Download presentation
Presentation is loading. Please wait.

1
Dr. Fatin Awartani

2
Width of AG differs in different areas of the mouth. Greatest in the incisor region (3.5-4.5 mm in the max, 3.3-3.9 mm in the man). Least width in the 1 st premolar area (1.9 mm in the max, 1.8 mm in the man) Anatomy Dr. Fatin Awartani
. Least width in the 1 st premolar area (1.9 mm in the max, 1.8 mm in the man) Anatomy Dr. Fatin Awartani.")
3
Literature Review No standard width of keratinized attached gingiva has been established. In people with good oral hygiene 1 mm or less may be sufficient for health (Lang and loe, 1972; Dorfman et al., 1980). Kirch et al (1986) and Wennstrom (1987) have shown that even a movable marginal tissue of alveolar mucosa can be maintained stable over a long period of time Dr. Fatin Awartani
. Kirch et al (1986) and Wennstrom (1987) have shown that even a movable marginal tissue of alveolar mucosa can be maintained stable over a long period of time Dr. Fatin Awartani.")
4
Trauma of prosthetic treatment (Maynard and Wilson, 1979; Ericsson and Lindhe, 1984) Orthodontic restoration (Maynard and Ochsenbein, 1975; Coatoam et al., 1981) Frenulum pull (Gottsgen, 1954; Gorman, 1967) Rapidly progressing recession (Baker and Seymour, 1976) Literature Review Dr. Fatin Awartani

5
Tissue barrier concept: Goldman and Cohen (1979) outlined a “tissue barrier” concept They postulated that a dense collagenous band of CT retards or obstructs the spread of inflammation better than does the loose fiber arrangement of the alveolar mucosa. They recommended increasing the zone of keratinized attached gingiva tissue to achieve an adequate tissue barrier (thick tissue). Literature Review Dr. Fatin Awartani
. Literature Review Dr. Fatin Awartani.")
6
Literature Review Wennstrom (1985) states,”A thin marginal tissue, in particular in the absence of underlying alveolar bone, will be at greater risk of recession since the plaque-induced inflammatory lesion may occupy and cause destruction of the entire CT portion of the gingiva” Dr. Fatin Awartani

7
Widening the attached gingiva accomplishes the following objectives: 1. Enhances plaque removal around the gingival margin. 2. Improve esthetics 3. Reduces inflammation around restored teeth. Dr. Fatin Awartani

8
Techniques to Increase Keratinized Attached Gingiva Widening the of the keratinized attached gingiva (apical or coronal to area of recession) can be accomplished by many techniques: Free gingival auto graft Free connective tissue graft Lateral pedicle flap Apically displaced flap Dr. Fatin Awartani

9
Free Gingival Graft Advantages 1- High degree of predictability 2- Simplicity 3- Ability to treat multiple teeth at the same time 4- Can be preformed when keratinized gingiva adjacent to the involved area is insufficient 5- As the first step in a two-stage procedure for attaining root coverage 6- As a single step for attaining root coverage Dr. Fatin Awartani

10
Disadvantages 1- Two operative sites 2- Compromised blood supply 3- Greater discomfort 4- Poor hemostasis 5- Retention of graft Free Gingival Graft Dr. Fatin Awartani

11
Factors: 1- Graft thickness (1.5 mm to 2 mm is recommended) 2- Suturing techniques 3- Entrapment of a blood clot between the graft and the roots, as well as the adjacent soft tissue recipient bed 4- Mechanical root preparation (Sc/Rp) 5- Flattening of the root surface with Sc and Rp or rotary instrumentation 6- Chemical root conditioning (citric acid and tetracycline) Free Gingival Graft Dr. Fatin Awartani

12
Contraindications 1- A perceptible mismatch in color between donor site and gingiva adjacent to recipient site 2- A lack of thick donor tissue 3- A class III or class IV recession defect 4- A root surface of excessive mesiodistal width coupled with interproximal tissue that is too narrow to support the blood supply Free Gingival Graft Dr. Fatin Awartani

