Download presentation
Presentation is loading. Please wait.

1
AAMR'S IQ-BASED DEFINITION OF MENTAL RETARDATION Mental retardation refers to significantly subaverage general intellectual functioning resulting in or associated with deficits in adaptive behavior and manifested during the developmental period (Grossman, 1983, p. 11). Wsignificantly subaverage general intellectual functioning a score of two or more standard deviations below the mean on a standardized intelligence test (an IQ score of approximately 70 or less) Wdeficits in adaptive behavior inability to meet the standards of personal independence and social responsibility expected of one’s age and social group Wmanifested during the developmental period the concurrent deficits in intellectual functioning and adaptive behavior must occur during the period from birth to age 18 T 6.1 W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved.
. Wsignificantly subaverage general intellectual functioning a score of two or more standard deviations below the mean on a standardized intelligence test (an IQ score of approximately 70 or less) Wdeficits in adaptive behavior inability to meet the standards of personal independence and social responsibility expected of one’s age and social group Wmanifested during the developmental period the concurrent deficits in intellectual functioning and adaptive behavior must occur during the period from birth to age 18 T 6.1 W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved..")
3
INTELLIGENCE TESTING: SOME IMPORTANT CONCERNS AND CONSIDERATIONS WIQ tests can be culturally biased. WIQ scores can change significantly. WIQ testing is not an exact science. WThe concept of intelligence is a hypothetical construct; it is something we infer from observed performance. WThere is nothing mysterious or all-powerful about an IQ test. WAn IQ test measures only how a child performs at one point in time on the items included in one test. We infer from that performance how a child might perform in other situations. WIQ tests have proven to be a good predictor of school achievement. WIn the hands of a competent school psychologist, IQ tests can provide useful information. WResults of an IQ test should never be used as the sole basis for labeling and classifying a child, or for making a decision on the provision or denial special education services. WResults from an IQ test are generally not useful for determining a student's educational objectives or for designing instructional strategies. W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.3

4
ALTERNATIVE DEFINITIONS OF MENTAL RETARDATION behavioral an individual with retardation is one who “has a limited repertoire of behavior shaped by events that constitute his history" (Bijou, 1966) sociological mental retardation is a sociological phenomenon and that the label mental retardation is "an achieved social status in a social system" (Mercer, 1973a) social responsibility mental retardation should be viewed as society's failure to provide sufficient training and education, rather than as a deficit within the individual (Gold, 1980) instructional mental retardation refers to the need for specific training of skills that most people acquire incidentally and that enable individuals to live in the community without supervision (Dever, 1990) All four alternate definitions of mental retardation recognize that: Wmental retardation describes a current level of performance; it is not something a person has such as the measles or red hair Wmental retardation is a relative phenomenon that should not be viewed as a permanent condition Wperformance can often be altered significantly by manipulating certain aspects of the environment (i.e., teaching) W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.4

