Download presentation
Presentation is loading. Please wait.

1
Dr. Maha Al-Sedik

3
Why do we study respiratory emergency? Respiratory Calls are some of the most Common calls you will see. Respiratory care is as essential as the ABC’s Mishandling a respiratory call can be fatal.

5
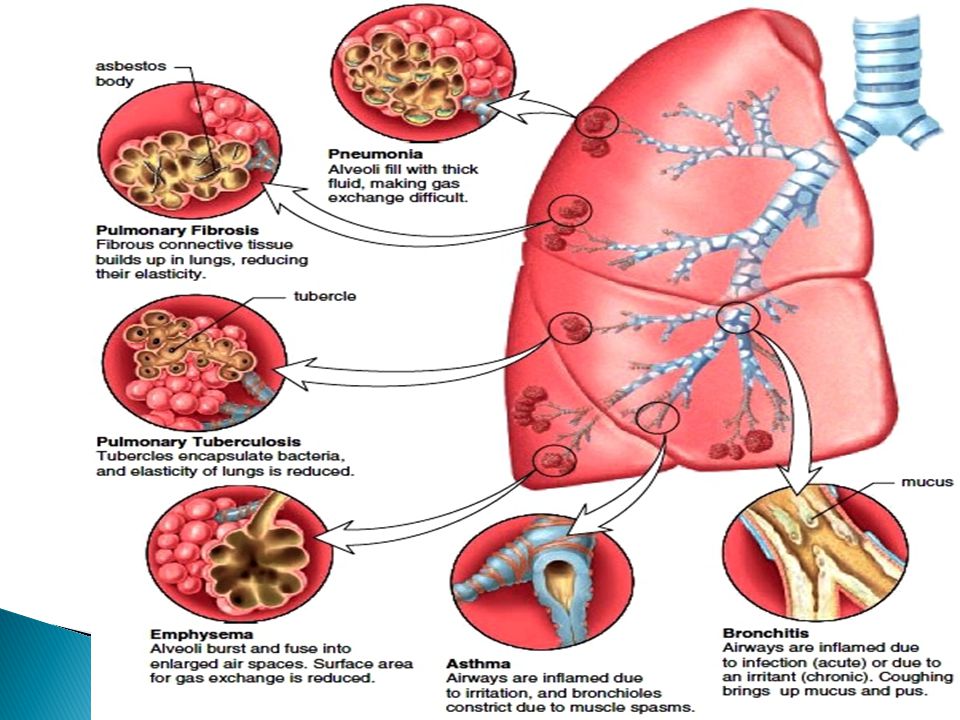
Infectious diseases may affect all parts of the airway. The problem is some form of obstruction to the air flow or the exchange of gases. Upper or Lower Airway Infection

6
Examples: Bronchitis Common cold Diphtheria TB Pneumonia Epiglottitis Influenza

7
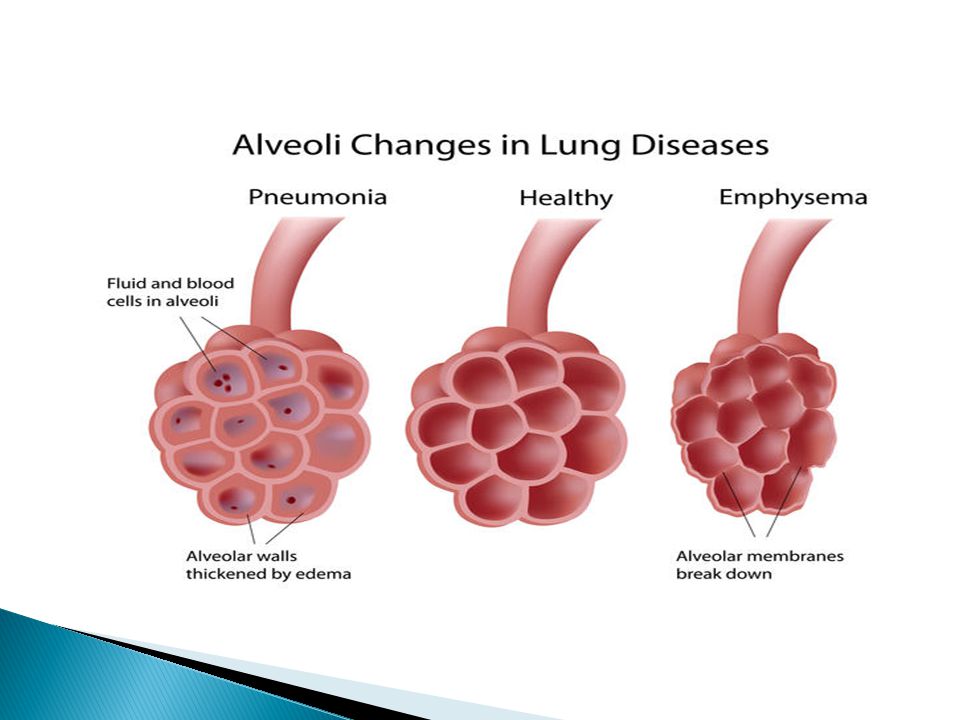
Some form of obstruction causes dyspnea: Obstruction to flow of air in major passages: Colds, diphtheria, epiglottitis. Obstruction to exchange of gases: Pneumonia.

