Download presentation
Presentation is loading. Please wait.

1
Preventative Care for the Throwing Athlete Scott Sheridan, MS PT ATC CSCS Head Athletic Trainer The Phillies

2
Youth Injuries - Data 3.5 million kids under age of 14 receive medical treatment for sports injuries each year 62% of injuries occur in practice, but same precautions are not put in place in practice as they are in games. By age 13, 70% of kids drop out of youth sports, The top three reasons: adults, coaches, parents

3
Youth Injuries - Data Among athletes 5 to 14 years of age, 25% of baseball players were injured while playing there sport Since 2000 there has been a fivefold increase in the number of serious shoulder and elbow injuries in youth baseball and softball False: Players do not come back stronger and throwing harder after Tommy John Surgery!! More than 50% of all sports injuries in children are preventable

4
Definition of Prevention Primary – avoids the development of disease Secondary – early disease detection Tertiary – reduces impact on already existing condition Want to detect problems as early as possible

5
Things We Can Not Prevent Genetics Quality of Tissue?

6
What is Happening Biomechanically with Throwing a Ball Not a “Normal” Act Calculated stress with throwing exceeds the load to failure of the native ligament. Flexor Muscle – Intimately attached to UCL, assist w/ stability Extensors - Increase ESM activation and Decrease FPM activation in injured pitchers during acceleration**

7
Muscular Fatigue - Biomechanics EMG Activity with Pitching (% of Max Muscle Test) Early Cocking – Upper Trap (64%), Supraspinatus(60%) Late Cocking – Serratus Anterior (106%), Subscapulairs (99%), Levator (72%), Infraspinatus (74%), Extensor Carpi Radialis (72%), Extensor Carpi Radialis Brevis (75%) Acceleration – Lower Trap (76%), Levator (77%),Subscapularis (115%), Latissimus (88%), Tricep (89%), Pronator Teres (85%), Flexor Carpi Radialis (120%), Flex Dig Superficialis (80%), Flexor Carpi Ulnaris (112%) Deceleration – Lower Trap (78%), Teres Minor (84%), Flexor Carpi Radialis (79%), Flexor Carpi Ulnaris (77%) Follow Through – All less than 42% DiGiovine et al.- J Sh and Elbow 1992
 Early Cocking – Upper Trap (64%), Supraspinatus(60%) Late Cocking – Serratus Anterior (106%), Subscapulairs (99%), Levator (72%), Infraspinatus (74%), Extensor Carpi Radialis (72%), Extensor Carpi Radialis Brevis (75%) Acceleration – Lower Trap (76%), Levator (77%),Subscapularis (115%), Latissimus (88%), Tricep (89%), Pronator Teres (85%), Flexor Carpi Radialis (120%), Flex Dig Superficialis (80%), Flexor Carpi Ulnaris (112%) Deceleration – Lower Trap (78%), Teres Minor (84%), Flexor Carpi Radialis (79%), Flexor Carpi Ulnaris (77%) Follow Through – All less than 42% DiGiovine et al.- J Sh and Elbow 1992")
8
“Not the Reaction You Want!”

9
How Do We Prevent Injuries? Screenings / Pre Participation Examinations Importance of the Active Warm Up Gradual / Appropriate Progression of Activity / Conditioning Understand What to Do When an Injury Occurs!

10
Screening The purpose of the screening is to create a list of dysfunctions. Ultimately the goal is to provide the throwing athlete the best possible anatomical and physiological base to achieve throwing efficiency.

11
Types of Examinations Medical History / Questionnaire Information Gathering Communication

12
Types of Examinations Functional Movement Screen Performed by Athletic Trainer / Physical Therapist Objective is to identify limitations / asymmetry Restrictions / Imbalances will distort motor learning, movement perception, body awareness, and mechanics

13
Deep Squat

14
Hurdle Step

15
In Line Lunge

16
Shoulder Mobility

17
Active Straight Leg Raise

18
Trunk Stability Pushup

19
Rotary Stability

20
Types of Examinations Orthopedic Shoulder Range of Motion Strength Special Testing Posture Scapular Assessment Spinal Assessment Lower Extremity Hip Range of Motion Changes

21
Shoulder Examination Range of Motion Decreased Internal Rotation (GIRD), increase posterior capsule thickness with throwing Change in Total ROM (IR + ER) Humeral Retroversion (maintain what given at birth on dominant / throwing side)
, increase posterior capsule thickness with throwing Change in Total ROM (IR + ER) Humeral Retroversion (maintain what given at birth on dominant / throwing side)")
22
Posture Assessment Areas to Evaluate Forward Head Forward Shoulder Coracoid Antecubital Fossa TS – Kyphosis, Flat, Scoliosis LS – Flat, Lordotic Shoulder Position Inferior Ang. Mid-Thorax

23
Scapular Assessment Shoulder pain is the result of movement impairment of the scapula, that disrupts relationship of glenoid and the humerus

