Download presentation
Presentation is loading. Please wait.

1
The Integrated Operations Center (IOC) An Operational Environment that supports teams in providing Quality Patient Care
 An Operational Environment that supports teams in providing Quality Patient Care")
2
What is our Integrated Operations Centre? Concept Place Purpose People

3
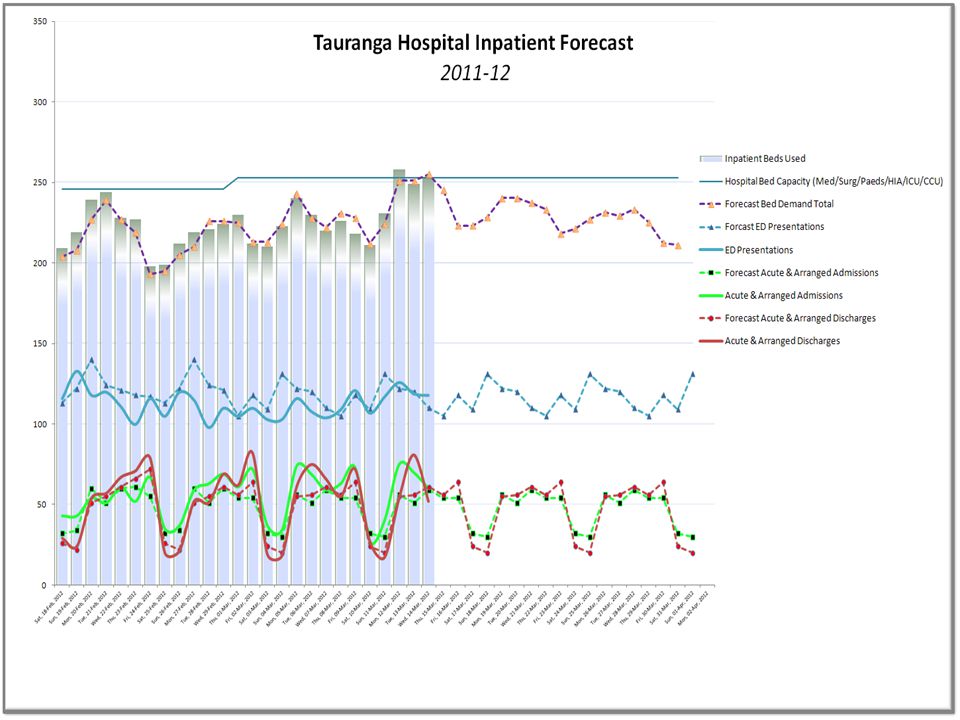
What Measurable Outcomes has it had? Acute patient journey - 6 hour target > 90% for 15/19 mnths – a sustained improvement Cared for 875 more acute patients YTD (4% increase YonY) while maintaining bed utilisation at 2008 levels by a reduction in ALOS, nos. of LOS outliers and improvements in discharge by 11 (using the transit lounge) and weekend discharges For the three months November to January we have been able to successfully keep closed 44 beds at Tauranga Hospital, and allow more staff to take annual leave over the summer/ school holiday, an have ongoing reduced occupancy
 while maintaining bed utilisation at 2008 levels by a reduction in ALOS, nos. of LOS outliers and improvements in discharge by 11 (using the transit lounge) and weekend discharges For the three months November to January we have been able to successfully keep closed 44 beds at Tauranga Hospital, and allow more staff to take annual leave over the summer/ school holiday, an have ongoing reduced occupancy.")
4
In 2009 – 2011 we had the Perfect Storm.. MOH 6 Hr Target expectations MOH Safe Staffing Healthy Workplaces – Care Capacity Demand Management trial site Air New Zealand Integrated Operations Centre visits

5
What do High Risk and High Performing Orgs have in Common?

6
And need to Minimise Variance Variance creates a productivity ‘black hole’ R isky!-increases patient risk and decreases quality of care Unsatisfactory-stressful and unsatisfactory for staff Unproductive!-diverts significant resource away from frontline care