10
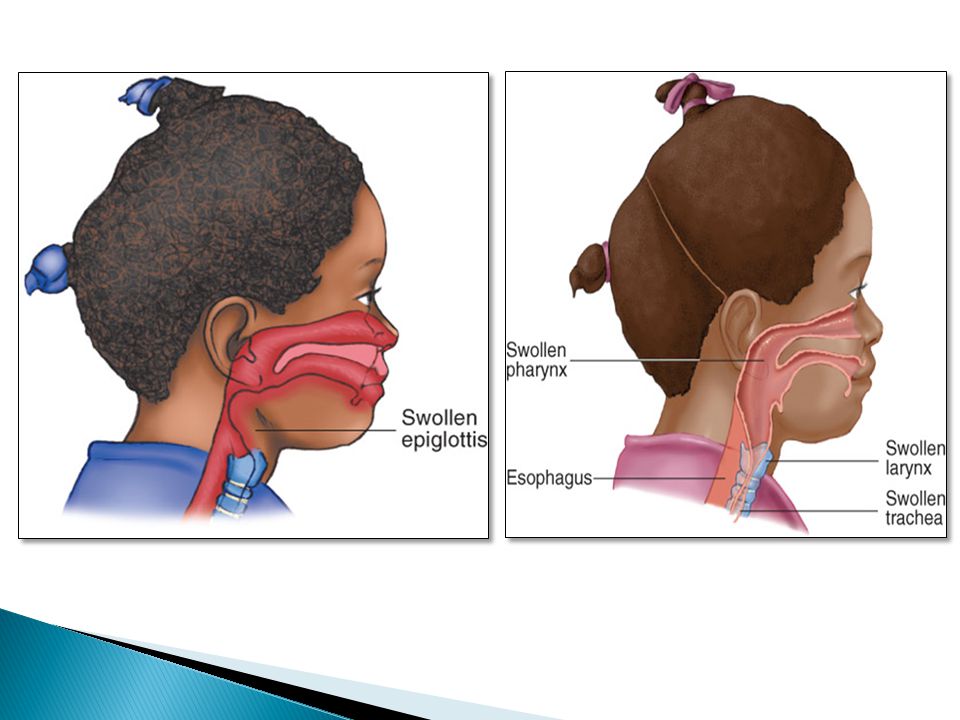
Assessment: Administer warm, humidified oxygen. Do not attempt to suction the airway or insert an oropharyngeal airway in a patient with suspected epiglottitis because this may cause a spasm and a complete airway obstruction. Transport patient in position of comfort.

11
Acute Pulmonary Edema Heart muscle can’t circulate blood properly. Fluid builds up between alveoli and capillaries. Signs and symptoms –Dyspnea –Frothy pink sputum History of chronic congestive heart failure

12
Fluid between alveolus and capillary CO 2 O2O2 Gas exchange inhibited by fluid between alveolus and capillary

13
Pathophysiology: Acute pulmonary edema occurs when an excessive amount of fluid collects in the spaces between the alveoli and the capillaries. This fluid disturbs normal gas exchange by reducing the ability of oxygen and carbon dioxide to diffuse across the alveolar-capillary surface. This leads to hypoxia.

