Download presentation
Presentation is loading. Please wait.

1
APPROACH TO CHRONIC COUGH
DIAGNOSIS & MANAGEMENT

2
COUGH One of the most common symptoms for which patients seek medical attention Defensive reflex that enhance the clearance of secretions and particles from the airway Protects the lower airways from the aspiration of foreign materials

3
Coughing may be initiated either voluntarily or reflexively.
It has both afferent and efferent pathways . The cough starts with a deep inspiration followed by glottic closure, relaxation of the diaphragm, and muscle contraction against a closed glottis.

4
Classification Acute cough Subacute cough Chronic Cough ~ 3 to 8 weeks
~ maximum of 3 weeks Subacute cough ~ 3 to 8 weeks Chronic Cough ~ more than 8 weeks Classification of cough based on symptom duration is somewhat arbitrary Acute cough (<3 weeks) Is most often due to upper respiratory infection (common cold, acute bacterial sinusitis, and pertussis), serious disorders, such as pneumonia, pulmonary embolus, and congestive heart failure, can also present in this fashion. Sub acute cough (between 3 and 8 weeks) Is commonly post-infectious, resulting from persistent airway inflammation and/or postnasal drip following viral infection, pertussis, or infection with Mycoplasma or Chlamydia. Chronic cough (>8 weeks) In a smoker raises the possibilities of asthma, COPD or bronchogenic carcinoma, Eosinophilic Bronchitis , Esophageal Disease, Post Nasal Drip , ACEI , Smoking. De Blasio et al. Cough 2011, 7:7
 Is most often due to upper respiratory infection (common cold, acute bacterial sinusitis, and pertussis), serious disorders, such as pneumonia, pulmonary embolus, and congestive heart failure, can also present in this fashion. Sub acute cough (between 3 and 8 weeks) Is commonly post-infectious, resulting from persistent airway inflammation and/or postnasal drip following viral infection, pertussis, or infection with Mycoplasma or Chlamydia. Chronic cough (>8 weeks) In a smoker raises the possibilities of asthma, COPD or bronchogenic carcinoma, Eosinophilic Bronchitis , Esophageal Disease, Post Nasal Drip , ACEI , Smoking. De Blasio et al. Cough 2011, 7:7.")
5
ETIOLOGY Acute cough ~ maximum of 3 weeks Upper Respiratory Infection (common cold, acute bacterial sinusitis, and pertussis) Pneumonia Pulmonary embolus Congestive cardiac failure Subacute cough ~ 3 to 8 weeks Post-infectious Postnasal drip following viral infection, Pertussis Tuberculosis Mycoplasma or Chlamydia infection Chronic Cough ~ more than 8 weeks Asthma COPD Bronchogenic carcinoma Eosinophilic Bronchitis Esophageal Disease, Post Nasal Drip ACEI Smoking.

6
Chronic Cough- Etiology
In non-smoking adults with a normal CXR who are not taking ACE inhibitors, chronic cough is almost always due to which of the following 3 conditions? Congestive Heart Failure Upper Airway Cough Syndrome (UACS) c) Asthma d) Gastroesophageal reflux disease (GERD) e) Chronic Bronchitis
 c) Asthma. d) Gastroesophageal reflux disease (GERD) e) Chronic Bronchitis.")
7
Etiology

