Download presentation
Presentation is loading. Please wait.

1
James Nott CT1 ACCS

2
Epidemiology and Definition Pathophysiology of Stress ulcers Clinical presentation Risk factors Prophylaxis agents available – mechanisms Meta-Analysis: PPIs vs H 2 RA for stress ulcer prophylaxis in critically ill patients.

3
Common ~ 1.5 – 8.5% GI bleeding in all ICU patients 15% - 25% of ICU patients not on prophylaxis 75% mucosal abnormalities of ICU patients <72hrs (major burn/cranial trauma) Ulcer: ‘Lesion of mucosal membrane accompanied by oedema and necrosis of surrounding tissue’ Loci: Stress ulcers - Fundus (Proximal) Peptic ulcers - antrum (Distal) / proximal duodenum Presentation range: Asymptomatic – Acute haemorrhage depending on depth of ulcer
 Ulcer: ‘Lesion of mucosal membrane accompanied by oedema and necrosis of surrounding tissue’ Loci: Stress ulcers - Fundus (Proximal) Peptic ulcers - antrum (Distal) / proximal duodenum Presentation range: Asymptomatic – Acute haemorrhage depending on depth of ulcer")
4
Imbalance: mucosal protection vs gastric pH Multi-factorial:

5
Range depends on depth of ulcer Superficial: Asymptomatic Deep: Haemorrhage (Haematemesis /Melena)
")
6
Intubated >48hrs OR 15.6 (3) Cook. DJ et al ’94 Coagulopathy OR 4.3 Additional risks identified: SHOCK Everyone! Sepsis Hepatic and Renal failure Multiple trauma Burns of >35% BSA Glucocorticoid therapy

7
Pharmacological mechanisms: 1) Block acid secretion Competitive H 2 antagonists (Ranitidine) Proton pump inhibitors (Omeprazole) 2) Neutralise stomach acid contents Antacids (Gaviscon) – Bicarbonate neutralises pH
 Block acid secretion Competitive H 2 antagonists (Ranitidine) Proton pump inhibitors (Omeprazole) 2) Neutralise stomach acid contents Antacids (Gaviscon) – Bicarbonate neutralises pH")
8
3) Protecting stomach mucosa – nil buffering Sucraflate - polysaccharide + Aluminium hydroxide 4) Prostaglandin analogues Misoprostol – inhibit parietal cells to generate cAMP, thus reduce stomach acid secretion
 Protecting stomach mucosa – nil buffering Sucraflate - polysaccharide + Aluminium hydroxide 4) Prostaglandin analogues Misoprostol – inhibit parietal cells to generate cAMP, thus reduce stomach acid secretion")
9
Nosocomial pneumonia (HAP/VAP) ↑ pH – Less hostile environment for bacteria Not so with Sucralfate (not affects pH) Ways to reduce risk: (Preventing aspiration) - Patient position – semirecumbant not supine - Mouth care – Chlorhexidine mouthwash/gel - Subglotic drainage - ? Residual gastric monitoring

