Download presentation
Presentation is loading. Please wait.

1
Guidelines in the Management of RA Haya M. Al-Malaq Lecturer, Clinical Pharmacy Dept. Clinical Pharmacist Rheumatology Haya_malak@yahoo.com

2
Outlines Introduction Epidemiology Pathopysiology S & S Management

3
Introduction Rheumatoid arthritis (RA) is an autoimmunedisorder of unknown etiology characterized by symmetric, erosive synovitis and, in some cases, extraarticular involvement. Most patients experience a chronic fluctuating course of disease that, despite therapy, may result in progressive joint destruction, deformity, disability, & even premature death.

4
Epidemiology RA results in more than 9 million physician visits and more than 250,000 hospitalizations per year. Disability from RA causes major economic loss and can have a profound impact on families. RA affects 1% of the adult population this is due to low diagnosis (difficult to diagnose in early stages).
..")
5
Pathophysiology

6
The cause of RA is still unknown, it could be infection & as the case of other autoimmune diseases the immune system (AB to organism) begins to attack its self (molecules in the synovium that looks like the offending organism) Some infectious organisms mentioned in this context have been Mycoplasma, Erysipelothrix, parvovirus B19 and rubella, EBV, human herpes virus.
 begins to attack its self (molecules in the synovium that looks like the offending organism) Some infectious organisms mentioned in this context have been Mycoplasma, Erysipelothrix, parvovirus B19 and rubella, EBV, human herpes virus.")
7
Pathophysiology Genetic predisposition is important, risk factors include cigarette smoking, hormonal factors (more in women). Once triggered, B lymphocytes produce immunoglobins, & RF of the IgG & IgM classes that are deposited in the tissue, this subsequently leads to the activation of the serum complement cascade & recruitment of the phagocytic arm of the immune response, which further exacerbates the inflammation of the synovium, leading to edema, vasodilation and infiltration by activated T-cells

8
Pathophysiology Early and intermediate molecular mediators of inflammation include TNF-α, IL-1,6,8,15, transforming growth factor beta, fibroblast growth factor and platelet-derived growth factor. Synovial macrophages and dendritic cells further function as antigen presenting cells by expressing MHC class II molecules, leading to an established local immune reaction in the tissue.

9
Pathophysiology The disease progresses in concert with formation of granulation tissue at the edges of the synovial lining (pannus) with extensive angiogenesis and production of enzymes that cause tissue damage. Once the inflammatory reaction is established, the synovium thickens, the cartilage and the underlying bone begins to disintegrate and evidence of joint destruction accrues.

11
S & S

12
Synovitis Most commonly affected joints are, small joints (including the hands, feet and cervical spine), but larger joints (shoulders, knees etc) can also be involved; the pattern of joint involvement can differ from patient to patient. Inflammation in the joints manifests itself as a soft, "doughy" swelling, pain, tenderness to palpation and movement, local warmth, and functional impairment. Morning stiffness is often a prominent feature and may last for more than an hour

13
Deformity The fingers are typically deviated towards the little finger ( ulnar deviation ) and can assume unnatural shapes. Classical deformities are the Boutonniere deformity swan neck deformity The thumb may develop a "Z- Thumb" deformity