7
Hospitals are High Risk Organisations with Significant Daily Variance at the front door

8
Added with Growth in Demand..

9
How do we achieve Safe Quality Care even on a busy day? Identify causes and address constraints Minimise and manage variation Predict demand Match demand with capacity

10
Methodology of the IOC Operations Management Principles – forecasting, planning, demand-capacity matching Think system-wide, not silo Visibility of operational status Data-driven Yesterday-Today –Tomorrow Aiming for a Learning Organisation

11
Assessing resource requirements plant people supply chain budget People fit for purpose Working systems Smoothing variability Information Environment fit for purpose Forecasting demand Estimating capacity Setting organisational goals Delivering effective services to patients Managing residual variance without compromising productivity Information 4. DELIVERING 1. FORECASTING 2. MATCHING 3. ESTABLISHING Patient MonitoringResponding SSHWP Model

12
IOC Roadmap Agreement on a Shared Vision Confirm membership of CCPG (Plus the project plan) Communication Plan - Social Movement / Culture Change AirNZ Visits, CCDM Think Tank, Vision Forum – COO, DON, Medical and Nurse Leaders, IT, DSAs, Non Clinical Support, SIU, Allied Health, Radiology Agreement to jointly proceed with IOC and CCDM project plan and confirm membership for governance overview for the process of change Resource commitment including training and education for CCDM members and others. Set up Steering group, agree TOR Communication on initiative to staff A culture change/ social movement targeted. Confirm change management and communication strategy

13
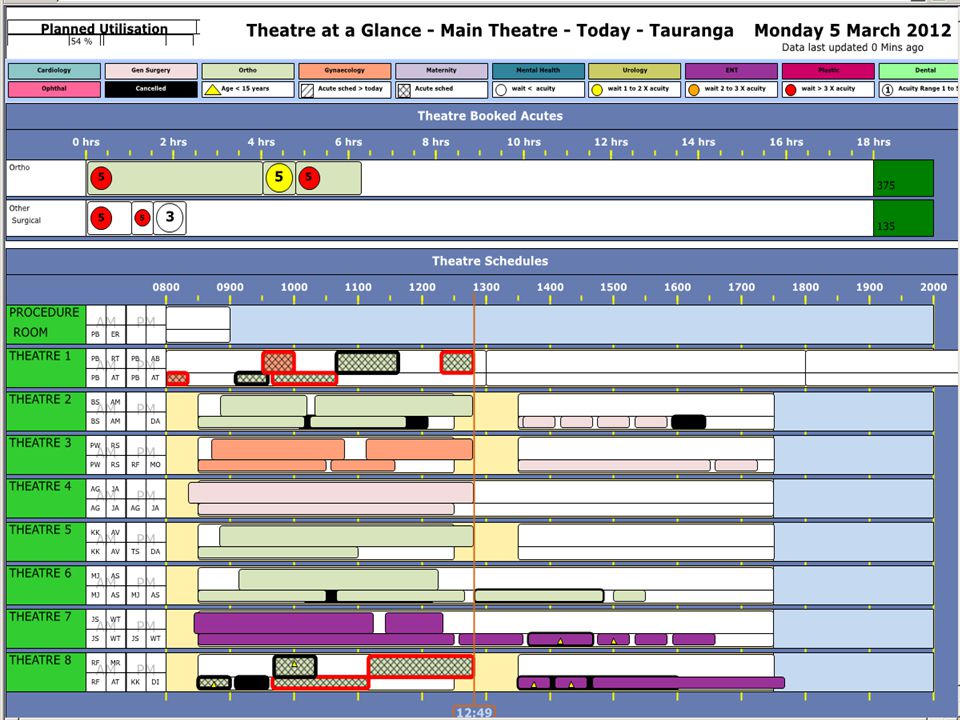
The 6 IOC Work Streams Co-location of Operations Staff Forecasting and Planning / CCDM “Status at a Glance” Data Views Daily IOC Meeting SOPs Working Relationships Face to face problem solving Innovation over the cooler Staffing units : RMO unit RN Bureau Admin Bureau Orderlies and security Coordinator Hospital Coordinator Duty Managers Emergency Planners From data bases - TrendCare, Webpas Proving to be very accurate Allows for Evidence based planning and staffing Built within the organisation, cost effective Organisation wide visibility and understanding/ awareness IT harnessed the data to increase understand around what is happening Scheduled work visible to all Enables early identification of exceptional circumstances Enables informed conversations across key groups for problem solving Operational oversight 11.30am Daily Operations Team Meetings - MDT, Whole of Hospital focus Operational decisions not made in isolation Yesterday, Today, Tomorrow Improvement Model VRM / CCDM Each team develops a VRM. Provide framework and context for escalation care capacity decision-making A live document ED SOP Developed (Northland DHB) Acute Patient Journey SOP developed Reflects patients location and stage of journey Whole of hospital agreement A live document
 Acute Patient Journey SOP developed Reflects patients location and stage of journey Whole of hospital agreement A live document.")
17
Forecasting 5 years of data Proving to be accurate Source, local data bases, Trendcare Allows for base line planning Staffing to need (evidence based) Built within the organisation, cost effective
 Built within the organisation, cost effective")
24
Standard Operating Procedures -SOPs Agreed Response Plan in advance with Front Line Staff and Service Leaders Standard Operating Procedures (SOP) – Agreed Business as Usual patient flow processes Variance Response Management Plans (VRM) – Essential Care Protocol On the Day SOPs used predominantly to unblock process constraints SOPs are developed and proposed in response to lessons learnt and evidence from the yesterday, today, tomorrow cycle VRMs are used when capacity and demand move into a mismatch Its about what's best for the patient and how the organisation can organise capacity to best deliver this
 – Agreed Business as Usual patient flow processes Variance Response Management Plans (VRM) – Essential Care Protocol On the Day SOPs used predominantly to unblock process constraints SOPs are developed and proposed in response to lessons learnt and evidence from the yesterday, today, tomorrow cycle VRMs are used when capacity and demand move into a mismatch Its about what s best for the patient and how the organisation can organise capacity to best deliver this")
25
CCDM- Care Capacity Demand Management Allocate resource to coordinate the strategy Take a whole of organisation/system approach High quality relationships & shared governance Electronic patient acuity/workload tool Variance response management

