Download presentation
Presentation is loading. Please wait.

1
TARRSON FAMILY ENDOWED CHAIR IN PERIODONTICS

2
UCLA SCHOOL OF DENTISTRY

3
Presents Presents Dr. E. Barrie Kenney Professor & Chairman Section of Periodontics

4
Surgical Techniques for Crown Lengthening
E. Barrie Kenney B.D.Sc., D.D.S., M.S., F.R.A.C.D.S. Surgical Techniques for Crown Lengthening Tarrson Family Endowed Chair in Periodontics. Professor and Chairman Division of Associated Clinical Specialties UCLA School of Dentistry

5
Indications for Crown Lengthening
Development of Adequate Crown Preparation Esthetics Indications for Crown Lengthening

6
Development of Adequate Crown Preparation
Gingival Margins must not invade Biological Width Requirements for Periodontal Health. Development of Adequate Crown Preparation

7
Biological Width Requirements
There must be a minimum of 1mm between the apical level of the Junctional Epithelium and the bone crest. Biological Width Requirements

8
Crown Margins which extend apically beyond the Junctional Epithelium can violate the requirements for periodontal health. An inappropriate crown margin increases plaque accumulation in close proximity to bone crest.

9
Deeply placed crown margins causing gingival inflammation and pockets.

10
Both Central Incisors and right lateral incisor have crowns violating Biologic Width concepts.

11
Gargiulo A., Wentz F., Orban F.
Dimensions and Relations of the Dentogingival Junction in Humans. J. Periodontol :261 This study measured dimensions of tissues involved in Biological Width considerations.

12
Used histologic sections to measure average dimensions of biologic width.
These are not clinically accurate due to distortion with histologic processing.

13
Gingival sulcus Junctional epithelium Connection tissue attachment coronal to bone Sulcus depth 0.69 mm 0.97 mm 1.07 mm This study said width of junctional epithelium plus connective tissue width was Biologic width; i.e. approximately 2 mm. Biologic Width

14
However since then it has been shown that in probing the sulcus, the probe is generally at the deepest position of junctional epithelium.

15
If a subgingival crown margin is placed in the middle of the gingival sulcus, the crest of bone should be a minimum of 2 mm apically positioned.

16
When a subgingival crown margin is to be placed it may be necessary to surgically move the crestal bone margin apically so that there is at least 2 mm space between the margin and the bone. The necessary for 1 mm of connective tissue between the epithelium and bone is a minimal requirement. Larger dimensions can be compatible with healthy tissues.

17
Use of Flap Surgery with Osseous Resection
This is the method of choice when crown margins will impinge on the Biologic Width. Use of Flap Surgery with Osseous Resection

18
Periapical Radiographs are needed to ensure sufficient root length is available. This case cannot have surgical crown lengthening and both premolars need to be extracted.

19
This patient had extensive tooth wear and loss of Vertical Dimension

20
There was insufficient clinical crown volume of the incisors for adequate retention so flap surgery was indicated.

22
Prior to Flap Surgery

23
Full thickness labial and lingual flaps .

24
Bone is recontoured so that 2 mm distance between level of proposed crown margin and crest of bone.

25
The lingual side required minimal bone surgery.

26
Flaps are positioned apically to increase length of clinical crowns.

27
Similar apical positioning on Lingual.

28
Crown preparations 12 weeks after crown lengthening surgery.

29
Final upper and lower restorations.

30
Before After

31
Inadequate clinical crowns for retention of new restorations.

33
Flap design on buccal. Intrasulcular incisions, mesial vertical incision, distal wedge.

34
Flap design on palatal. Reverse bevel incision removing gingival margin ,mesial vertical incision, distal wedge.

36
Buccal full thickness flap elevation to expose at least 3 mm of crestal bone.

37
Palatal flap elevation to expose at least 3 mm of crestal bone.

38
The gingival level of new crown margin is estimated and bone removed so crestal level is 2 mm apical to this.

39
Buccal crown margins will be subgingival for esthetics
Buccal crown margins will be subgingival for esthetics. So margins will be in middle of gingival sulcus i.e. 1 mm coronal to probing depth, add another 1 mm for connective tissue to determine bone level.

40
Palatal crown margin will be supragingival
Palatal crown margin will be supragingival. So allow 1mm for connective tissue plus 2 to 3 mm for sulcus with bone level 3 to 4 mm apical to level of crown margin.