14
Free Gingival Graft Common reasons for graft failure: use of root coverage (prominent roots, wide areas of root exposure) proper graft adaptation adequate transfusion of the graft graft movement (plasmatic diffusion) Dr. Fatin Awartani

15
Subepithelial Connective Tissue Graft Advantages 1- It is predictable for obtaining root coverage 2- The technique results in good gingival color match 3- The palatal donor site is less prone to bleeding, and healing is easier than FGG 4- The double blood supply created in this approach is advantageous 5- The surgeon’s ability to control the thickness is greater than is possible with the FGG Dr. Fatin Awartani

16
Indications 1- A lack of adequate donor tissue for a lateral sliding flap 2- The presence of root recession 3- The presence of isolated wide recession 4- The presence of multiple root recession 5- The presence of recession adjacent to an edentulous area requiring ridge augmentation 6- The presence of recession in an area where esthetics is often great concern Subepithelial Connective Tissue Graft Dr. Fatin Awartani

17
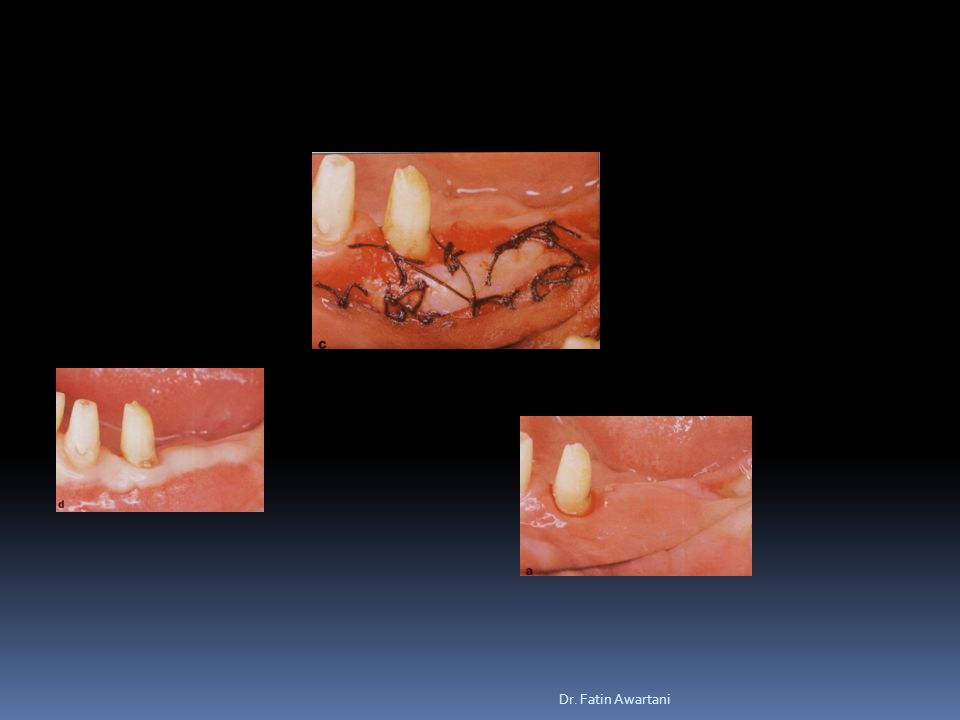
Before Sub epithelial CT After Dr. Fatin Awartani

22
Laterally Positioned Pedicle Graft Advantages: 1- One surgical site 2- Good vascularity of the pedicle flap 3- Ability to cover a denuded root surface Disadvantages: 1- Limited by the amount of adjacent keratinized attached gingiva 2- Possibility of recession at the donor site 3- Dehiscence or fenestration at donor site 4- limited to one or two teeth Dr. Fatin Awartani

23
Contraindications: 1- Presence of deep interproximal pockets 2- Excessive root prominence 3- Deep or extensive root abrasion or erosion 4- Significant loss of interproximal bone height Laterally Positioned Pedicle Graft Dr. Fatin Awartani

25
Apically displaced flap Dr. Fatin Awartani

26
Flap apically displace and sutured Before After Dr. Fatin Awartani

Similar presentations







 placement>")




>")











