Download presentation
Presentation is loading. Please wait.

1
© 2006 Thomson-Wadsworth Chapter 8 Addressing the Obesity Epidemic: An Issue for Public Health Policy

2
© 2006 Thomson-Wadsworth Learning Objectives Define the terms obesity and overweight as they apply to adults. Define the terms overweight and at risk for overweight as they apply to children. Describe the epidemiology of obesity and overweight among adults and children.

3
© 2006 Thomson-Wadsworth Learning Objectives Explain how to assess and survey obesity and overweight in the population. List and discuss determinants of obesity and overweight. Discuss various interventions and intervention strategies for the prevention and treatment of obesity and overweight among adults and children.

4
© 2006 Thomson-Wadsworth Learning Objectives Describe potential public health strategies to prevent obesity, including examples of current and proposed policies and legislation.

5
© 2006 Thomson-Wadsworth Introduction During the past 15 years, obesity has emerged as a significant public health problem in both adults and children. Genetics and societal and environmental factors contribute to the rising number of obese individuals.

6
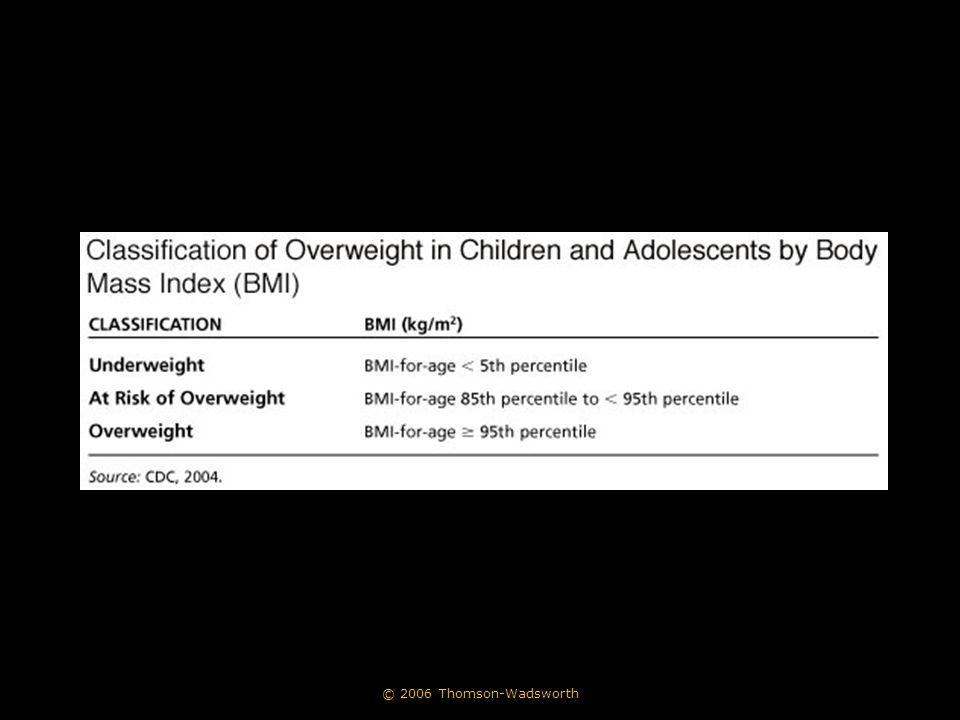
© 2006 Thomson-Wadsworth Defining Obesity and Overweight In adults, overweight is defined as a body mass index (BMI) between 25 and 29.9 whereas obesity is defined as a BMI greater than 30. In children, overweight is defined as a BMI above the CDC growth chart criterion of 95th percentile whereas at risk for overweight is defined as a BMI between the 85th and 95th percentiles.

7
© 2006 Thomson-Wadsworth

9
Epidemiology of Obesity and Overweight

10
© 2006 Thomson-Wadsworth

11
Epidemiology of Obesity and Overweight Two national surveys from which obesity data is regularly obtained: –The National Health and Nutrition Examination Study (NHANES) –Behavioral Risk Factor Surveillance System (BRFSS)
 –Behavioral Risk Factor Surveillance System (BRFSS)")
12
© 2006 Thomson-Wadsworth Epidemiology of Obesity and Overweight The Youth Risk Behavior Surveillance System (YRBSS) provides the prevalence of youth BMI by state. –The data are self-reported and limited to high school students. –Mississippi and Tennessee reported the highest rates for overweight –Utah, Wyoming, and Idaho were the lowest

13
© 2006 Thomson-Wadsworth Medical and Social Costs of Obesity The Surgeon General’s Report (2001) estimated the total economic burden of obesity to be $117 billion in 2000.
 estimated the total economic burden of obesity to be $117 billion in 2000.")
14
© 2006 Thomson-Wadsworth