24
Scapular Assessment

25
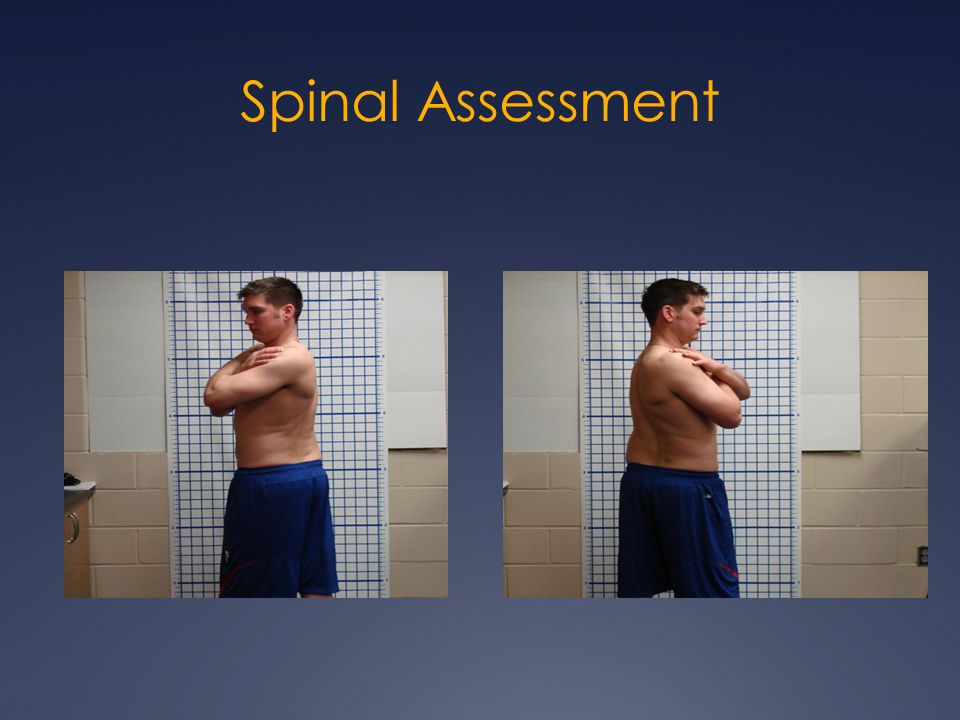
Spinal Assessment

27
Lower Extremity

28
Why Evaluate All These Areas? Kinetic Chain Progression Core is active with any movement Velocity most directly correlated with Lower extremity strength Exercise in manner that they will be used (functional) FORCE GENERATION LEGS TRUNK / BACK SHOULDER ELBOW WRIST
 FORCE GENERATION LEGS TRUNK / BACK SHOULDER ELBOW WRIST.")
29
The Injury “Cause List” Range of Motion Changes Reinold et al – AJSM 2008; decrease in sh. IR, total motion, and elbow extension immediately after, lasting 24 hours Scapular Dyskinesis (Kibler) Muscular Fatigue(shoulder, scap, forearm)* Core Stability Spinal Mobility (wind up vs. follow through) Limitations in the Lower Body (opening up?)
 Muscular Fatigue(shoulder, scap, forearm)* Core Stability Spinal Mobility (wind up vs. follow through) Limitations in the Lower Body (opening up ).")
30
Importance of Active Warm Up Should always be the first thing that is done before practice or game. Not just a static stretching program. Developed to address consistent concerns found during screening process. Should be sweating after completing.

31
Gradual and Appropriate Progression of Activity / Conditioning Equipment Weekly Inspections Hitting Progressions Indoor, Tee, # of Swings Throwing Programs Long Toss – Distance? Types of Exercises

32
What to do if an injury occurs? Symptoms are present for a reason. Do not let a minor problem progress into a major problem. Remember types of prevention! Compensations will occur Seek appropriate medical advice Orthopedist, Physical Therapist, Athletic Trainer @ School

33
Red Flag Symptoms Elbow Medial Elbow Pain Ulnar Nerve Symptoms Shoulder Deltoid Soreness Posterior Shoulder Pain Performance Concerns Control and Velocity Duration of Symptoms Sore During – Sore After – Sore Next Day

34
“Don’t Bring Me a Problem, Bring Me a Solution!” ① Pre Participation Exam / Screening ② Warm Up Appropriately ③ Do Not Pitch Through Symptoms ④ Do Not Play Year-Round ⑤ Communicate to players regarding how they are feeling ⑥ Emphasize, control, accuracy, and age appropriate skills ⑦ Speak to a medical professional if you have concerns about an injury or to develop a prevention strategy.

35
Special Thank You - Acknowledgement Kinetic Rehab Phil Donley, MS PT ATC Jeff Cooper, MS ATC Gray Cook, PT Gary Gray, PT Craig Morgan, MD Shirley Sahrmann Ron Hruska

36
Questions / Solutions

Similar presentations














>")




