inpatient Medications require the following entries: Line 1 - Dose, Units, Route, Frequency, and Reason for Use Line 2 – Quantity or Days Select Done

41
Multiple physicians can act on a patient’s medication reconciliation. Submitting a partially completed medication reconciliation will generate this message. l Select “Yes” to leave some medications unreconciled. a) unsure of the home status of a medication at this time b) waiting for another physician to act on medication c) will complete reconciliation at a later time Select “No” to return to the medication reconciliation screen. ALL Home Medications must be addressed prior to discharge.
 unsure of the home status of a medication at this time b) waiting for another physician to act on medication c) will complete reconciliation at a later time Select No to return to the medication reconciliation screen. ALL Home Medications must be addressed prior to discharge..")
43
Completed Discharge Medication Reconciliation Medications EDIT button changes from Red to Blue, signifying all Home Medications have been acted upon. Medications are listed by actions taken: New Prescriptions, Continued, and Stopped.

Similar presentations



































 Bathrooms Exits Q&A Format.>")