15
Medical and Social Costs of Obesity Obesity is costly to society because it is associated with chronic diseases including: –Cardiovascular disease –Type 2 diabetes –Hypertension –Stroke –Dyslipidemia –Osteoarthristis

16
© 2006 Thomson-Wadsworth Medical and Social Costs of Obesity Obesity is costly to society because it is associated with chronic diseases including: –Selected cancers –Gallbladder disease –Sleep-breathing disorders –Musculoskeletal disorders

17
© 2006 Thomson-Wadsworth Medical and Social Costs of Obesity Overall quality of life is often worse with increasing obesity, and obese people experience prejudice and discrimination.

18
© 2006 Thomson-Wadsworth Determinants of Obesity Determinants of obesity can be related to either dietary intake or physical activity or both. They can be genetic, psychological, behavioral, or environmental.

19
© 2006 Thomson-Wadsworth Determinants of Obesity Referred to more frequently in the literature as causes of obesity are: –an “obesogenic” environment, or one that promotes obesity. –a “toxic environment,” or one that limits the opportunities for physical activity. Excess weight accumulation occurs with an imbalance in energy, caused by either a surplus of energy intake or lack of energy expenditure.

20
© 2006 Thomson-Wadsworth Determinants of Obesity Genetic Risk Factors Psychosocial Risk Factors –Depression –Comfort eating Behavioral Risk Factors –Caloric Intake –Types of Food Consumed –Physical Activity –Use of Television, Video Games, and Computers

21
© 2006 Thomson-Wadsworth Determinants of Obesity Environmental Risk Factors –Other Technological Innovations in Food Production and Transportation –Other Technological Changes –Portion Sizes –Eating Away from Home and Consumption of “Fast Foods” –Maternal Employment –Urban Sprawl and the Built Environment –Poverty

22
© 2006 Thomson-Wadsworth Obesity Prevention and Treatment Interventions In public health applications, interventions that address body weight are often preventive, rather than treatment, oriented. The goal of an obesity prevention program is to maintain a stable weight and not increase body size over time, in contrast to an obesity treatment program, in which the primary goal is to lose weight over time.

23
© 2006 Thomson-Wadsworth Obesity Prevention and Treatment Interventions Current recommendations for obesity treatment: –Lifestyle therapy - weight management techniques, increases in physical activity –Behavioral therapy - goal setting –Clinical therapies - pharmacotherapy, weight loss surgery

24
© 2006 Thomson-Wadsworth Obesity Prevention and Treatment Interventions Adult Interventions –Most adult-based obesity interventions have centered on clinical approaches to obesity treatment, and thus haven’t been largely successful. –Worksite health promotion programs have shown modest effects on weight in the short term.

25
© 2006 Thomson-Wadsworth Obesity Prevention and Treatment Interventions Child and Adolescent Interventions –Largely implemented in the school environment –Tended to be most effective when they included a component of decreasing television viewing

26
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Although obesity is a significant public health issue, efforts to control obesity at the public policy level in the United States are lacking.

27
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Obesity Surveillance and Monitoring Efforts

28
© 2006 Thomson-Wadsworth

29
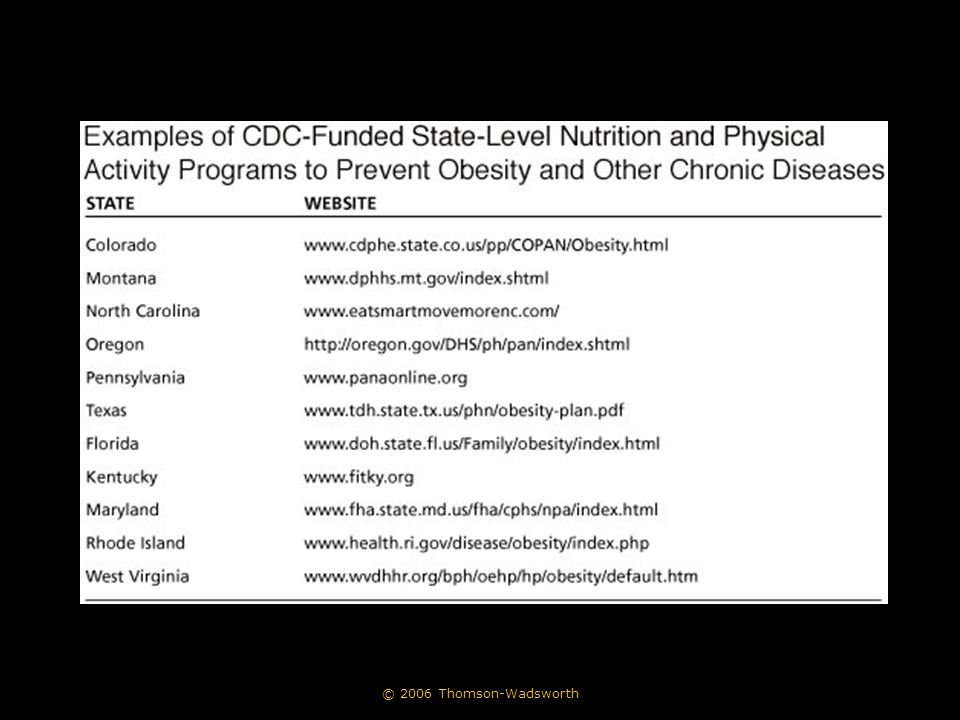
Public Health Policy Options for Addressing the Global Obesity Epidemic Awareness Building, Education, and Research –Department of Health and Human Services (DHHS) Centers for Disease Control and Prevention (CDC) National Institutes of Health (NIH)
 Centers for Disease Control and Prevention (CDC) National Institutes of Health (NIH)")
30
© 2006 Thomson-Wadsworth