8
Chronic cough sometimes can have more than 1 cause
Smyrnios et al Arch Intern Med :1222 3

10
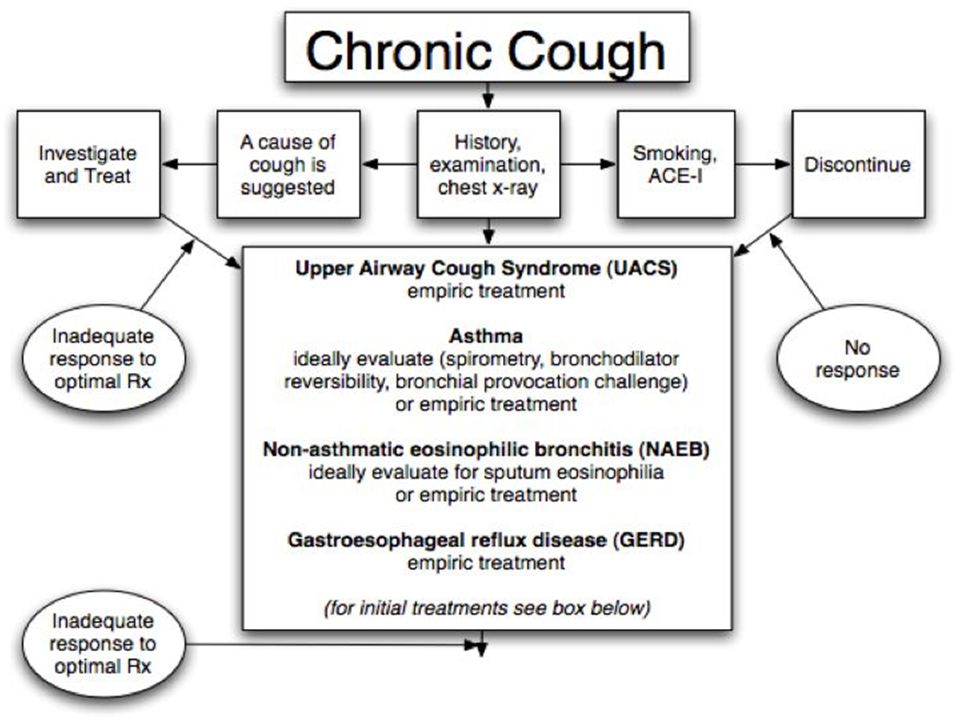
Guideline for Evaluating Chronic Cough
• A systematic, diagnostic approach has been validated in immunocompetent patients- 5 steps plan: Step 1: Review history and exam focusing on the most common causes of chronic cough

11
History taking History Reasons Onset
To determine acute/subacute or chronic causes of cough Aggravating factor, relieving factor Cough due to GERD affected by postural changes, post meal Cold induced or MDI relieved cough in asthma or COPD Sputum colour Normal sputum: clear to white colour, thin, odourless n tasteless Yellow-green: bacterial infection Rust-colored: pneumonia Sputum character Mucoid or mucopurulent: cigarette smokers as a result of chronic bronchitis Commonly purulent in bronchiestasis Sputum amount Significant volumes: more than 1 cup per day

12
Wheezing suggest asthma/COPD
History Reasons Fever Ongoing infection SOB Respiratory distress Noisy breathing Wheezing suggest asthma/COPD Loss of appetite, loss of weight, hemoptysis Suggesting Tuberculosis, malignancy Allergy, nasal obstruction or congestion, rhinorrhoea, sneezing, facial pain, post-nasal drip or repetitive throat clearance Suggesting Rhinosinusitis Dyspepsia, heartburn, waterbrash GERD Medication used ACE-inhibitor Occupation Exposure to asbestos, chemical or cigarette smoke Family history Asthma, tuberculosis, lung cancer, cystic fibrosis Social history Contact with PTB suggesting PTB Reflux: usually caused by transient relaxation of low esophageal sphincter. Thus, relaxation cough may occur after meal, during meal, supine, bending or stooping position : diminish at sleep (LOS closed) but recur on adopting an upright position : talking, laughing may precipitate reflux cough (diaphragm important component of LOS) Dyspnoea, wheezing n chest tightness suggest asthma but can be absent in CVA -variability from day to day and nocturnal exacerbation suggestive Pharyngeal sm: rhinosinusitis : many of these sm also occur in reflux disease. GERD may be suggested by presence of classic sm – dyspepsia, heartburn, water brash ACE-I :< 15% patient on ACE-I develop dry cough soon after commencement : usially disappear after cessation of tx but resolution may takes several months, may persists in small minority.
 but recur on adopting an upright position. : talking, laughing may precipitate reflux cough (diaphragm important component of LOS) Dyspnoea, wheezing n chest tightness suggest asthma but can be absent in CVA. -variability from day to day and nocturnal exacerbation suggestive. Pharyngeal sm: rhinosinusitis. : many of these sm also occur in reflux disease. GERD may be suggested by presence of classic sm – dyspepsia, heartburn, water brash. ACE-I :< 15% patient on ACE-I develop dry cough soon after commencement. : usially disappear after cessation of tx but resolution may takes several months, may persists in small minority.")
13
Physical Examination Physical examination Reasons
General condition such as altered conscious level, accessory muscles usage, cyanosis, grunting, nasal flaring, clubbing, nicotine stain To assess severity and to look for respiratory distress Vital signs Fever – infection Tachycardia, tachypnoea – respiratory distress Pulsus paradoxus – asthma Nasal polyps Allergy rhinitis Pharynx: erythema, a cobblestone appearance of posterior pharyngeal mucosa or mucoid secretions dripping from the nasopharynx Post nasal drip Chest: Hyperinflated Recession Silent chest Crepitations, wheezing Suggest air trapping due to chronic disease Respiratory distress Severe asthma Pneumonia, asthma, heart failure

