Download presentation
Presentation is loading. Please wait.

1
A Randomized Trial of Protocol-Based Care for Early Septic Shock Andrea Caballero, MD January 15, 2015 LSU Journal Club The ProCESS Investigators. N Engl J Med 2014; 370:1683-1693. May 1, 2014.

2
Background There are over 750,000 cases of severe sepsis and septic shock per year in the US. Short term mortality is estimated to be >20% Many of our current guidelines are based on the 2001 Rivers et al paper – Single-center – Showed that mortality was lower in the population treated according to the 6hr protocol of EGDT (early-goal directed therapy)
.")
3
Objective Are all elements of that protocol still applicable a decade later?

4
Methods 31 academic hospitals in the US – These had to adhere to the Surviving Sepsis Campaign Guidelines for nonresuscitation protocols but did not routinely use SvcO2 monitoring and had no routine resuscitation protocols – Serum lactate was used as the method for screening cryptogenic shock Patient selection – >18 years of age – Meet 2 SIRS criteria – Had refractory hypotension (1L in 30 minutes) or lactic acid >/=4mmol/L Exclusion criteria – Primary diagnosis of acute CVA, ACS, acute pulmonary edema, status asthmaticus, major cardiac arrhythmias, active GIB, seizure, drug overdose, burn or trauma – Requirement for immediate surgery. CD4<50cells/mm2. Advanced directives restricting the protocol. C/i to CVC. High likelihood of refusing blood transfusion. Transfer from outside hospital. Pregnancy. Deemed futile care by treating physician.

5
Three Groups Protocol-based EGDT Protocol-based Standard Therapy Usual Care Randomization 1:1:1

6
Protocol- based EGDT

7
Protocol- based Standard Therapy

8
Patient Selection

9
Outcomes Measured Primary end-point was the rate of in-hospital death from ANY cause at 60 days Secondary mortality outcomes – Rate of death from ANY cause at 90 days – Cumulative mortality at 90 days and 1 year Other outcomes – Duration of acute cardiovascular failure (need for vasopressors) – Acute respiratory failure (duration of mech vent – Acute renal failure (duration of HD)
 – Acute respiratory failure (duration of mech vent – Acute renal failure (duration of HD)")
10
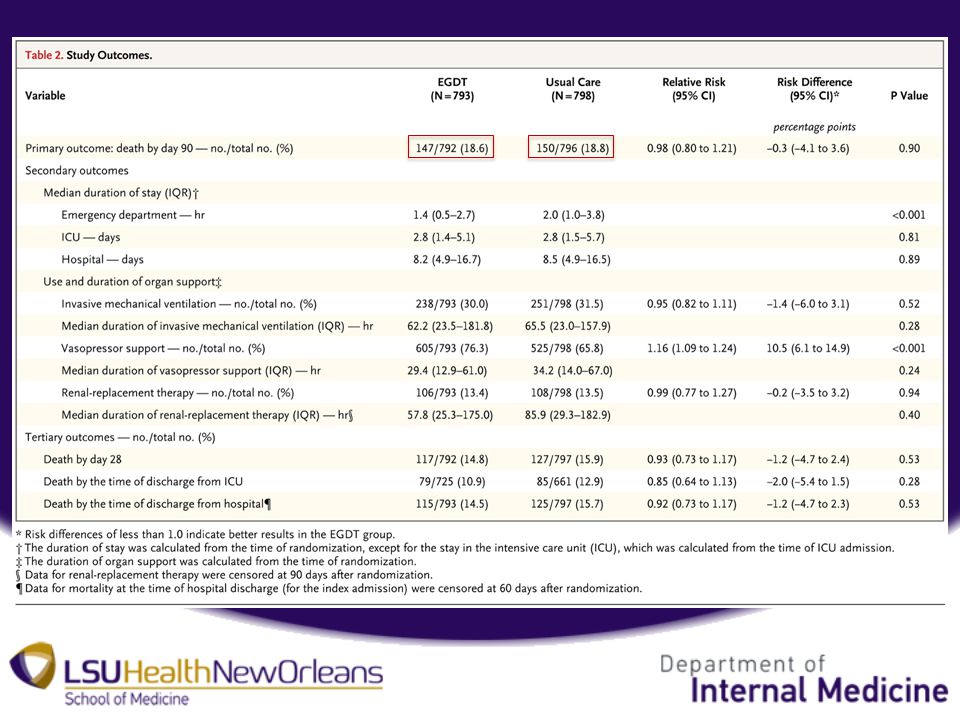
Results

11
Incidence of acute renal failure was highest in the Protocol-Based Standard, even though duration of therapy did not differ between groups No significant differences in incidence and duration of cardiovascular failure or respiratory failure or length of stay in hospital

12
Results Protocol based care resulted in more use of central venous catheterizations overall. Also increase use of IVF, vasoactive agents and blood transfusion in the initial 6hrs, with little difference between groups thereafter. By 6hrs, more patients in these two groups had reached the target MAP>/=65

13
Discussion – In Rivers et al. the patient population was older, had higher rates of pre-existing heart and liver disease, and higher initial lactate level. Initial SvcO2 reported was lower than in ProCESS (however it was measured after initial fluid bolus). – Care of critically ill patients has changed including lower Hgb threshold for transfusion, lung-protective strategies, tighter blood sugar control.
. – Care of critically ill patients has changed including lower Hgb threshold for transfusion, lung-protective strategies, tighter blood sugar control..")
14
Conclusion “In summary… patients [that] were identified EARLY in the emergency department as having SEPTIC SHOCK and received ANTIBIOTICS and other NONRESUSCITATION aspects of care promptly, we found NO ADVANTAGE, with respect to mortality or morbidity, of protocol-based resuscitation over bedside care… according to the treating physician’s judgment”.
![Conclusion In summary… patients [that] were identified EARLY in the emergency department as having SEPTIC SHOCK and received ANTIBIOTICS and other NONRESUSCITATION aspects of care promptly, we found NO ADVANTAGE, with respect to mortality or morbidity, of protocol-based resuscitation over bedside care… according to the treating physician’s judgment .](http://images.slideplayer.com/13/3843009/slides/slide_14.jpg "Conclusion In summary… patients [that] were identified EARLY in the emergency department as having SEPTIC SHOCK and received ANTIBIOTICS and other NONRESUSCITATION aspects of care promptly, we found NO ADVANTAGE, with respect to mortality or morbidity, of protocol-based resuscitation over bedside care… according to the treating physician’s judgment .")
15
“Goal-Directed Resuscitation for Patients with Early Septic Shock” The ARISE Investigators and the ANZICS Clinical Trials Group N Engl J Med 2014; 371:1496-1506. October 16, 2014 -Primary end point was 90 day mortality -51 centers in Australia and New Zealand -EGDT v Standard – which did not include SvcO2 monitoring (in first 6hrs) and decisions involving invasive monitoring, IVF rescuscitation, vasoactive support, transfusion and mechanical ventilation were discussed by the treating team
 and decisions involving invasive monitoring, IVF rescuscitation, vasoactive support, transfusion and mechanical ventilation were discussed by the treating team.")
17
Thank you

Similar presentations

 for severe sepsis and septic shock treatment>")

