32
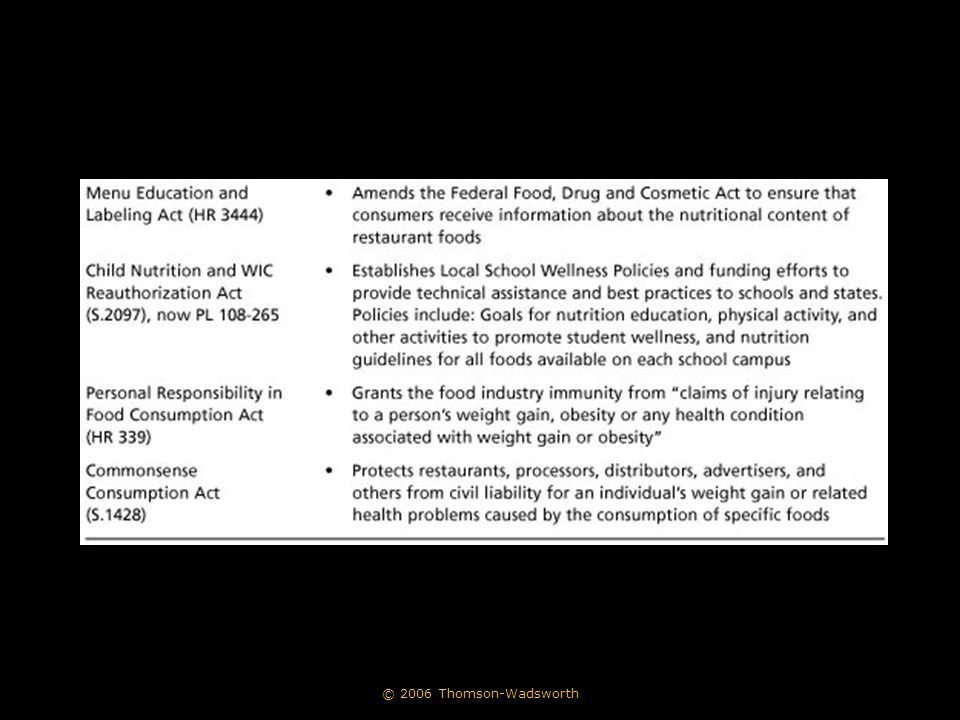
Public Health Policy Options for Addressing the Global Obesity Epidemic Awareness Building, Education, and Research (continued) –United States Department of Agriculture (USDA) –Federal Trade Commission (FTC) –Recent Legislative Efforts
 –United States Department of Agriculture (USDA) –Federal Trade Commission (FTC) –Recent Legislative Efforts")
33
© 2006 Thomson-Wadsworth

35
Public Health Policy Options for Addressing the Global Obesity Epidemic Regulating Environments –The Food Environment –The School Environment –The Built Environment

36
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Private Enforcement and Litigation –Personal Responsibility in Food Consumption Act (H.R. 339) –Commonsense Consumption Act (S 1428)
 –Commonsense Consumption Act (S 1428).")
37
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Pricing Policies –The U.S. Congress supports food industries, particularly agribusiness, through subsidies, price fixing, and price supports. –In response, price policies, such as subsidies and taxing, have been suggested as a way to reverse the obesity epidemic.