10
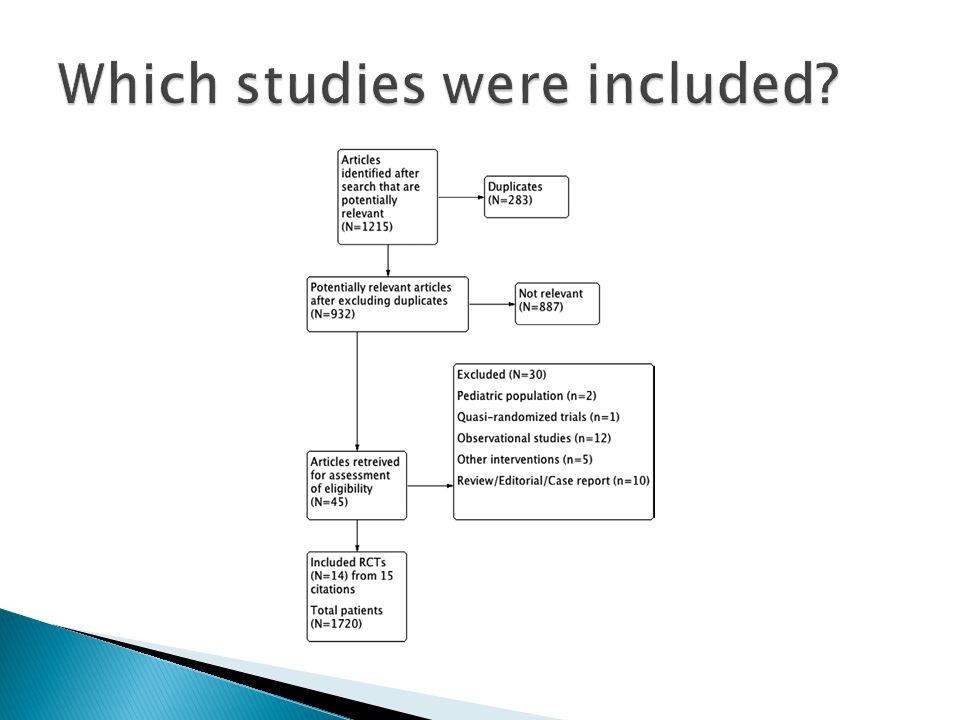
Aim: ‘Determine efficacy and safety of proton pump inhibitors verses H 2 receptor antagonists for the prevention of upper GI bleeding in ICU’ Methodology: Search strategy – MEDLINE (1948-March 2012) EMBASE (1980-March 2012) Two researchers independently ACPJC (1991-March 2012) extracted data Cochrane (central) database CINHAL. Any disagreements resolved by discussion or consensus

11
Types of study: - Randomised Control Trials (RCTs) Population: - ICU Adults (Medical and Surgical included) Intervention: - Control= H 2 RA Intervention=PPIs - para-enteral/enteral - regardless of dose, frequency and duration
 Population: - ICU Adults (Medical and Surgical included) Intervention: - Control= H 2 RA Intervention=PPIs - para-enteral/enteral - regardless of dose, frequency and duration")
12
Primary outcomes : - clinically important GI bleed (?Meaning Hb drop/instability) - overt upper GI bleeding (coffee ground emesis, melena, fresh blood PR from UGI ) Secondary outcomes : - Nosocomial pneumonia (VAP/HAP) - All-cause mortality - ICU length of stay - C. Diff infection

13
All trials assessed for risk, depending on domains: - Low = risk low in ALL domains - Unclear =risk is unclear in >1 domain - High = risk is high in >1 domain Domains: Sequence Generation Allocation concealment Blinding Incomplete outcome data Selective reporting bias Free of other bias Plus – Overall risk of bias

15
Data analysed using RevMan 5.1 model. Pooled: Dichotomous outcomes - RR 95% CI Continuous outcomes – Mean Methods of assessing heterogeneity (? Bias): Subgroup analysis – Size, Egger’s test /funnel plot to assess publication bias
: Subgroup analysis – Size, Egger’s test /funnel plot to assess publication bias.")
16
Primary objectives: 1) Clinically important bleeding (12 Trials n=1614) Significantly lower RR with PPIs vs H 2 RA: (RR 0.36 95% CI 0.19-0.68 p=0.002)
 Clinically important bleeding (12 Trials n=1614) Significantly lower RR with PPIs vs H 2 RA: (RR % CI p=0.002)")
17
2) Overt Bleeding ( 14 Trials n= 1720) Significantly lower RR with PPIs vs H 2 RA: (RR 0.35; 95%CI 0.21-0.59 p<0.0001)
 Overt Bleeding ( 14 Trials n= 1720) Significantly lower RR with PPIs vs H 2 RA: (RR 0.35; 95%CI p<0.0001)")
18
1) Nosocomial Pneumonia ( 8 Trials, n= 1100) No significant difference: RR 1.06 95% CI (0.73- 1.52) p=0.76
 Nosocomial Pneumonia ( 8 Trials, n= 1100) No significant difference: RR % CI ( ) p=0.76")
19
2) Mortality ( 8 Trials n= 1196) No significant difference: RR 1.01 95% CI (0.83- 1.24) p=0.91
 Mortality ( 8 Trials n= 1196) No significant difference: RR % CI ( ) p=0.91")
20
3) ICU Length of stay ( 5 Trials n=555) No significant difference :CI (-2.20-1.13) p=53 4) Clostridium difficile infection No trials reported on C. Difficile infection