26
CCDM - Matching Resource Mix and Match – HIA, medical floors, ED, APU Staffing to forecasting Capacity management - 3A closed, CSU open Medical resource in APU SOP

28
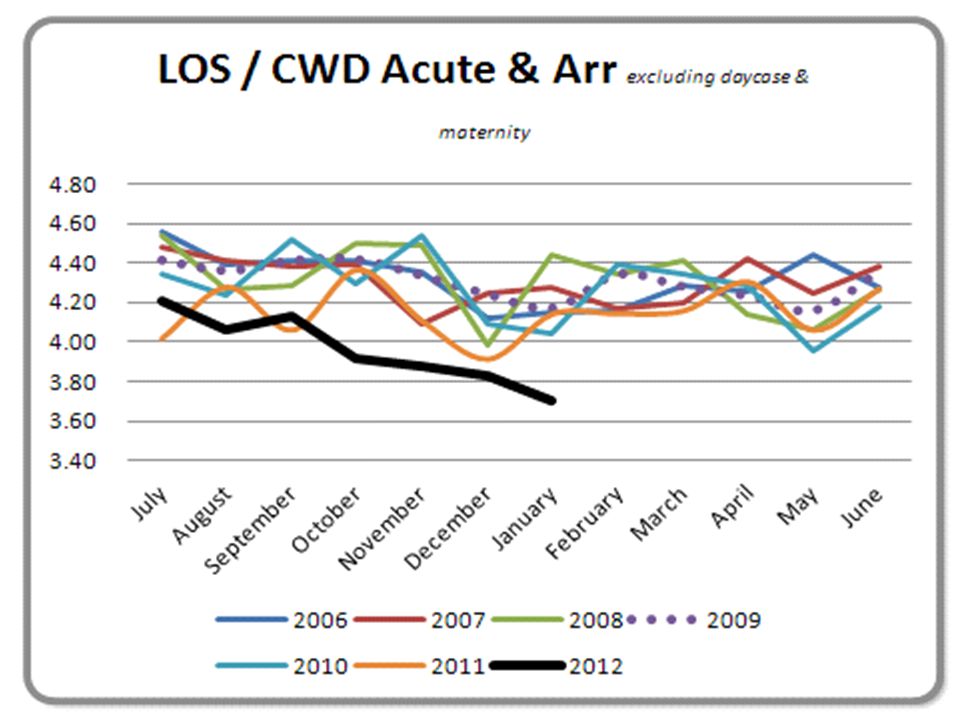
Flow and LOS Initiatives and Impacts EDD on Trendcare and WardView CNS stream in ED Appropriate use of OBS Increased APU capacity with chairs, APU Reg Allied Health Weekend Trial Phlebotomy Rounds earlier Transit lounge surge capacity Acute response by IP teams Red Triangles Ward View Structured Daily Meetings on Ward