38
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Societal-Level Solutions –In general, low socioeconomic status (SES) groups are more likely to be obese than their high-SES counterparts in industrialized countries. –Upper SES groups are more likely to be obese in developing countries. –In developing nations, childhood obesity is most prevalent in wealthier sections of the population.

39
© 2006 Thomson-Wadsworth Public Health Policy Options for Addressing the Global Obesity Epidemic Societal-Level Solutions (continued) –A primary goal of public health initiatives addressing the global obesity epidemic is to increase the consciousness in the non- health sectors of the potential adverse effects of their various actions on the ability of people to maintain energy balance. Culture and education Commerce and trade Development Planning Transport

40
© 2006 Thomson-Wadsworth

41
Coordinated School Health Programs Coordinated School Health Program - CDC model that views the school in a multidimensional fashion, in which all components at the school level work together to maintain consistent, healthful messages.

42
© 2006 Thomson-Wadsworth

43
Coordinated School Health Programs Coordinated Approach To Child Health (CATCH) program –Probably the best example of a coordinated school health program that addresses both nutrition and physical activity
 program –Probably the best example of a coordinated school health program that addresses both nutrition and physical activity")
44
© 2006 Thomson-Wadsworth Coordinated School Health Programs Goals and Objectives –Overall goal = create healthy children and healthy school environments –Specific aims: Encourage students to consume a diet that is low in fat and saturated fat and higher in fruits and vegetables Encourage students to participate in increased amounts of moderate to vigorous physical activity (MVPA)
")
45
© 2006 Thomson-Wadsworth Coordinated School Health Programs Goals and Objectives –Specific aims (continued): Increase MVPA in schools to 50% of the physical education class Provide food in school cafeterias that is lower in fat and saturated fat Encourage parental participation in the school health program
: Increase MVPA in schools to 50% of the physical education class Provide food in school cafeterias that is lower in fat and saturated fat Encourage parental participation in the school health program")
46
© 2006 Thomson-Wadsworth Coordinated School Health Programs Priority Population –Target population groups: –Elementary school children and their parents –Elementary school teachers –School administration and staff –Main trial included a cohort of 5,106 third-grade students from 96 schools in 4 sites

47
© 2006 Thomson-Wadsworth Coordinated School Health Programs Rationale for the Intervention –Children’s diets were high in fat and saturated fat –Health behaviors track from childhood into adulthood –Therefore, changes in children’s diets/physical activity habits would benefit them in the future as well as in the present

48
© 2006 Thomson-Wadsworth Coordinated School Health Programs Methodology –Randomized clinical trial (main CATCH study) –Each of 96 schools at 4 sites was assigned to 1 of 3 conditions: Control (usual health program) (n = 40) School-based program (n = 28) School-based program plus family component (n= 28)
 –Each of 96 schools at 4 sites was assigned to 1 of 3 conditions: Control (usual health program) (n = 40) School-based program (n = 28) School-based program plus family component (n= 28)")
49
© 2006 Thomson-Wadsworth Coordinated School Health Programs Methodology (continued) –Main trial followed by dissemination phase –Opinion leaders and change agents were contacted Opinion leaders - people who influence other people’s attitudes about a program Change agents - people who can influence decisions to implement a program
 –Main trial followed by dissemination phase –Opinion leaders and change agents were contacted Opinion leaders - people who influence other people’s attitudes about a program Change agents - people who can influence decisions to implement a program")
50
© 2006 Thomson-Wadsworth Coordinated School Health Programs Methodology (continued) –They influenced others to adopt the program or suggest legislative efforts –Partnerships formed between groups with the common goal of promoting school- based physical activity and nutrition programs –CATCH dissemination was measured using quantitative and qualitative methods
 –They influenced others to adopt the program or suggest legislative efforts –Partnerships formed between groups with the common goal of promoting school- based physical activity and nutrition programs –CATCH dissemination was measured using quantitative and qualitative methods")
51
© 2006 Thomson-Wadsworth Coordinated School Health Programs Results –Significant changes in self-reported diet and physical activity levels of the children –Changes maintained for 3 years without additional intervention –As of October 2004: > 1,600 schools had adopted part of the CATCH curriculum > 700 schools had been trained in coordinated school health

52
© 2006 Thomson-Wadsworth Coordinated School Health Programs Lessons Learned –It is possible to implement a school- based health promotion program to change child/adolescent diet and physical activity patterns –Changes in diet and physical activity do not necessarily result in changes in related physiologic risk factors

53
© 2006 Thomson-Wadsworth Coordinated School Health Programs Lessons Learned (continued) –Example of translational research Translational research - research in which studies that are rigorously evaluated under controlled conditions and show promising results are “translated” into community-based interventions that are implemented in real-life situations
 –Example of translational research Translational research - research in which studies that are rigorously evaluated under controlled conditions and show promising results are translated into community-based interventions that are implemented in real-life situations")
54
© 2006 Thomson-Wadsworth Where Do We Go From Here? The awareness of obesity and overweight as a significant public health issue is in its beginning stages. In general, environmental changes will need a strong lead from policy and/or social change. The roles of the community nutritionist in this endeavor are varied and crucial.