5
AAMR'S DEFINITION OF MENTAL RETARDATION BASED ON NEEDED SUPPORTS Mental retardation refers to substantial limitations in present functioning. It is characterized by significantly subaverage intellectual functioning, existing concurrently with related limitations in two or more of the following applicable adaptive skill areas: communication, self-care, home living, social skills, community use, self-direction, health and safety, functional academics, leisure, and work. Mental retardation manifests before age 18. The following four assumptions are essential to the application of the definition: 1. Valid assessment considers cultural and linguistic diversity as well as differences in communication and behavioral factors; 2. The existence of limitations in adaptive skills occurs within the context of community environments typical of the individual's age peers and is indexed to the person's individualized needs for supports; 3. Specific adaptive limitations often coexist with strengths in other adaptive skills or other personal capabilities; and 4. With appropriate supports over a sustained period, the life functioning of the person with mental retardation will generally improve. (Luckasson et al., 1992, p. 1) W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.5
 W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.5.")
7
DEFINITIONS OF INTENSITIES OF SUPPORTS FOR INDIVIDUALS WITH MENTAL RETARDATION intermittent Supports on an "as needed basis." Characterized by episodic nature, person not always needing the support(s), or short-term supports needed during life-span transitions. Intermittent supports may be high or low intensity when provided. limited An intensity of supports characterized by consistency over time, time-limited but not of an intermittent nature, may require fewer staff members and less cost than more intense levels of support. extensive Supports characterized by regular involvement (e.g., daily) in at least some environments (such as work or home) and not time-limited. pervasive Supports characterized by their constancy and high intensity; provided across environments; potential life-sustaining nature. Pervasive supports typically involve more staff members and intrusiveness than do extensive or time-limited supports. [Source: From American Association on Mental Retardation, 1992.] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.7
 in at least some environments (such as work or home) and not time-limited. pervasive Supports characterized by their constancy and high intensity; provided across environments; potential life-sustaining nature. Pervasive supports typically involve more staff members and intrusiveness than do extensive or time-limited supports. [Source: From American Association on Mental Retardation, 1992.] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.7.")
8
CAUSES OF MENTAL RETARDATION WMore than 250 causes of mental retardation have been identified. WThe disorders, syndromes, and conditions commonly associated with mental retardation have been categorized by the AAMR according to prenatal (occurring before birth), perinatal (occurring during or shortly after birth), and postnatal causes. WAll of the etiologic factors associated with mental retardation can be classified as either organic (biological or medical) or environmental. WThe cause is unknown for approximately 50% of cases of mild mental retardation and 30% of cases of severe mental retardation. WAll of the known causes of retardation are biological or medical, and these conditions are referred to as clinical mental retardation (brain damage). WWhen no actual organic damage is evident in an individual with mental retardation, the cause is presumed to be psychosocial disadvantage: the combination of a poor social and cultural environment early in the child's life. WAlthough there is no direct proof that social and environmental deprivation causes mental retardation, it is generally believed that these influences cause most cases of mild retardation. W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.8
, perinatal (occurring during or shortly after birth), and postnatal causes. WAll of the etiologic factors associated with mental retardation can be classified as either organic (biological or medical) or environmental. WThe cause is unknown for approximately 50% of cases of mild mental retardation and 30% of cases of severe mental retardation. WAll of the known causes of retardation are biological or medical, and these conditions are referred to as clinical mental retardation (brain damage). WWhen no actual organic damage is evident in an individual with mental retardation, the cause is presumed to be psychosocial disadvantage: the combination of a poor social and cultural environment early in the child s life. WAlthough there is no direct proof that social and environmental deprivation causes mental retardation, it is generally believed that these influences cause most cases of mild retardation. W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.8.")
9
DISORDERS IN WHICH MENTAL RETARDATION MAY OCCUR I. Prenatal Causes A. Chromosomal disorders (e.g., Trisomy 21 [Down syndrome]) B. Syndrome disorders (e.g., Prader-Willi syndrome) C. Inborn errors of metabolism (e.g., phenylketonuria [PKU]) D. Developmental disorders of brain formation (e.g., hydrocephalus) E. Environmental influences (e.g., fetal alcohol syndrome) II. Perinatal Causes A. Intrauterine disorders (e.g., premature delivery) B. Neonatal disorders (e.g., head trauma at birth) III. Postnatal Causes A. Head injuries (e.g., cerebral concussion) B. Infections (e.g., encephalitis) C. Demyelinating disorders (e.g., postinfectious disorders) D.Degenerative disorders (e.g., Rett syndrome) E. Seizure disorders (e.g., epilepsy) F. Toxic-metabolic disorders (e.g., lead or mercury poisoning) G. Malnutrition (e.g., protein-calorie malnutrition) H. Environmental deprivation (e.g., psychosocial disadvantage) I. Hypoconnection syndrome [Source: From American Association on Mental Retardation, 1992.] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.9
 B. Syndrome disorders (e.g., Prader-Willi syndrome) C. Inborn errors of metabolism (e.g., phenylketonuria [PKU]) D. Developmental disorders of brain formation (e.g., hydrocephalus) E. Environmental influences (e.g., fetal alcohol syndrome) II. Perinatal Causes A. Intrauterine disorders (e.g., premature delivery) B. Neonatal disorders (e.g., head trauma at birth) III. Postnatal Causes A. Head injuries (e.g., cerebral concussion) B. Infections (e.g., encephalitis) C. Demyelinating disorders (e.g., postinfectious disorders) D.Degenerative disorders (e.g., Rett syndrome) E. Seizure disorders (e.g., epilepsy) F. Toxic-metabolic disorders (e.g., lead or mercury poisoning) G. Malnutrition (e.g., protein-calorie malnutrition) H. Environmental deprivation (e.g., psychosocial disadvantage) I. Hypoconnection syndrome [Source: From American Association on Mental Retardation, 1992.] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.9.")
11
COMMON FEATURES OF TEACHING METHODS DERIVED FROM APPLIED BEHAVIOR ANALYSIS 1.Precise definition and task analysis of the new skill or behavior to be learned 2.Direct and frequent measurement of the student's performance of the skill 3.Frequent opportunities for active student response during instruction 4.Immediate and systematic feedback for student performance. 5.Procedures for achieving the transfer of stimulus control from instructional cues or prompts to naturally occurring stimuli 6.Strategies for promoting the generalization and maintenance of newly learned skills to different, nontraining situations and environments W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.11

