Download presentation
Presentation is loading. Please wait.

2
Enhanced recovery meta-analysis Kirsty Cattle Research Registrar

3
The paper

4
Introduction –Enhanced recovery: –A combination of interventions aimed at reducing the operative stress response, resulting in faster recovery –Therefore often called the “fast-track programme”

5
–Aim of study: –The evidence for enhanced recovery comes from observational studies and consensus opinion. –Previous systematic review was felt to be inadequate

6
Methods –Define colorectal enhanced recovery surgery: –Enhanced recovery elements:

8
Methods –Define colorectal enhanced recovery surgery: –Enhanced recovery elements: –Include five elements, at least one from each of pre-, peri- and post-operative period –“A circumferential segmental excision of any part, or parts, of the colon and or rectum involving either a primary anastomosis and or stoma formation”

9
–Identify randomised controlled trials and clinical controlled trials by searching: –Medline, Embase, Cochrane Colorectal Cancer Group Database, Cochrane Register of Controlled Trials (CENTRAL) –1966 to 2006 –Review of list of references in relevant articles
 –1966 to 2006 –Review of list of references in relevant articles")
10
–Outcomes: –Primary: total primary length of stay –Secondary: Primary length of stay plus length of any readmissions Readmissions Morbidity Mortality –If necessary, data was obtained by contacting the authors directly

11
–Analysis: –Weighted mean difference for continuous data –Relative risk for categorical data –Heterogeneity examined (I 2 test)
")
12
Results –71 papers assessed, 4 papers included in meta-analysis –376 patients, 64 within RCTs –11 deaths –Bias: –2 RCTs, both from same centre, inadequacies with randomization –2 CCTs, comparing different centres or wards

13
Meta-analysis –Total primary length of stay: –Included RCT data only, therefore 64 patients –Homogenous studies –Both primary length of stay and total stay secondary to readmissions reduced in enhanced recovery groups: Primary LOS reduced by 3.64 (95% CI -4.98 to -2.29) days Total 30 day LOS reduced by 3.75 (95% CI -5.11 to - 2.40) days
 days Total 30 day LOS reduced by 3.75 (95% CI to ) days")
15
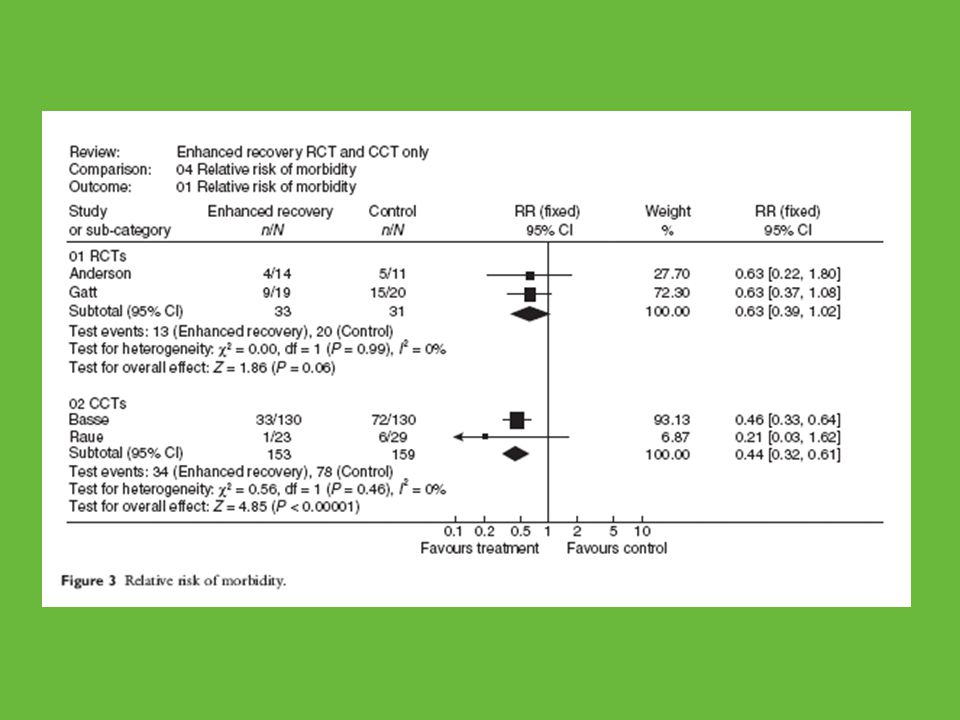
–Morbidity: –Lower relative risk of 30 day morbidity among enhanced recovery group: RR = 0.44, p < 0.0001, combined RCT and CCT data –No statistically significant difference when RCTs alone examined RR= 0.63, p = 0.06, RCT data only

17
–Mortality: –No significant difference in mortality rates between enhanced recovery and standard care RR = 0.92, p = 0.93, RCT data RR = 2.0, p = 0.32, CCT data

18
–Readmission rates: –Equivocal data reported Lower readmission rates among enhanced recovery group reported in one RCT, RR = 0.26, p = 0.21 Lower readmission rates among control group reported from both CCTs, RR = 1.73, p = 0.05 Pooled data: RR 1.46, p = 0.15

19
Discussion –Their conclusions match the conclusions of the previous meta-analysis and support it by being a stronger meta-analysis –Exclusion of non-colorectal papers –Lower heterogeneity –Analysis of total 30-day length of stay –Morbidity and mortality data should be interpreted with caution due to small numbers –Difficult to determine if enhanced recovery gives better outcomes due to constituent parts or the overall package

20
Critique –Small numbers, only 4 papers, including only 2 RCTs, both from same centre, 2 years apart. –Primary outcome based on RCTs only –My conclusions: –More background reading first

Similar presentations