14
Physical examination Reasons CVS: Displaced apex beat, raised JVP, loud P2, RV heave Cor pumonale Eczema, transverse nasal crease, injected conjunctiva Signs of atopic disease Lymphadenopathy To suggest infection Abnormal physical signs are rare in a chronic dry cough Wheeze may be audible on examination but is usually absent in cough variant asthma (CVA)
")
15
Guideline for Evaluating Chronic Cough
Step 2: Order a CXR in all patients Step 3: Do not order additional tests in present smokers or patients taking ACE inhibitors until the response to smoking cessation or drug discontinuation for at least 4 weeks can be assessed. - Cough due to smoking or ACE inhibitors should improve substantially or disappear during this time- frame of abstinence. Step 4: Order additional diagnostic tests or embark on empiric treatment

16
Investigations Spirometry:
-demonstrate significant airway reversibility (asthma) -unavailable or normal and history suggestive: serial measurement of PEF (diurnal variability) Bronchoprovocation test : - negative: rules out asthma but does not rules out steroid- responsive cough Plain sinus radiography: low specificity but improves with history and findings Sputum eosinophilia Cxr mandatory a early stage as is significant abnormality will alter the diagnostic algorithm and avoid unnecessary Ix. Spirometry : before and after inhaled bronchodilator Bronchoscopy: Suspected FB, CXR showing mass, pulmonary, lobar or segmental collapse, hemoptysis, recurrent pneumonia in the same area Fibreoptic bronchoscopy – biopsy High Resolution CT scan: lung parenchymal disease or bronchiectasis (not appreciated from hx and CXR)
 -unavailable or normal and history suggestive: serial. measurement of PEF (diurnal variability) Bronchoprovocation test : - negative: rules out asthma but does not rules out. steroid- responsive cough. Plain sinus radiography: low specificity but improves with history and findings. Sputum eosinophilia. Cxr mandatory a early stage as is significant abnormality will alter the diagnostic algorithm and avoid unnecessary Ix. Spirometry : before and after inhaled bronchodilator. Bronchoscopy: Suspected FB, CXR showing mass, pulmonary, lobar or segmental collapse, hemoptysis, recurrent pneumonia in the same area. Fibreoptic bronchoscopy – biopsy. High Resolution CT scan: lung parenchymal disease or bronchiectasis (not appreciated from hx and CXR)")
17
SPIROMETRY NORMAL OBSTRUCTIVE RESTRICTIVE

18
SPIROMETRY

19
SPIROMETRY

20
Guideline for Evaluating Chronic Cough
Step 5: Determine the cause(s) of cough by observing which specific therapy eliminates cough • If the evaluation suggests more than one possible cause, initiate treatment in the same sequence that the abnormalities were discovered • Since cough can be simultaneously caused by more than one condition, do NOT stop therapy that appears to be partially successful; rather, sequentially add to it.
 of cough by observing which specific therapy eliminates cough • If the evaluation suggests more than one possible cause, initiate treatment in the same sequence that the abnormalities were discovered • Since cough can be simultaneously caused by more than one condition, do NOT stop therapy that appears to be partially successful; rather, sequentially add to it.")
21
Case Scenario 1 55 yo school teacher c/o cough for 3 years Non-smoker
Cough: Often productive Better with abx, but comes back “no better” with asthma meds Worst in the morning Frequent clearing the throat, sensation of dripping into throat

