Download presentation
Presentation is loading. Please wait.

1
Transplant Immunology – A User’s Guide!! Dr Mary Keogan Consultant Clinical Immunologist & Medical Director, NHISSOT Beaumont Hospital

2
Overview l A little bit about the immune system l What happens in the lab when you are listed. l What happens on the night when there is a donor. l What happens when you have a living donor l What can be done for people who are highly sensitised.

3
The immune system fights infection Distinguishes self from non-self Attacks non-self

4
A transplanted organ is “non-self” Distinguishes self from non-self Attacks non-self

5
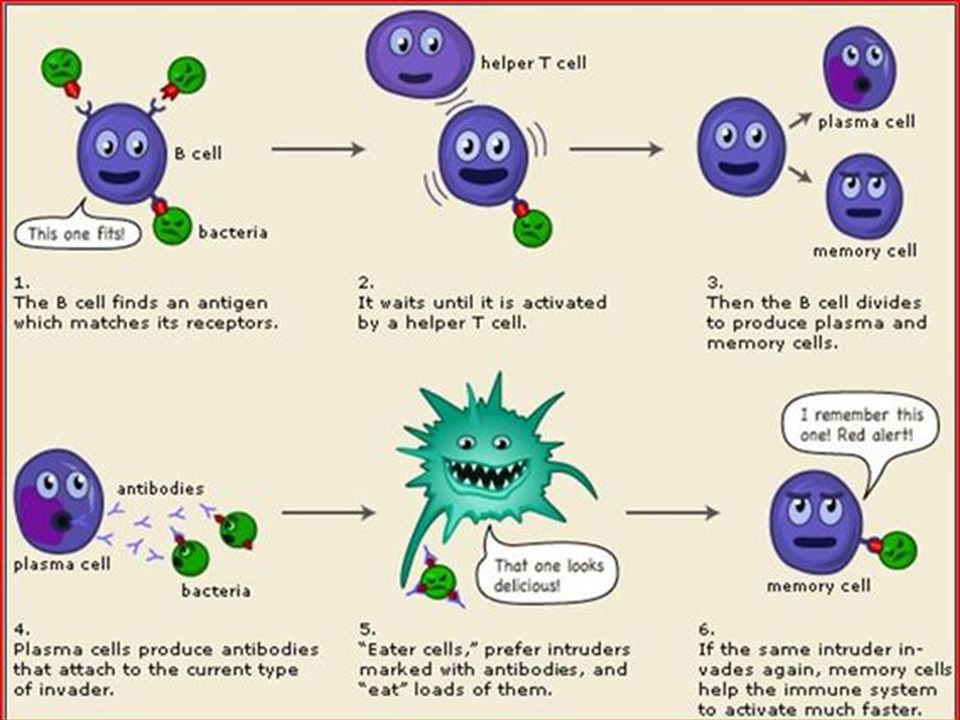
Our Immune army – 2 main platoons l B cell platoon Make antibodies Damage organ Easy to measure l T cell platoon Cause most rejection Better controlled than B cells by immunosuppression Hard to measure

6
What are antibodies? l Proteins made by cells of the immune system (B cell platoon) l Job is to fight infection l Can damage graft l Some types more damaging that others
 l Job is to fight infection l Can damage graft l Some types more damaging that others.")
7
The immune system remembers l Memory T & B cells react quickly & strongly l Meds control new immune cells better Difficult to control memory cells If have antibodies likely to have memory cells Memory cell

8
That’s not a dog Remember how good cat tastes? Organ Immune System

9
Rejection l Avoid Hyperacute l Minimise AMR l Reduce Cellular Rejection

10
How does the immune system know my transplant is “non- self”? l Blood Group l Tissue Type (HLA type) l 1000s of other differences
 l 1000s of other differences.")
11
Immunologically ideal transplant l MUST be Blood Group Compatible l SHOULD be anti-HLA antibody compatible l IDEALLY, well HLA-matched Even if “perfect HLA match” transplant is non-self

12
When you are listed l History - transplants; pregnancy; transfusions. l Check blood group (twice) l Check HLA type (1 full; 1 check) l Measure antibodies to HLA molecules l Recheck every 3 months l If sample not received, temporarily suspended from list
 l Check HLA type (1 full; 1 check) l Measure antibodies to HLA molecules l Recheck every 3 months l If sample not received, temporarily suspended from list.")
13
How does my blood group affect my kidney? l Markers are on all your cells, not just blood cells l Blood group made up of markers Group A – A marker Group B – B marker Group O – no A or B marker Group AB – A & B markers l Your immune system reacts to markers you don’t have – they are “non-self”

15
Your TissueType (HLA type) More flags for your immune system Use to say how well matched a donor is.
 More flags for your immune system Use to say how well matched a donor is.")
16
Antibodies to HLA l Your own tissue (HLA) type is self l Other tissue types are non-self l If exposed to other HLA types, you may make antibodies & memory cells l Exposure – transplant; transfusion; pregnancy l Sometimes infections cause anti-HLA antibodies l Check what tissue types you have made antibodies to. l Aim to identify donor to whom you have NO antibody