12
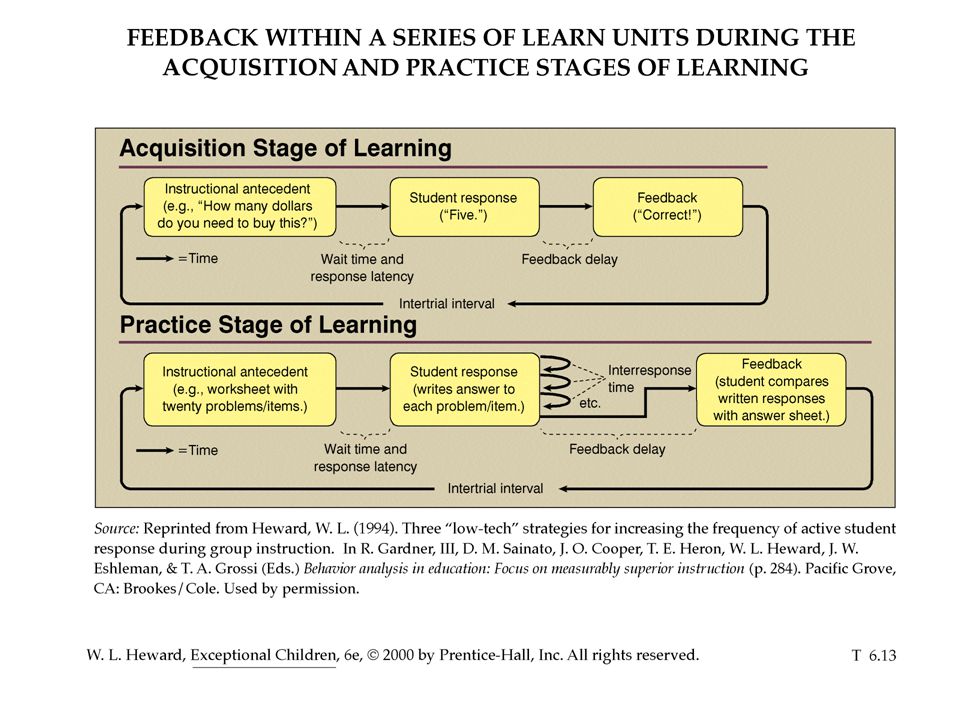
ACTIVE STUDENT RESPONSE (ASR) Active student response (ASR) occurs when a student emits a detectable response to ongoing instruction. T The kinds of responses that qualify as ASR are as varied as the kinds of lessons that are taught (e.g., words read, problems answered, test tubes measured, praise and supportive comments spoken, notes or scales played, sentences written, workbook questions answered, fastballs pitched). T The basic measure of how much ASR a student experiences is a frequency count of the number of academic responses emitted within a given period of instruction. An ASR-rich lesson will generally result in more learning than a lesson in which students make few or any responses. Instructional methods characterized by high rates of ASR include: T Choral responding T Response cards T Guided notes T Repeated reading T Fluency-building activities such as time-trials T Peer tutoring T Computer-assisted instruction T Direct Instruction [Source: From W. L. Heward, 1994] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.12
. T The basic measure of how much ASR a student experiences is a frequency count of the number of academic responses emitted within a given period of instruction. An ASR-rich lesson will generally result in more learning than a lesson in which students make few or any responses. Instructional methods characterized by high rates of ASR include: T Choral responding T Response cards T Guided notes T Repeated reading T Fluency-building activities such as time-trials T Peer tutoring T Computer-assisted instruction T Direct Instruction [Source: From W. L. Heward, 1994] W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T")
14
FOUR STRATEGIES FOR PROMOTING THE GENERALIZATION AND MAINTENANCE OF NEW SKILLS AND KNOWLEDGE Aim for naturally occurring contingencies of reinforcement This can be accomplished by (a) teaching only functional skills that are needed and likely to be valued by people in the natural environment and (b) teaching students to perform new skills with enough accuracy and fluency necessary to produce reinforcement in the natural environment. Use a general case strategy to select teaching examples Instructional examples that systematically represent the response requirements and stimulus variations found in the natural environment should be selected and incorporated into lessons. Program common stimuli is accomplished by (a) incorporating into the teaching situation as many typical features of the generalization setting as possible and/or (b) creating a new common stimulus that the student learns to use in the teaching setting and that is transportable to the generalization setting, where it prompts or assists performance of the target skill. Teach self-management skills The only person who is with the learner at all times and in all places is the learner's own self. Students can use self-management skills to promote the generalization and maintenance of their new knowledge and skills. W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 6.14
 incorporating into the teaching situation as many typical features of the generalization setting as possible and/or (b) creating a new common stimulus that the student learns to use in the teaching setting and that is transportable to the generalization setting, where it prompts or assists performance of the target skill. Teach self-management skills The only person who is with the learner at all times and in all places is the learner s own self. Students can use self-management skills to promote the generalization and maintenance of their new knowledge and skills. W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T")
Similar presentations








 Marc J. Tassé, PhD Director, Nisonger Center - UCEDD Professor,>")



 Allyn & Bacon 2004Copyright © Allyn and Bacon 2004 Chapter Eight Teaching Students with Mental Retardation This multimedia product and its contents.>")





 Multiple disabilities means concomitant impairments, the combination of which causes such severe.>")



>")