22
Case Scenario 1 Nasal voice, afebrile, looks well
Pharynx: Mild “cobblestoning” No facial tenderness Normal heart and lungs Normal spirometry

23
Chronic Sinusitis

24
Causes of Upper Airway Cough Syndrome

25
Upper Airway Cough Syndrome
Also called “Post-nasal drip syndrome” (PNDS) Common cause of chronic cough in all age groups – Second most common cause in children – Most common cause in adults and the elderly In addition to cough, UACS can also cause - Wheeze - Dyspnea
 Common cause of chronic cough in all age groups. – Second most common cause in children. – Most common cause in adults and the elderly. In addition to cough, UACS can also cause. - Wheeze. - Dyspnea.")
26
Upper Airway Cough Syndrome
Clues to UACS – History of • Need to frequently clear their throat • Friend/relative notices that the patient frequently clears their throat • Sensation of dripping into throat • Nasal symptoms – Physical Exam demonstrating • Secretions in nose or oropharynx • Cobblestone appearance of mucosa

27
Upper Airway Cough Syndrome
Diagnosis of UACS as a cause of cough is established when: frequent throat clearing is elicited from the history b) cobblestoning and phlegm are present on physical examination of the posterior pharynx c) cough responds favourably to specific therapy aimed at eliminating the drip
 cobblestoning and phlegm are present on. physical examination of the posterior pharynx. c) cough responds favourably to specific therapy. aimed at eliminating the drip.")
28
Treatment Antibiotics – sinusitis
Oral antihistamine/decongestant x 3 weeks Intranasal decongestant for maximum of 5 days: e.g. oxymetazoline 2 sprays each nostril bid x 3 days only

29
Treatment Allergic Rhinitis • Allergen avoidance • Intranasal steroid • Antihistamine • Antihistamine/decongestant

30
Case Scenario 2 The Computer Programmer, 35 y.o woman
c/o Yearly cough lasted for > 8 weeks – starts only after a “cold weather” at end of the year – severe coughing – goes away by itself – has happened last year - nocturnal cough • Tried “everything”

31
Case Scenario 2 Denies: wheezes, PND sx, allergies, heartburn, aspiration • No: pets, current meds • Family hx: negative • PMH: negative • Physical exam and CXR normal • Normal spirometry Any other Ix? Methacholine Challenge Testing

32
Asthma Second most common cause of cough in adults
• Clues that chronic cough is due to asthma: – Episodic wheezing, dyspnea , cold or exercise induced – Reversible airflow obstruction – Bronchial hyperresponsiveness • Confirmed by resolution of cough with asthma treatment

33
Cough Variant Asthma • 30-60% of patients presenting with chronic cough that was due to asthma had cough as their ONLY symptom Clues: - nocturnal cough, exercise induced, after allergen exposure Bronchoprovocation test: positive Negative test exclude asthma but does not rule out steroid responsive cough

34
ASTHMA/Cough Variant Asthma
Treatment • Inhaled corticosteroid • ICS/LABA combination > 8 weeks Leukotrine receptor antagonist -Confirmed by resolution of cough with asthma treatment

35
Non-Asthmatic Eosinophilic Bronchitis (NAEB)
Eosinophilic airway inflammation WITHOUT variable airflow obstruction or airway hyperresponsiveness Diagnostic tests: Spirometry: normal Methacholine challenge: normal Sputum or BAL eosinophilia: >3% eosinophils Diagnostic/Therapeutic trial: inhaled corticosteroid for ≥ 4 weeks Characteristically resistant to bronchodilator but reponds ICS Confirmed diagnosis if responded to ICS

36
Case Scenario 2 The Computer Programmer…
• Aggressive asthma regimen x 8 weeks Not feeling better Now what??

37
GERD Suspect GERD when… – Symptoms of heartburn or sour taste in mouth
– Reflux demonstrated by • 24-hour pH-impedance monitoring • Barium x-ray • Cough is the only symptom of GERD in 40-75% of patients with chronic cough due to GERD

