Download presentation
Presentation is loading. Please wait.

1
Kinza Ali

2
Cardiomyopathies are a group of diseases primarily involving the myocardium and is characterized by myocardial dysfunction that is not the result of hypertension, coronary atherosclerosis, valvular dysfunction, or pericardial abnormalities.

3
The main types of cardiomyopathy are: Dilated cardiomyopathy (Congestive, ACM, IDC) ▪ Ventricular enlargement and systolic dysfunction Hypertrophic cardiomyopathy (IHSSic, HOCM) ▪ Inappropriate myocardial hypertrophy in the absence of Hypertension or aortic stenosis Restrictive cardiomyopathy(infiltrative) ▪ Abnormal filling and diastolic dysfunction
 ▪ Ventricular enlargement and systolic dysfunction Hypertrophic cardiomyopathy (IHSSic, HOCM) ▪ Inappropriate myocardial hypertrophy in the absence of Hypertension or aortic stenosis Restrictive cardiomyopathy(infiltrative) ▪ Abnormal filling and diastolic dysfunction")
4
Most common type of cardiomyopathy Generally occurs between ages of 20 to 60 years More common in men Heart begins to dilate or stretch and become thinner increased ventricular chamber size Systolic dysfunction Reduced CO increased EDV weakness and shortness of breath biventricular CHF

6
Most commonly Idiopathic Toxic: due to cocaine, amphetamines, and some chemotherapy drugs (doxorubicin, daunorubicin) Ischemic: caused by CAD and MI, leave scars in the heart muscle Infectious: HIV, viral myocarditis due to coxasackie B or echovirus Alcoholic: happens 10 years after sustained, heavy alcohol consuption Pregnancy
 Ischemic: caused by CAD and MI, leave scars in the heart muscle Infectious: HIV, viral myocarditis due to coxasackie B or echovirus Alcoholic: happens 10 years after sustained, heavy alcohol consuption Pregnancy")
7
Signs of CHF Dyspnea on exertion, orthopnea, paraoxysmal nocturnal dyspnea Palpitations Fatigue Resting tachycardia Mitral regurgitation NormalDCM Ejection fraction (>55%) LV Diastolic Dimension (<55mm) LV wall thickness Atrial size Valvular regurgitation Common first Symptoms <30% >60mm Decreased Increased Mitral Exertion intolerace
 LV Diastolic Dimension (<55mm) LV wall thickness Atrial size Valvular regurgitation Common first Symptoms <30% >60mm Decreased Increased Mitral Exertion intolerace")
8
Most common cause of death in young people Occurs when muscle thickens abnormally ( usually LV)=impaired diastolic function the ventricles fill with less blood because the thickened walls are less compliant and take up too much space, and the heart has too much muscle to be able to support its own energy needs Diastolic failure, increased ejection fraction Sudden death due to ventricular arrhythmias
=impaired diastolic function the ventricles fill with less blood because the thickened walls are less compliant and take up too much space, and the heart has too much muscle to be able to support its own energy needs Diastolic failure, increased ejection fraction Sudden death due to ventricular arrhythmias")
9
Two types of HCM: obstructive and non obstructive. Septum thickens and bulges into the left ventricle, blocks flow of blood into aorta. Thick but not abnormal thick that any part of it crowds the ventricles Noncompliant chamber= decrease diastolic filling=increased ED pressure=increase pulmonary venous pressure