15
Assessment: Place the patient in a position of comfort, usually sitting up. Administer high-flow oxygen. Provide ventilatory support.

16
Obstructive Pulmonary Disease Obstructive Pulmonary Disease A call for a patient complaining of shortness of breath who has an obstructive pulmonary (lung) disease is common in the pre-hospital environment. An obstructive lung disease Obstruction of airflow through the respiratory tract Reduction in gas exchange hypoxia

17
Chronic Obstructive Pulmonary Disease (COPD) A call for a patient complaining of shortness of breath who has an obstructive pulmonary (lung) disease is common in the pre-hospital environment. An obstructive lung disease obstruction of airflow through the respiratory tract reduction in gas exchange hypoxia

18
The two most commonly obstructive pulmonary diseases: emphysema chronic bronchitis Many patients have a combination of chronic bronchitis and emphysema and present with a mixture of signs and symptoms associated with both conditions.

20
Hypoxic drive: Normally, the amount of carbon dioxide in the blood is the primary stimulus for breathing. A secondary stimulus for breathing is hypoxia, a decrease in oxygen. COPD patients whose expirations are so inefficient that their bodies have become accustomed to higher than normal levels of co 2. So hypoxic drive is a condition in which the body's stimulus for taking a breath is low oxygen. Occurs in people with COPD.

22
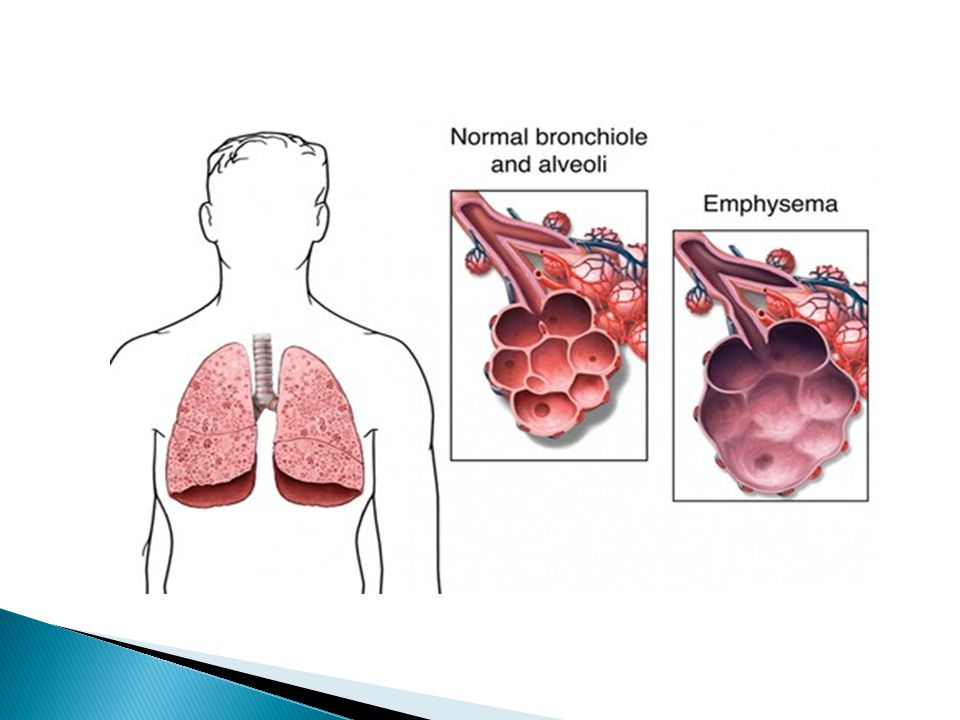
Emphysema More common with smokers. Emphysema is a permanent disease that is characterized by destruction of the alveolar walls and distention of the alveolar sacs. Severe reduction in the alveolar/capillary area for gas exchange to occur.

25
Pathophysiology: In emphysema, the lung tissue loses its elasticity, the alveoli become distended with trapped air, and the walls of the alveoli are destroyed. Loss of the alveolar wall reduces the surface area in contact with pulmonary capillaries. Decrease in gas exchange occurs. The patient becomes progressively hypoxic and begins to retain carbon dioxide.