41
Buccal flap sutured apically with increased tooth structure for crown preparation.

42
Palatal flap repositioned with continuous sling mattress sutures and simple U shaped sutures of distal wedge and vertical incisions.

43
Buccal Healing at 3 weeks.

44
Palatal Healing at 3 weeks.

45
Crowns placed at 6 weeks.

46
After Before

47
After Before

48
Gingivectomy for Crown Lengthening
Most cases need flap and osseous surgery. Gingivectomy used when have adequate band of Keratinized tissue and bone crest is positioned apically with an initial wide Biological Width. Gingivectomy for Crown Lengthening

49
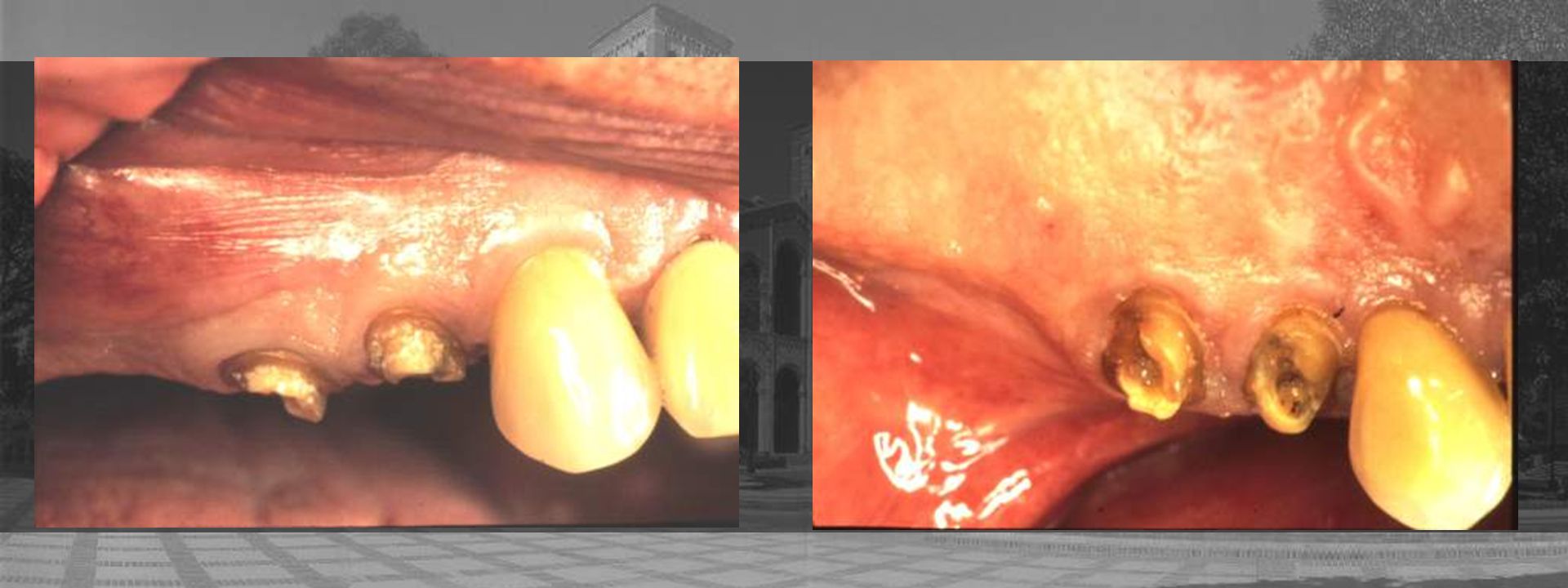
Poor crowns with recurrent caries.

50
Soft tissue removal will be adequate for exposure of sound tooth for margins with a 1 mm Ferrule Extension.

51
Electrosurgery used for gingivectomy
Electrosurgery used for gingivectomy. This can also be done with scalpels or laser.

52
Tissue recontoured to expose root surfaces for adequate preparation of margins.

53
Provisional restorations at 12 weeks
Provisional restorations at 12 weeks. Marginal gingiva is now stable so final subgingival crowns can be completed.

54
Final crown restorations should not be completed until a minimum of 6 weeks after surgery in order to minimized further tissue loss due to trauma of impressions. In esthetic areas a minimum of 12 weeks after-surgery is required to be sure no further gingival recession will occur.

Similar presentations




 placement>")

.>")






>")