10
50% of cases are familial Mutations in one of 4 genes encoding proteins of cardiac sarcomere accounts for majority of familial cases -MHC, Cardiac troponin, myosin binding protein C, alpha-tropomyosin Genetic IHSS (1:500 young athletes affected) Autosomal dominant Beta-MHC Often Idiopathic
 Autosomal dominant Beta-MHC Often Idiopathic")
11
Dyspnea Syncope (usually seen with exercise) Angina Palpitations Sudden death: may be the only manifestation S4: atria contracts, fluid going into harder surface Diagnose it with ECG (atrial enlargement, V hypertrophy), echo, histology, etc.
 Angina Palpitations Sudden death: may be the only manifestation S4: atria contracts, fluid going into harder surface Diagnose it with ECG (atrial enlargement, V hypertrophy), echo, histology, etc.")
12
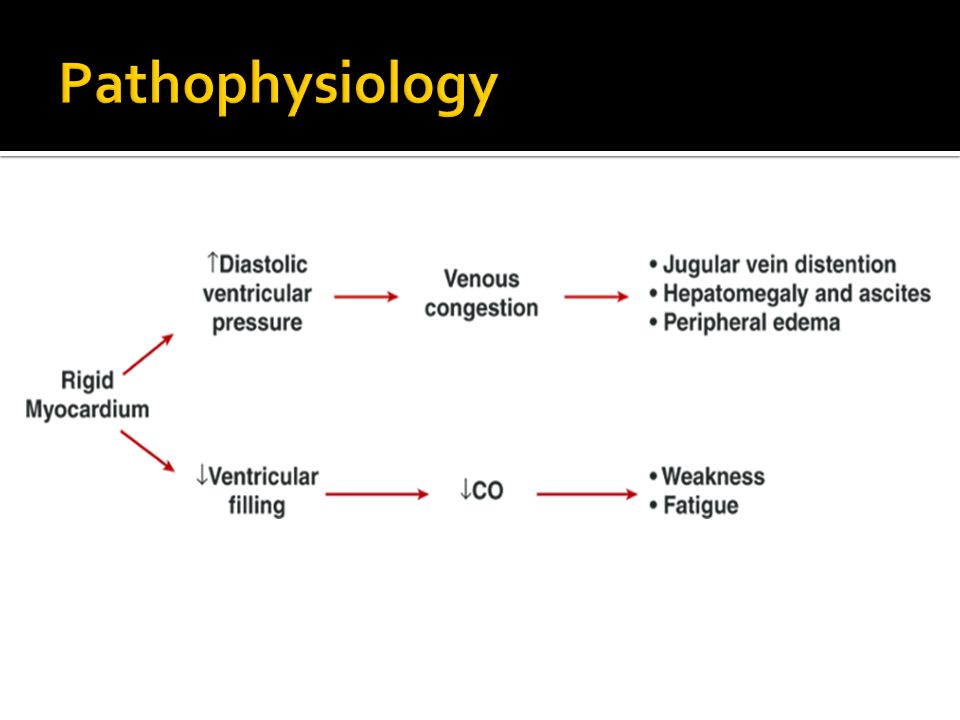
Less common, tends to mostly affect older adults Myocardial infiltration causing decreased compliance and rigidity The ventricles become stiff and rigid because of scar tissue formation Atria enlargement Heart failure/arrthymias

14
Main causes include: Post-Radiation therapy Collagen Vascular disease Amyloidosis: insoluble proteins deposit within tissues Hemacuromatosis

15
Presents with symptoms of progressive left sided and right sided heart failure: Edema, ascites, hepatomegaly, distended neck veins may be present Fatigue, weakness Congestive heart failure

16
Manage any conditions that cause or contribute to the cardiomyopathy Diet, physical activity, and lifestyle changes Diuretics: remove excess fluid and sodium from the body ACE inhibitors: lowers blood pressure and reduces stress on heart Beta blockers: slows heart rate by reducing the speed of the heart contraction. Also lowers BP.

17
Digoxin (avoid in amyloidosis) Antiarrhythmics (amiodorone) Calcium channel blockers: slows rapid heartbeart by reducing the force and rate of heart contractions, decrease BP. Anticoagulants

18
A 39 year old school teacher, presented on account of progressive dyspnea associated with orthopnea, palpitations and bilateral leg swelling. There was no previous remarkable illness or hospital admission. She had a history of daily ingestion of alcohol for 8 years. On examination she was in respiratory distress, had bilateral basal crepitation, an irregular pulse, elevated jugular venous pulse, a displaced non heaving apex with left parasternal heave, and a non radiating apical pansystolic murmur. She also had a tender hepatomegaly, and bilateral pitting pedal edema. A chest radiograph showed upper lobe diversion, bilateral hilar opacities and a multi chamber cardiomegaly. A 12 lead surface electrocardiogram (ECG) showed atrial supraventricular and ventricular ectopics, and echocardiography showed, four chamber dilatation with poor systolic function and absent a waves.
 showed atrial supraventricular and ventricular ectopics, and echocardiography showed, four chamber dilatation with poor systolic function and absent a waves..")
19
http://www.nhlbi.nih.gov/health/health- topics/topics/cm/signs.html http://www.nhlbi.nih.gov/health/health- topics/topics/cm/signs.html http://circheartfailure.ahajournals.org/conten t/6/2/e19.extract http://circheartfailure.ahajournals.org/conten t/6/2/e19.extract http://medind.nic.in/jal/t04/i4/jalt04i4p157.pd f http://medind.nic.in/jal/t04/i4/jalt04i4p157.pd f http://www.clevelandclinicmeded.com/medic alpubs/diseasemanagement/cardiology/dilat ed-restrictive-cardiomyopathy/

Similar presentations







 Deterioration of heart muscle Becomes enlarged, thick or rigid Scar tissue Pumping blood.>")








, means your heart can't pump enough blood to meet your body's.>")