17
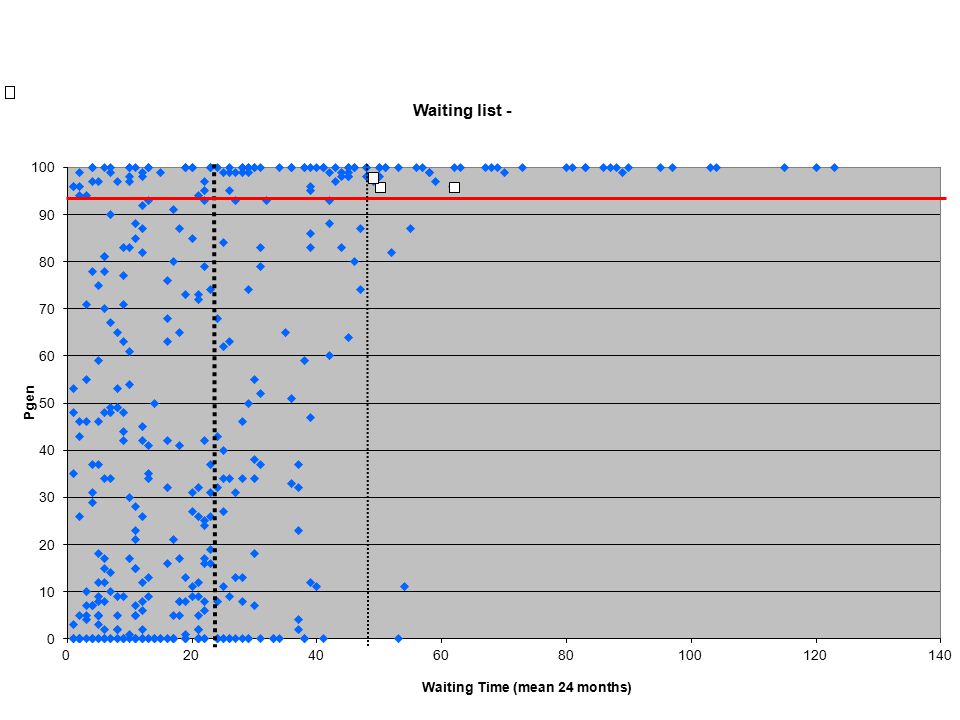
Whats my Pgen? l We measure antibodies when listing, after transfusions and pregnancy. l Recheck every 3 months l Make a list of all your antibodies l Match against database of thousands of donors l Pgen is the percentage of Irish donors against whom you have antibodies. l Measure of how hard it is to find an antibody compatible donor for you

18
What does my Pgen mean? l Lower – antibodies against fewer donors l Higher – more difficult to find ideal donor l We use allocation to “level the playing field” l Extra priority if Pgen >50% l High priority if >94% l Consider higher risk transplant if >94%

19
What happens when there is a deceased donor? l Blood sent to lab – Blood group & HLA type checked l Run matching programme to identify patients who do not have antibodies to the donor l Prepare shortlist of potential recipients who are blood group & anti-HLA antibody compatible.

20
Recipient short list l Clinically urgent l Paediatric patients l Pgen >94% l Pgen > 50% l Best HLA matched l Recipients with rare types l Longest waiting

22
Crossmatch Potential Recipients & back-ups l Test up to 4 potential recipients to prevent delays l Once crossmatch cleared, recipients are contacted. l If unwell, back-up patient called l If crossmatch positive due to anti-HLA transplant is increased risk, or may be too high risk to proceed.

23
Crossmatch measures antibody binding to donor cells Thousands of Different cell surface proteins Positive result if antibodies to any of them Only relevant if anti-HLA antibodies

24
Living Donors – Immunological assessment l Blood Group checked locally l Determine tissue (HLA) type l See if recipient has antibodies against the donor. l Determine immunological risk

25
Your Tissue Type (Aka HLA type) More flags for your immune system Use to say how well matched a donor is.
 More flags for your immune system Use to say how well matched a donor is.")
26
You inherit “packages” of HLA flags from each parent

27
Risk assessment l Low Risk – Perfect HLA match l Standard Risk – No antibodies against donor now or in the past l Slight increase in risk – weak antibodies, negative crossmatch. l Increased risk – antibodies against donor; can mitigate with immunosuppression. Detailed discussion re alternatives l High risk – unsuitable, at least without antibody removal

28
LD Assessment l If Immunology unlikely to preclude transplantation, assessment proceeds. l Monitor 3 monthly samples for new antibodies against the donor l Within 3 months of expected date formal review – may include crossmatch. l Crossmatch the week before transplant

29
My Pgen is 100%. What about me? l Means antibodies to >99.5% of population l Additional priority as Pgen >94% l Living Donor l If LD incompatible – Paired kidney exchange l 100% reviews – define antibodies that are less damaging. Then transplant with augmented immunosuppression.

30
Graft Survival 3 months1 year3years5years10 years DSA+ C1q+ n=15 787164 55 DSA+ C1q- n=46 9185827667 No sig. Abs. n=145 9897948680 % graft survival

31
2012/2013 – 33 of the most complex patients transplanted l Deceased donors l 9 x 100% patients l 12 x AMM patients l Living donors l 9 -100% patients l 1 – 100%ABOi l 2 - AMM patients l 8 because of 100% review programme

32
The future……….. l Transplant plans for patients with Pgens of 100% l Each member of staff “adopts” a 100% patient. Detailed review of every antibody. l Review opens windows to facilitate transplant in many patients l Consider increased risk transplants in long waiting patients with few opportunities l ?desensitisation

33
That’s not a dog Remember how good cat tastes? Organ Immune System Don’t let your puppy immune cells turn into memory cells

Similar presentations







 Anti-A11 and B44.>")





 Anindyaningrum Chrisant Rystiasih Nadia Karlina *Protein images comparing the MHC I (1hsa) and MHC II (1dlh) molecules.>")