38
GERD Cough due to GERD occurs most commonly while patients are awake, stooping posture, meal related, and usually does not occur during the night • Diagnosis of GERD as cause of chronic cough requires resolution of cough with GERD treatment

39
GERD Life-style changes Stop smoking Avoid alcohol Lose weight
Elevate HOB Small meals Avoid fatty/acidic foods /low fat diet Avoid caffeine Avoid – tight clothes, eating < 4 hrs pre-bed, recumbency 3 hrs post meal

40
TReatment Conservative measures : • Antacid therapy ≥ 2 months : – Proton pump inhibitor (high dose) – H2 blockers less effective • Motility therapy: – Metoclopromide Surgery is last resort
 – H2 blockers less effective • Motility therapy: – Metoclopromide Surgery is last resort")
41
ACE-inhibitor therapy
Angiotensin converting enzyme (ACE) inhibitors (enalapril, captopril, lisinopril, ramipril, etc.) Dry cough in 3-30% patients Begins 1 week to 6 months after drug started Usually resolves 1-7 days after stopping therapy, but can take 4 weeks Diagnosis is confirmed when cough disappears after drug in discontinued Minority of patient will have persistent cough even after the medication was off
 inhibitors (enalapril, captopril, lisinopril, ramipril, etc.) Dry cough in 3-30% patients. Begins 1 week to 6 months after drug started. Usually resolves 1-7 days after stopping therapy, but can take 4 weeks. Diagnosis is confirmed when cough disappears after drug in discontinued. Minority of patient will have persistent cough even after the medication was off.")
43
Fibreoptic bronchoscopy – biopsy
High Resolution CT scan: lung parenchymal disease or bronchiectasis (not appreciated from hx and CXR)
")
44
Case scenario 3 Hamid, a 45 year old gentleman who is a clerk presented to the outpatient clinic after coughing up 2 cups of bright red blood. For the past 2 months, he has chronic cough productive of whitish mucoid sputum Prior to this episode, he had, on two occasion a blood-streaking on his sputum. He has also noticed that over the last few weeks he tires easily and is short of breath whenever he exerts himself Hemoptysis pulm origin: frothy sputum, absence of brownish-colored blood due to hemoglobin. a/w cough rather than vomitng. Usually blood is mixed with sputum Non pulm hemoptysis: dt aspiration of blood from nasal, oropharyngeal, gi or other bleeding site are brownish in colour Possible cause of hemoptysis Lung ca Ptb Bronchiectasis LVF Pneumonia Pulmm infarction

45
Case scenario 3 Further history..
Constitutional symptoms (fever, LOA, LOW) Fhx or contact with PTB patient Smoking history Occupation and habits On direct questioning, he admit smoking 2 packs of cigarettes daily for the last 20 years but he has no known medical illness except for history of appendicectomy done 15 years ago. His appetite has been poor and he lost about 4 kg of his weight in 1 month , no contact with PTB paient.
 Fhx or contact with PTB patient. Smoking history. Occupation and habits. On direct questioning, he admit smoking 2 packs of cigarettes daily for the last 20 years but he has no known medical illness except for history of appendicectomy done 15 years ago. His appetite has been poor and he lost about 4 kg of his weight in 1 month , no contact with PTB paient.")
46
Case scenario 3 Physical examination discloses a slightly apprehensive looking man who is not in acute distress. T: PR:100 bpm,regular, BP:130/80 mmHg and RR:17 per minute Slight pallor but no cyanosis, no significant lymphadenopathy or finger clubbing Auscultation of the chest: generalized coarse crepitations but more over the right upper lobe CVS is normal with no signs of cardiac failure There is no calf tenderness At this point the most likely diagnosis is PTB What ix would u request

47
Case scenario 3 Investigations: Full blood count ESR Blood C & S
Mantoux test Sputum AFB & cytology Chest X-ray ECG

48
Smear positive Pulmonary Tuberculosis
Mantoux test is 12mm Sputum: negative for AFB Bronchoscopic washings :positive for acid fast bacilli

49
Standard treatment regime:
Intensive phase Goal is to quickly kill the rapidly dividing organism to control disease and render patient non-infectious and prevent emergence of drug resistance Continuation phase Sterilize the lungs by killing dormant and semi-dormant organisms to prevent relapse DOT allows for intermittent therapy