55
© 2006 Thomson-Wadsworth Cigarette Consumption and Public Health Initiatives

56
© 2006 Thomson-Wadsworth

58
Diet Confusion: Weighing the Evidence How Do Diets Work? –Diets work because people limit their food consumption. –Table 8-10 compares caloric content and macronutrient distribution of several types of diets...

59
© 2006 Thomson-Wadsworth

61
Diet Confusion: Weighing the Evidence What Are Some Common Diets? –Common diets appearing in recent years include the following...

62
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Dr. Atkins New Diet Revolution –Consumption of high-fat meats, cheeses, and fats is encouraged –Consumption of carbohydrates is severely limited –Underlying premise = elimination of these foods will produce “benign dietary ketoacidosis”

63
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence The Zone Diet –Rigid eating plan that separates foods into “macronutrient blocks” The South Beach Diet –More healthful version of the Atkins diet –Incorporates lower-fat protein sources such as chicken, fish, whole grains, vegetables and fruits

64
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Weight Watchers –Dieters may use a list of core foods or a point system to select and eat foods to reduce caloric intake Dr. Ornish Eat More, Weigh Less –A very-low-fat diet with little meat, oils, nuts, butter, dairy (except non-fat), sweets, or alcohol –Original Ornish plan included exercise and stress reduction
, sweets, or alcohol –Original Ornish plan included exercise and stress reduction.")
65
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Eat Right for Your Blood Type –Based on the claim that your blood type determines the types of foods that you should eat and how your body absorbs nutrients –[Pause for uproarious laughter]
![© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Eat Right for Your Blood Type –Based on the claim that your blood type determines the types of foods that you should eat and how your body absorbs nutrients –[Pause for uproarious laughter]](http://images.slideplayer.com/16/5129424/slides/slide_65.jpg "© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Eat Right for Your Blood Type –Based on the claim that your blood type determines the types of foods that you should eat and how your body absorbs nutrients –[Pause for uproarious laughter]")
66
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence Dr. Phil’s Ultimate Weight Solution –Book focuses on “Keys to Weight Loss Freedom” –No defined meal plans or recipes –Promotes seafood, poultry, meat, low-fat dairy, whole grains, fruits, vegetables, some oils, supplements, weight-loss bars and shakes

67
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence The New Glucose Revolution –Encourages consumption of low- glycemic foods, such as beans, pasta, most fruits, vegetables, low-fat dairy, and meats

68
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence How Can You Evaluate a Diet to Determine Whether It Is Healthful? –Does the weight-loss program systematically eliminate one group of foods from a person’s eating pattern? –Does the weight-loss program encourage specific supplements or foods that can be purchased only from selected distributors? –Does the weight-loss program tout magic or miracle foods or products that burn fat?

69
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence How Can You Evaluate a Diet? (cont.) –Does the weight-loss program promote bizarre quantities of only one food or one type of food? –Does the weight-loss program have rigid menus? –Does the weight-loss program promote specific food combinations? –Does the weight-loss program promise a weight loss of more than 2 pounds per week for an extended period of time?
 –Does the weight-loss program promote bizarre quantities of only one food or one type of food. –Does the weight-loss program have rigid menus. –Does the weight-loss program promote specific food combinations. –Does the weight-loss program promise a weight loss of more than 2 pounds per week for an extended period of time .")
70
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence How Can You Evaluate a Diet? (cont.) –Does the weight-loss program provide a warning to people with diabetes, high blood pressure, or other health conditions? –Does the weight-loss program encourage or promote increased physical activity? –Does the weight-loss program encourage an intake that is very low in calories (below 800 kcal/d) without supervision of medical experts?
 –Does the weight-loss program provide a warning to people with diabetes, high blood pressure, or other health conditions. –Does the weight-loss program encourage or promote increased physical activity. –Does the weight-loss program encourage an intake that is very low in calories (below 800 kcal/d) without supervision of medical experts .")
71
© 2006 Thomson-Wadsworth Diet Confusion: Weighing the Evidence What Can You Do? –Be familiar with the current fad diets. –Recommend appropriate weight-loss strategies and programs. –Refer the public to websites that list resources for determining whether a diet is a fad. –Report fraudulent or deceptive weight-loss claims.

Similar presentations