27
Exhaling becomes an active rather than a passive process, requiring muscular contraction; therefore, the patient uses most of his energy to breathe.

28
Assessment: Dyspneic Thin, barrel-chest appearance from chronic air trapping in the alveoli causing the anterior– posterior diameter of the chest to increase

29
Prolonged exhalation Pursed-lip breathing (physiologic PEEP) Diminished breath sounds Wheezing and rhonchi on auscultation Extreme difficulty of breathing on minimal exertion Pink puffer (extra hemoglobin to make up for poor oxygen pick up). Tachypnea: breathing rate usually greater than 20 per minute at rest. Tachycardia (increased heart rate).
..")
30
Pursed-lip breathing

32
Management: Ensuring an open airway position of comfort Administration of supplemental oxygen

33
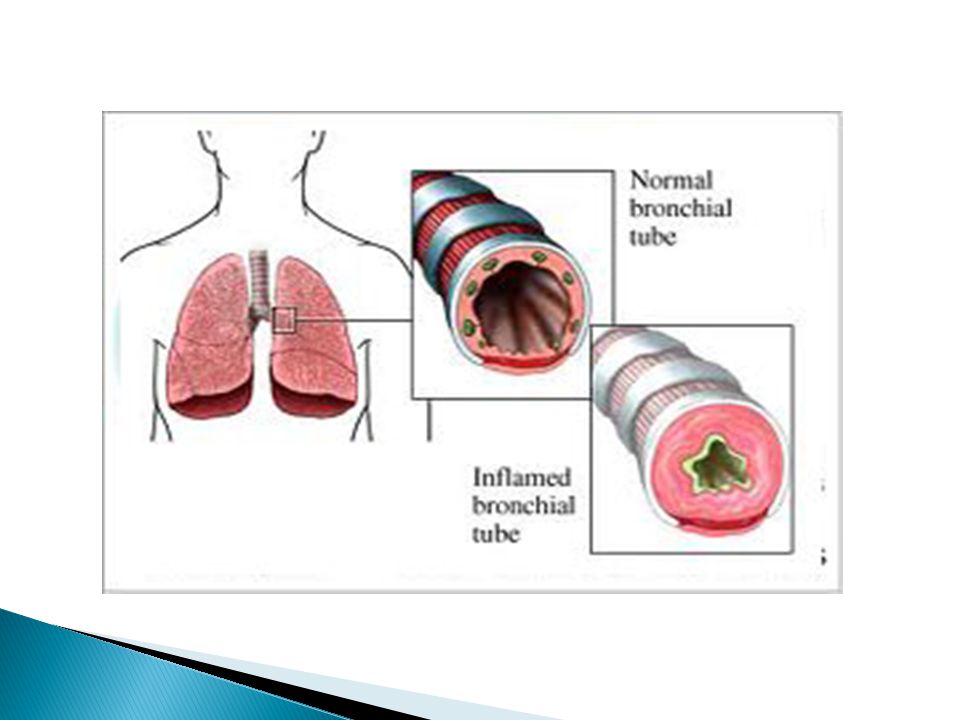
Chronic Bronchitis Increased mucus production. Decreased alveolar ventilation. Underlying problem: Ventilation and inflammation.

34
Pathophysiology: Chronic bronchitis involves inflammation, swelling, and thickening of the lining of the bronchi and bronchioles and excessive mucus production. The alveoli remain unaffected by the disease. The airways become very narrow, causing a high resistance to air movement and chronic difficulty in breathing.

35
Obstructive Pulmonary Disease Obstructive Pulmonary Disease An obstructive lung disease Obstruction of airflow through the respiratory tract Reduction in gas exchange hypoxia

37
Assessment: Cough (hallmark sign) is prominent; with sputum Cyanosis ( so it was called “blue bloaters” ) Minimal difficulty in breathing and anxiety. Wheezes and, possibly, crackles at the bases of the lungs

39
Secure airway Correct hypoxia Albuterol bronchodilation if wheezing Management

Similar presentations












 into the atmosphere Filter, moisten,>")