50
Treatment of TUBERCULOSIS
2 months of daily EHRZ (2EHRZ) 4 months of daily HR (4 HR) Dosage of 1st line anti-TB drugs If ethambutol is contraidicated, streptomycin can be substituted
 4 months of daily HR (4 HR) Dosage of 1st line anti-TB drugs. If ethambutol is contraidicated, streptomycin can be substituted.")
51
TUBERCULOSIS Frequency Optimal Duration
New patient with PTB: daily intensive regimen f/by daily maintenance regimen Thrice weekly maintenance regimen can be considered under direct observation All extrapulmonary: minimum 6 months except- - Bone and joint TB: 6 – 9 months - TB Meningitis: 9 –12 months No retrievable evidence on optimal duration of treatment for disseminated TB and miliaryTB -- should be low threshold to suspect TB meningitis WHO recommends daily dosing thorughout the entire treatment However, a daily intensive phase followed by thrice weekly maintenance phase is an option provided that each dose is directly observed and patient has improved clinically. A maintenance phase with twice weekly dosing is not recommended since missing one dose means the patient receives only half the total dose for that week

52
TUBERCULOSIS Follow-Up During & After Treatment
Patients with initial sputum smear positive should have repeat sputum smear at two and six months of antituberculous (antiTB) treatment. (Grade C) • Patients with initial sputum smear negative should have repeat sputum smear at two months of antiTB treatment. If still negative, no further sputum sample is required. (Grade C) • Patients who remains sputum positive at two months should be referred to specialist with experience in tuberculosis (TB) management. (Grade C) • Sputum Mycobacterium tuberculosis culture and sensitivity testing should be obtained at the start of antiTB treatment. (Grade C) • Chest x-ray should be performed at two and six months of antiTB treatment. (Grade C) • Follow-up within one month of starting antiTB treatment is advisable. (Grade C) • Follow-up may not be conducted routinely after completion of antiTB treatment. Patients should be well-informed on symptoms of TB recurrence. (Grade C) • Patients should be monitored for complications of antiTB drugs. (Grade C)
 treatment. (Grade C) • Patients with initial sputum smear negative should have repeat sputum smear at two. months of antiTB treatment. If still negative, no further sputum sample is required. (Grade C) • Patients who remains sputum positive at two months should be referred to specialist with. experience in tuberculosis (TB) management. (Grade C) • Sputum Mycobacterium tuberculosis culture and sensitivity testing should be obtained at. the start of antiTB treatment. (Grade C) • Chest x-ray should be performed at two and six months of antiTB treatment. (Grade C) • Follow-up within one month of starting antiTB treatment is advisable. (Grade C) • Follow-up may not be conducted routinely after completion of antiTB treatment. Patients. should be well-informed on symptoms of TB recurrence. (Grade C) • Patients should be monitored for complications of antiTB drugs. (Grade C)")
53
Case Scenario 4 Tony is a bus conductor aged 45 years
c/o recent exacerbation of his chronic cough with productive of yellow-green sputum Heavy smoker for 25 years. He has a long standing smoker’s cough frequently productive in recent years. Last year he suffered many exacerbation of his bronchitis, two of which were severe enough for him to be admitted to hospital. Although he had returned to work, progressive dyspnoea had made his job increasingly difficult

54
Case Scenario 4 Examination: drowsy, plethoric and cyanosed, flapping tremor was elicited. RR was 25/min, T: 38.2, PR: 124/min, regular rhythm, BP 120/80mmHg JVP raised 8cm, gallop rhythm was heard, sacral oedema present. Both lung fields had scattered crepitations and diminished air entry. The liver was felt 3 cm below the costal margin. No focal neurological deficit.

55
CHRONIC OBSTRUCTIVE AIRWAY DISEASE
SYMPTOMS Shortness of breath Chronic cough Sputum EXPOSURE TO RISK FACTORS Tobacco Occupation Indoor/outdoor pollution Spirometry should be performed after the administration of an adequate dose of a short-acting inhaled bronchodilator to minimize variability. A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation. SPIROMETRY: Required to establish diagnosis

56
CHRONIC OBSTRUCTIVE AIRWAY DISEASE
An exacerbation of COPD is: “an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication.”