21
‘ Significantly ↓ risk of both 1 0 outcomes with PPIs - Clinically important GI bleeding – RR 0.36 (0.19-0.68) - Overt UGI bleeding – RR 0.35 (0.21-0.59) ‘No significant ↓ risk of 2 0 outcomes with PPIs vs H 2 RA’ Nosocomial pneumonia – RR 1.06 (0.73-1.52) ICU mortality – RR 1.01 (0.83-1.24) ICU length of stay – RR 0.54 (-2.20-1.13)
 - Overt UGI bleeding – RR 0.35 ( ) ‘No significant ↓ risk of 2 0 outcomes with PPIs vs H 2 RA’ Nosocomial pneumonia – RR 1.06 ( ) ICU mortality – RR 1.01 ( ) ICU length of stay – RR 0.54 ( )")
22
Primary outcomes (14 Trials): Low risk of bias – 3 Inflates benefit of PPIs Unclear – 5 High risk of bias – 6 (lack of blinding) Publication bias (Funnel plot): Larger trials (y axis) are more reliable – closer to mean RR (x axis) Inverted funnel shape Clinically important bleeding Overt bleeding outcome
: Low risk of bias – 3 Inflates benefit of PPIs Unclear – 5 High risk of bias – 6 (lack of blinding) Publication bias (Funnel plot): Larger trials (y axis) are more reliable – closer to mean RR (x axis) Inverted funnel shape Clinically important bleeding Overt bleeding outcome")
23
Definitions varied (Pneumonia) No randomisation of nutritional strategies Age of studies (1948) – ? relevance to today’s Accepts - ‘PPIs may lower risk of GI bleeding’ Welcomes further research: - Effect of early nutrition - Cost-benefit analysis - C. Diff infection

24
NO! Meta-analysis does not show significant evidence that PPIs are better than H 2 RAs. Rantidine is cheap and as effective as PPIs for ulcer prophylaxis, so why change? Establish enteral nutrition important – no statistical evidence.

25
Thank you, any questions!?!

26
1) Cook.DJ, Stress ulcer prophylaxis. Best evidence synthesis Scand J Gastroenterol Supple 1995; 210:48 2) Stollman. N, Pathophysiology and prophylaxis of stress ulceration in ICU, Journal of critical care, vol 20, March 2005 3) Cook. DJ et al, risk factors for gastrointestinal bleeding in critical ill patients, Canadian Critical Care Trials Group. N Engl J Med 1994; 330:377 5) Marik P.E et al, Stress ulceration prophylaxis in the new millennium, meta-analysis. Critical Care Med 2010; 38:2222
 Stollman. N, Pathophysiology and prophylaxis of stress ulceration in ICU, Journal of critical care, vol 20, March ) Cook. DJ et al, risk factors for gastrointestinal bleeding in critical ill patients, Canadian Critical Care Trials Group. N Engl J Med 1994; 330:377 5) Marik P.E et al, Stress ulceration prophylaxis in the new millennium, meta-analysis. Critical Care Med 2010; 38:2222.")
Similar presentations
 for severe sepsis and septic shock treatment>")




 2004 Elsevier Inc. All rights reserved. Drugs for Peptic Ulcer Disease Chapter 73.>")




>")








 in Critically Ill Patients Liz Goddard.>")