30
Nek Minute - VRM Variance Response Management

32
What does Care Capacity Variance look like? There is the capacity available to offer more health care to more people The capacity is about right to efficiently provide quality care which demands reasonable work effort Safe effective care can be provided with extra work effort and some change to how care is organised The ability to provide safe care is at risk. Care is being rationed. Resources are being diverted away from direct care and into service rearrangement Care and safety are being compromised. The system is gridlocked. Resource attention is being directed at the system rather than the care

33
Variance Response Management Matrix MauveGreenYellowOrangeRed Exec. Management Service Leadership/ Ops Management Ward Unit 1.The Variance status (Colours) are defined; MauveExtra capacity GreenCapacity matches demand YellowEarly variance OrangeSignificant care capacity deficit RedCritical care capacity deficit.
 are defined; MauveExtra capacity GreenCapacity matches demand YellowEarly variance OrangeSignificant care capacity deficit RedCritical care capacity deficit..")
35
Ward/Unit Variance Response Action Plan MauveGreenYellowOrangeRed Nursing CNM/Delegate determines plan for the shift and communicates with Duty Manager Expedite discharges: Review EDD for patients’ expected to discharge in next 24hrs. Review patient management plans. Offer staff for period available (e.g. 1 hour, 2 hour, 4 hour, meal relief, full shift). Staff maybe directed to area of greater variance in cluster. Review staffing for next 24hrs. Pull patients in from other areas (e.g. outliers or ED) If staff not required, consider offering annual leave or time in lieu (if owing). Consider quality improvement activities Ensure appropriate timely referrals to Allied Health CNM/Delegate determines plan for the shift and communicates with Duty Manager Expedite discharges: Review EDD for patients’ expected to discharge in next 24hrs. Review patient management plans. Escalate to medical team any patients not seen in last 24hrs. Staff maybe directed to area of greater variance in consultation with Duty Manager. Review staffing for next 24hrs. Consider capacity to ‘pull’ patients in from other areas (e.g. outliers or ED) Consider quality improvement activities Ensure appropriate timely referrals to Allied Health CNM/Delegate determines plan for the shift and communicates with Duty Manager. CNM remains on the unit. Consider reallocating staff to balance skill mix across floor Expedite discharges: Review EDD for patients’ expected to discharge in next 24hrs. Review patient management plans. Escalate to medical team any patients not seen in last 24hrs Repatriation of patients to other facilities. Identify patients who could be put in to the lounge to await discharge. Review staffing for next 24hrs. Reassess status in 1 hour As per Yellow plus: Notifies Duty Manager and requests specific resource eg additional staff or admit stop. CNM take on floor co- ordination role. Consider overtime, extended shifts and/or calling in part time staff. CNM considers utilisation of all staff present e.g. orientation staff and students. Ensure ward/unit MDT are aware of status. Consider notifying Nurse Leader. Put agreed care rationing measures in place including rounding. Compile activity sheets for staff coming to assist for short periods. Ensure patients and on-ward relatives aware of status. Reassess status in 1 hour Complete Reportable Event form (REF) inclusive of Trendcare variance. As per Orange plus: Mandatory reporting to Duty Manager and, Nurse Leader. CNM to arrange for staff to stop all non clinical activities, e.g. cancel staff training. CNM take on floor co- ordination role. Implement “admit stop’ Put ‘life and limb’, agreed care rationing measures in place including rounding. Reassess status in 30 minutes