15
Extra-articular general tiredness and lassitude, low-grade fever, elevated ESR, and anemia. GI bleeding as a side effect of drugs used in treatment, especially NSAIDs. Extra-articular manifestations occur in about 15% of patients Hepatosplenomegaly which may occur with concurrent leukopenia and is then referred to as Felty's syndrome,. lymphocytic infiltration affecting the salivary &lacrimal glands (Sjögren's syndrome). pericarditis, pleurisy, alveolitis, scleritis, and subcutaneous nodules.
. pericarditis, pleurisy, alveolitis, scleritis, and subcutaneous nodules..")
16
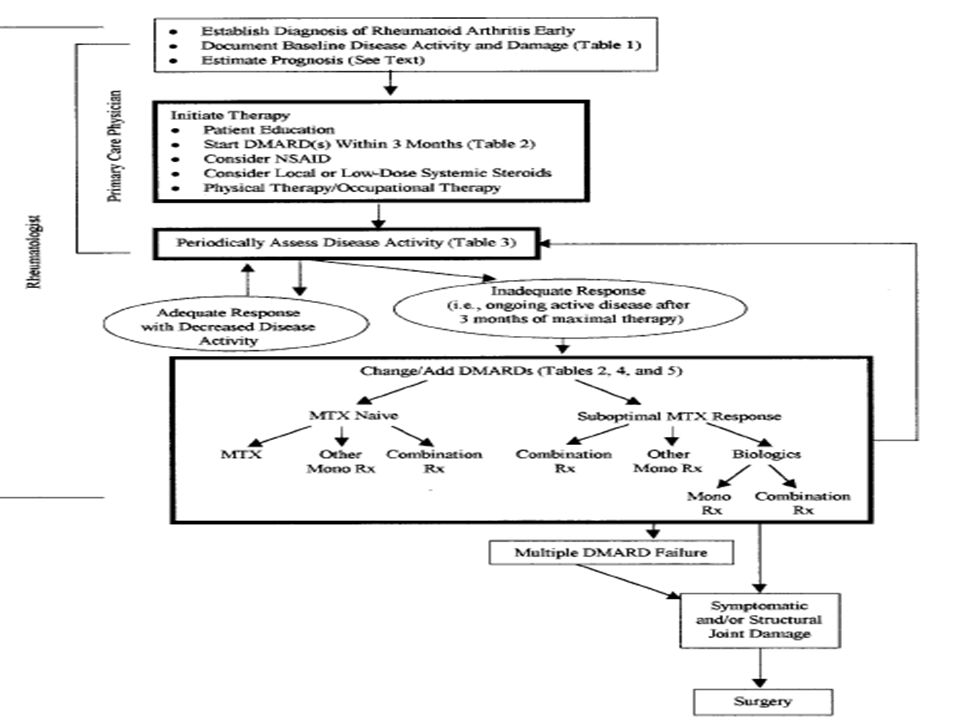
Management

18
1-Diagnosis

19
Diagnostic Criteria The ACR has defined the following criteria (>4) for the classification of RA: Morning stiffness of >1 hour most mornings for at least 6 weeks. Arthritis and soft-tissue swelling of >3 of 14 joints/joint groups, present for at least 6 weeks Arthritis of hand joints, present for at least 6 weeks Symmetric arthritis, present for at least 6 weeks Subcutaneous nodules in specific places Rheumatoid factor at a level above the 95th percentile Radiological changes suggestive of joint erosion

20
Blood Test RF (patients can be seronegative RA), not very specific test, 80% -ve in the 1 st yr. anti-citrullinated protein antibodies (ACPA), more specific, can detect pt in early stages or even before occurrence of the disease. ESR, CRP, CBC, RF, liver enzyme, ANA, Ferritin can reveal hemochromatosis.
, more specific, can detect pt in early stages or even before occurrence of the disease. ESR, CRP, CBC, RF, liver enzyme, ANA, Ferritin can reveal hemochromatosis..")
21
2-Document baseline disease activity & damage

23
3-Prognosis

24
Prognosis Selection of the treatment regimen requires a assessment of prognosis. Poor prognosis is suggested by earlier age at disease onset, high titer of RF, elevated ESR, and swelling of 20 joints. Extraarticular manifestations of RA may also indicate poor prognosis.

25
Prognosis Studies have shown that patients with active, polyarticular, RF- positive RA have a 70% probability of developing joint damage or erosions within 2 years of the onset of disease

26
Assessment of Disease Activity

27
4-Initial therapy

28
Goals of Management RA are to preventor control joint damage by inducing complete remission. Prevent loss of function. Decrease pain. Maximize the QOL.

29
Complete Remission Is Absence of: 1) symptoms of active inflammatory joint pain 2) morning stiffness 3) fatigue, 4) synovitis on joint examination 5) progression of radiographic damage on sequential radiographs 6)elevation of ESR or CRP levels
 symptoms of active inflammatory joint pain 2) morning stiffness 3) fatigue, 4) synovitis on joint examination 5) progression of radiographic damage on sequential radiographs 6)elevation of ESR or CRP levels")
30
Patient education It is a chronic disease. Risks of joint damage and loss of Reviewing the risks and benefits of existing treatment modalities. Periods of rest, job modification, time off from work, changes in occupation, or termination of work may be necessary

31
Patient education Surgery Longitudinal treatment plan Treatment options Cost Adverse effects Expected time of response

32
Non-Pharmacological Tx Patient education. Instruction in joint protection, conservation of energy, home program of joint range of motion strengthening exercises Regular participation in dynamic and even aerobic conditioning exercise programs

33
Pharmacological Therapy

34
General Guidelines NSAIDs, glucocorticoid joint injection, and/or low-dose prednisone may be considered for control of symptoms. The majority of patients with newly diagnosed RA should be started on DMARD therapy within 3 months of diagnosis.

35
General Guidelines DMARD control not cure so periodic assessment is required for efficacy & SE & therapy modification. If disease activity is confined to one or a few joints, then local glucocorticoid injection may help. For patients with severe symptoms, systemic glucocorticoids may need to be initiated, or the dosage may need to be increased, for a short period of time. Try to avoid narcotic addiction.