57
The goal of treatment is to minimize the impact of the current exacerbation and to prevent the development of subsequent exacerbations Arterial blood gas measurements (in hospital): PaO2 < 8.0 kPa with or without PaCO2 > 6.7 kPa in room air indicates respiratory failure. Chest X-Ray: useful to exclude alternative diagnoses. ECG: may aid in the diagnosis of coexisting cardiac problems. Full blood count: identify polycythemia, anemia, infection Purulent sputum during an exacerbation: indication to begin empirical antibiotic treatment. Biochemical tests: detect electrolyte disturbances, diabetes, and poor nutrition. Spirometric tests: not recommended during an exacerbation. Antibiotics should be given to patients with: Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence. Who require mechanical ventilation
: PaO2 < 8.0 kPa with or without PaCO2 > 6.7 kPa in room air indicates respiratory failure. Chest X-Ray: useful to exclude alternative diagnoses. ECG: may aid in the diagnosis of coexisting cardiac problems. Full blood count: identify polycythemia, anemia, infection. Purulent sputum during an exacerbation: indication to begin empirical antibiotic treatment. Biochemical tests: detect electrolyte disturbances, diabetes, and poor nutrition. Spirometric tests: not recommended during an exacerbation. Antibiotics should be given to patients with: Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence. Who require mechanical ventilation.")
58
Oxygen: titrate to improve the patient’s hypoxemia with a target saturation of 88-92%.
Bronchodilators: Short-acting inhaled beta2-agonists with or without short-acting anticholinergics are preferred. Systemic Corticosteroids: - Shorten recovery time, improve lung function (FEV1) and arterial hypoxemia (PaO2) - reduce the risk of early relapse, treatment failure, and length of hospital stay. mg prednisolone per day for days is recommended Noninvasive ventilation (NIV): -Improves respiratory acidosis, decreases respiratory rate, severity of dyspnea, complications and length of hospital stay
 and arterial hypoxemia (PaO2) - reduce the risk of early relapse, treatment failure, and length of hospital stay mg prednisolone per day for days is recommended. Noninvasive ventilation (NIV): -Improves respiratory acidosis, decreases respiratory rate, severity of dyspnea, complications and length of hospital stay.")
59
CHRONIC OBSTRUCTIVE AIRWAY DISEASE
Indications for Hospital Admission Marked increase in intensity of symptoms Severe underlying COPD Failure of an exacerbation to respond to initial medical management Presence of serious comorbidities Frequent exacerbations Older age Insufficient home support

60
Management of Stable COPD
KEY POINTS Identification and reduction of exposure to risk factors are important steps in prevention and treatment Individualized assessment of symptoms, airflow limitation, and future risk of exacerbations should be incorporated into the management strategy All COPD patients benefit from rehabilitation and maintenance of physical activity. Pharmacologic therapy is used to reduce symptoms, reduce frequency and severity of exacerbations, and improve health status and exercise tolerance. Long-acting formulations of beta2-agonists and anticholinergics are preferred over short-acting formulations Long-term treatment with inhaled corticosteroids added to long-acting bronchodilators is recommended for patients with high risk of exacerbations Long-term monotherapy with oral or inhaled corticosteroids is not recommended in COPD The phospodiesterase-4 inhibitor roflumilast may be useful to reduce exacerbations for patients with FEV1 < 50% of predicted, chronic bronchitis, and frequent exacerbations Avoidance of risk factors - smoking cessation - reduction of indoor pollution - reduction of occupational exposure Influenza vaccination Based on efficacy and side effects, inhaled bronchodilators are preferred over oral bronchodilators.