. Staff maybe directed to area of greater variance in cluster. Review staffing for next 24hrs. Pull patients in from other areas (e.g. outliers or ED) If staff not required, consider offering annual leave or time in lieu (if owing). Consider quality improvement activities Ensure appropriate timely referrals to Allied Health CNM/Delegate determines plan for the shift and communicates with Duty Manager Expedite discharges: Review EDD for patients’ expected to discharge in next 24hrs. Review patient management plans. Escalate to medical team any patients not seen in last 24hrs. Staff maybe directed to area of greater variance in consultation with Duty Manager. Review staffing for next 24hrs. Consider capacity to ‘pull’ patients in from other areas (e.g. outliers or ED) Consider quality improvement activities Ensure appropriate timely referrals to Allied Health CNM/Delegate determines plan for the shift and communicates with Duty Manager. CNM remains on the unit. Consider reallocating staff to balance skill mix across floor Expedite discharges: Review EDD for patients’ expected to discharge in next 24hrs. Review patient management plans. Escalate to medical team any patients not seen in last 24hrs Repatriation of patients to other facilities. Identify patients who could be put in to the lounge to await discharge. Review staffing for next 24hrs. Reassess status in 1 hour As per Yellow plus: Notifies Duty Manager and requests specific resource eg additional staff or admit stop. CNM take on floor co- ordination role. Consider overtime, extended shifts and/or calling in part time staff. CNM considers utilisation of all staff present e.g. orientation staff and students. Ensure ward/unit MDT are aware of status. Consider notifying Nurse Leader. Put agreed care rationing measures in place including rounding. Compile activity sheets for staff coming to assist for short periods. Ensure patients and on-ward relatives aware of status. Reassess status in 1 hour Complete Reportable Event form (REF) inclusive of Trendcare variance. As per Orange plus: Mandatory reporting to Duty Manager and, Nurse Leader. CNM to arrange for staff to stop all non clinical activities, e.g. cancel staff training. CNM take on floor co- ordination role. Implement admit stop’ Put ‘life and limb’, agreed care rationing measures in place including rounding. Reassess status in 30 minutes.")
36
And so how does the IOC relate to the MOH 6 Hr Target…. The IOC provides for a targeted focus on patient flow: Patient flow -variation and constraints on the day When the planets align - 95%!! When they do not – we identify which planet Initiatives are live evidenced Impact of change is monitored live

38
Variance in the Daily 6 Hr Target Performance

42
What enabled the IOC implementation? Having a whole of hospital shared vision Leadership by senior management and clinical leaders Hearing concerns to the fullest and champions addressing them Working hard on awareness across the organisation – social marketing Proactive implementation – whole of hospital

43
Positive Outcomes Organisational ability to learn, and translate into action IOC operational staff report enhanced problem solving - face to face Conversations are informed by Status at a Glance screens - scene setting Silos reduced for operational decision making Working in the “tomorrow” and less surprises today SOPS - shared understanding Variance Response - unified language using the ‘colour’ system Transparency between departments - visual picture of the organisation status Timely Data Entry Developing trust – bridging gaps

44
The Future Hospital Dashboard, Hospital Schedule, Electronic Whiteboards What else would staff find useful? GO TEAM nominated Awards, Making Change that Matters Competition Mechanism to identify Patients at Risk Trendcare Patient Pathways Awaiting VRM audit results

Similar presentations


















>")








>")





 87.7.>")