36
Common DMARD

37
General Guidelines Pharmacologic therapy for RA often consists of combinations of NSAIDs, DMARDs, and/or glucocorticoids.

38
NSAIDs These agents have analgesic and antiinflammatory properties but do not alter the course of the disease or prevent joint destruction, so not used alone. Choice of available agents is based on considerations of efficacy, safety, convenience, and cost. Selective vr non-selective, no difference, cost.

39
Risk factors for NSADs SE advanced age. history of ulcer. concomitant use of corticosteroids or anticoagulants higher dosage of NSAID use of multiple NSAIDs serious underlying disease

40
Approaches to reduce SE use of low-dose prednisone instead of an NSAID, use of a nonacetylated salicylate, use of a highly selective COX-2 inhibitor, or use of a combination of an NSAID and a gastroprotective agent as: H2 blocker, PPI, PG analogue

41
DMARDs hydroxychlor oquine (HCQ), sulfasalazine (SSZ), methotrexate (MTX), leflunomide etanercept infliximab. azathioprine (AZA) D-penicillamine (D-Pen) gold salts minocycline cyclosporine.
 D-penicillamine (D-Pen) gold salts minocycline cyclosporine..")
42
Many factors influence the choice of DMARD relative efficacy Convenience of administration, requirements of the monitoring program, costs of the medication and monitoring time until expected benefit frequency seriousness of adverse reactions. Patient factors (compliance, diseases, prognosis, pregnancy/lactation).
..")
43
DMARDs HCQ or SSZ first, active disease or poor prognosis, MTX or combination therapy. MTX alone or in combination should be included in patient with no MTX. HCQ is indicated for milder disease, no monitoring (ophtha exam). SSZ act more quickly, start gradually, watch for leucopoenia.
. SSZ act more quickly, start gradually, watch for leucopoenia..")
44
DMARDs Most select MTX as initial therapy esp. in severely active disease, CI: liver disease, renal impairment, lung disease, or alcohol abuse, monitor liver fx, contraception is recommended. leflunomide as an alternative to MTX as monotherapy, especially for patients who cannot tolerate MTX, long t1/2, can be combined e MTX for max effect.

45
DMARDs Anti–tumor necrosis factor (anti- TNF-alpha)- biological agents etanercept and infliximab are beneficial in combination with MTX, avoid in TB, watch for infx, high cost. AZA is rarely used D-Pen is effective but its use is limited, in part, by an inconvenient dosing schedule.

46
DMARDs IM gold treatment is effective but injections are required every week for 22 weeks before less-frequent maintenance dosing is initiated, oral gold need 6 m to be effective. Tetracyclines ( minocycline), may be effective, needs more research. Cyclosporine is beneficial as monotherapy and has short-term efficacy similar to that of D-Pen. The use of cyclosporine, however, has been limited by its toxicity, HTN & renal toxicity.
, may be effective, needs more research. Cyclosporine is beneficial as monotherapy and has short-term efficacy similar to that of D-Pen. The use of cyclosporine, however, has been limited by its toxicity, HTN & renal toxicity..")
47
DMARDs Staphylococcal protein A immunoadsorption. Extracorporeal immunoadsorption of plasma against a staphylococcal protein A column was reported to be efficacious in a portion of patients with severe refractory RA. Given the difficulty and cost of administering weekly treatments for 12 weeks, the limited duration of the response, and the high frequency of side effects, this treatment should be considered only for patients with refractory RA in whom treatment with several DMARDs has failed.

48
Glucocorticoids. Low-dose oral glucocorticoids (10 mg of prednisone daily, or the equivalent) and local injections of glucocorticoids are highly effective for relieving symptoms in patients with active RA. Discuss ADRs. 1,500 mg of elemental calcium/day,400–800 IU of vitamin D/day. Hormone replacement therapy bisphosphonates
 and local injections of glucocorticoids are highly effective for relieving symptoms in patients with active RA. Discuss ADRs. 1,500 mg of elemental calcium/day,400–800 IU of vitamin D/day. Hormone replacement therapy bisphosphonates.")
49
Combination therapy Cyclosporine plus MTX MTX, HCQ, and SSZ Plus lo dose CS

50
Monitoring of common SE

Similar presentations





 Immunomodulatory and immunosuppresive Xenobiotic – Gold salts – Azathioprine – Methotrexate Biological.>")




 25 th Nov 2013.>")
? RA is an autoimmune disorder inflammation of the lining of the joints. The body.>")