61
Global Strategy for Diagnosis, Management and Prevention of COPD
Assessment of COPD Assess symptoms : CAT, mMRC Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day-to-day. Dyspnea: Progressive, persistent and characteristically worse with exercise. Chronic cough: May be intermittent and may be unproductive. Chronic sputum production: COPD patients commonly cough up sputum

62
(C) (D) (B) (A) Risk Risk Symptoms 4 > 2 3 2 1 1 mMRC 0-1
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD 4 (C) (D) > 2 3 (Exacerbation history) Risk (GOLD Classification of Airflow Limitation) Risk 2 (A) (B) 1 1 mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)) © 2013 Global Initiative for Chronic Obstructive Lung Disease
 (D) > (Exacerbation history) Risk. (GOLD Classification of Airflow Limitation) Risk. 2. (A) (B) mMRC 0-1. CAT < 10. mMRC > 2. CAT > 10. Symptoms. (mMRC or CAT score)) © 2013 Global Initiative for Chronic Obstructive Lung Disease.")
63
Use combined assessment
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Use combined assessment Patient is now in one of four categories: A: Less symptoms, low risk B: More symptoms, low risk C: Less symptoms, high risk D: More symptoms, high risk 4 (C) (D) > 2 3 (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) Risk 2 1 (A) (B) 1 mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)) © 2013 Global Initiative for Chronic Obstructive Lung Disease
 (D) > (GOLD Classification of Airflow Limitation) Risk. (Exacerbation history) Risk (A) (B) 1. mMRC 0-1. CAT < 10. mMRC > 2. CAT > 10. Symptoms. (mMRC or CAT score)) © 2013 Global Initiative for Chronic Obstructive Lung Disease.")
64
Pharmacologic Therapy RECOMMENDED FIRST CHOICE
GOLD 4 ICS + LABA or LAMA ICS + LABA and/or LAMA > 2 GOLD 3 Exacerbations per year A B GOLD 2 SAMA prn or SABA prn LABA or LAMA 1 SAMA: short acting muscarinic agent = also called short acting anticholinergic e.g ipratropium bromide, o xitropium bromide LAMA: thiotopium, aclinidium bromide SABA: short acting B2 agonist : salbutamol, fenoterol, terbutaline LABA: Formoterol,Salmeterol ICS: beclomethasone, budesonide, fluticasone Symbicort: fluticasone + salmeterol Combivent: albuterol + ipratropium Pulmicort: budesonide Spiriva: tiotropium Proventil: albuterol Atrovent: ipratropium GOLD 1 mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10

65
Rehabilitation Exercise training programs : improves exercise tolerance and symptoms of dyspnea and fatigue Pulmonary rehabilitation program: the longer the program continues, the more effective the results Oxygen Therapy: The long-term administration of oxygen (> 15 hours per day) to patients with chronic respiratory failure has been shown to increase survival in patients with severe, resting hypoxemia Ventilatory Support: Combination of noninvasive ventilation (NIV) with long-term oxygen therapy may be of some use in a selected subset of patients Lung volume reduction surgery (LVRS) : more efficacious than medical therapy among patients with upper-lobe predominant emphysema and low exercise capacity Lung Transplantation : In appropriately selected patients with very severe COPD, improve quality of life and functional capacity
 to patients with chronic respiratory failure has been shown to increase survival in patients with severe, resting hypoxemia. Ventilatory Support: Combination of noninvasive ventilation (NIV) with long-term oxygen therapy may be of some use in a selected subset of patients. Lung volume reduction surgery (LVRS) : more efficacious than medical therapy among patients with upper-lobe predominant emphysema and low exercise capacity. Lung Transplantation : In appropriately selected patients with very severe COPD, improve quality of life and functional capacity.")
66
Take Home Message In patients with chronic cough and a normal CXR finding who are nonsmokers and are not receiving therapy with an ACE inhibitor, the diagnostic approach should focus on the detection and treatment of UACS (formerly called PNDS), asthma, NAEB, or GERD, alone or in combination. This approach is most likely to result in a high rate of success in achieving cough resolution. ACCP Evidence-Based Clinical Practice Guidelines
, asthma, NAEB, or GERD, alone or in combination. This approach is most likely to result in a high rate of success in achieving cough resolution. ACCP Evidence-Based Clinical Practice Guidelines.")
67
THANK YOU

Similar presentations


>")
 Airway.>")

 BONUS.>")
 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")



 By Chris Callan 23 April 2008.>")

>")





 Professor Bill MacNee>")
 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")
