Download presentation
Presentation is loading. Please wait.

1
Hematopoietic Stem Cell Transplantation Lynn Savoie September 30, 2006

2
Hematopoietic stem cell transplantation is potentially life-saving therapy in patients with SAA or MDS Generally done when benefits thought to outweigh risks Only allogeneic stem cell transplantation considered for these diseases therefore need a donor Recipient and donor factors considered when assessing risk

3
General Concept Blood cell production and immune system very closely linked and ultimately derived from bone marrow Goal of high dose chemotherapy is to kill “defective” marrow – MDS or malfunctioning immune system – SAA Replace with healthy marrow/immune system – Unfortunately not straightforward – mostly due to the new immune system

4
Risks Infections –Potentially life or organ threatening Due to neutropenia then immunosupression Graft versus host disease –New immune system attacking recipient organs –Acute and chronic Can affect many different organs –Potentially life or organ threatening –Potentially life altering Graft failure –Rare but potentially fatal Increased risk in aplastic anemia

5
Types of transplants 3 main factors

6
Type of donor –Related –Unrelated Source of stem cell –Bone marrow –Peripheral blood –Cord blood Conditioning Regimens –Myeloablative –Non-myeloablative –TBI containing

7
Type of donor Related vs. Unrelated

8
HLA Matching

9
HLA antigens –Proteins that help the immune system identify self vs. non-self –Genetically inherited together on chromosome 6 –Most important determinant of compatibility between donor and recipient –Each sibling pair has a 25% chance of inheriting the same HLA antigens –Approximately 30% of patients will have an HLA matched sibling

10
MOTHERFATHER M1M2 F1F2 CHILDCHILD M1F1 M2F1 CHILDCHILD M2F2 M1F2

11
Statistically unlikely for an extended family member to have 2 similar HLA groupings to patient just by chance Able to find a unrelated donor in 70% of cases that is fully matched but not likely “identical” Search can take time More difficult in some ethnic groups due to genetic diversity Generally increased and more severe graft versus host disease than with related donor

12
Other important factors in donor selection Age –Younger generally better Sex –Males generally better Number of pregnancies –Few the better Blood group –Same is better CMV status –Negative donor is best if patient is negative Health –Some health conditions preclude donation from a recipient perspective and some from a donor perspective

13
Source of Stem Cell Bone marrow vs. peripheral blood vs. cord blood

14
Still unclear whether bone marrow or peripheral blood stem cells better for recipients – studies ongoing –Currently using bone marrow in SAA and peripheral blood in MDS Faster count recovery with peripheral blood stem cells but increase chronic graft versus host disease that may or may not translate into decreased relapse Peripheral blood collection generally felt to be easier for donor but long term effects of G-CSF not known

15
Cord Blood Stem Cells Rapidly available Can accept a lesser match Less graft versus host disease –Immune cells naive Cell doses often a concern in adults –Because based on weight Longer time to count recovery –can increase risk of infection due to prolonged neutropenia Combinations or expansion being investigated

16
Conditioning Regimens Myeloablative vs. Non- myeloablative vs. TBI containing

17
Myeloablative –Generally used for SAA or MDS –Calgary regimens somewhat less myeloablative than other regimens…..but not technically non- myeloablative Non-myeloablative –Unclear if really safer – generally more graft vs. host disease, particularly chronic due to mixture of cells present –Unclear if really a role in these disorders since don’t need much graft vs. leukemia effect-under investigation TBI containing –Used in acute leukemia and at times in MDS if transforming – felt to decrease relapse

18
IBMTR, MDS, Sib HSCT

20
EBMT, SAA

21
IBMTR, SAA, Sib HSCT

22
Calgary – FLUBUP +/- TBI From 05/99 to 05/05 Matched related donor (MRD) –201 pts, survival 60% Mismatched related donor (MMRD) –22 pts, survival 58% Matched unrelated donor (MUD) –81 pts, survival 57% Mismatched unrelated donor (MMUD) –40 pts, survival 38%
 –201 pts, survival 60% Mismatched related donor (MMRD) –22 pts, survival 58% Matched unrelated donor (MUD) –81 pts, survival 57% Mismatched unrelated donor (MMUD) –40 pts, survival 38%")
23
Calgary MDS –MRD – 15 pts Survival 79% –Alt – 10 pts Survival 38% SAA –MRD -20 pts survival 90%, 100% in last 13 yrs –Alt – 10 pts survival 38%

24
Indications

25
Myelodysplasia –Patients < 65 yrs of age –Before transfusion dependence and/or clinically significant neutropenia –Before transformation to acute leukemia Severe aplastic anemia –If pt < 40 y.o. with sib match –If >60 y.o. pt > 40 y.o. with sib match trial after failure of immunosupression –No sib match – Failure of immunosupression X 2, consider after 1 if pt is young

26
Donor Search Type sibling at presentation if HSCT at all a consideration now or later Can identify an unrelated donor when HSCT strongly under consideration –Costs –Can only “hold” a donor for 3 months

27
UBMDR Established in 1989 Administered by Canadian Blood Services 215 000 potential volunteer donors If no Canadian donor can search the world

28
NMDP United States 6 million donors 50 000 cord blood units

29
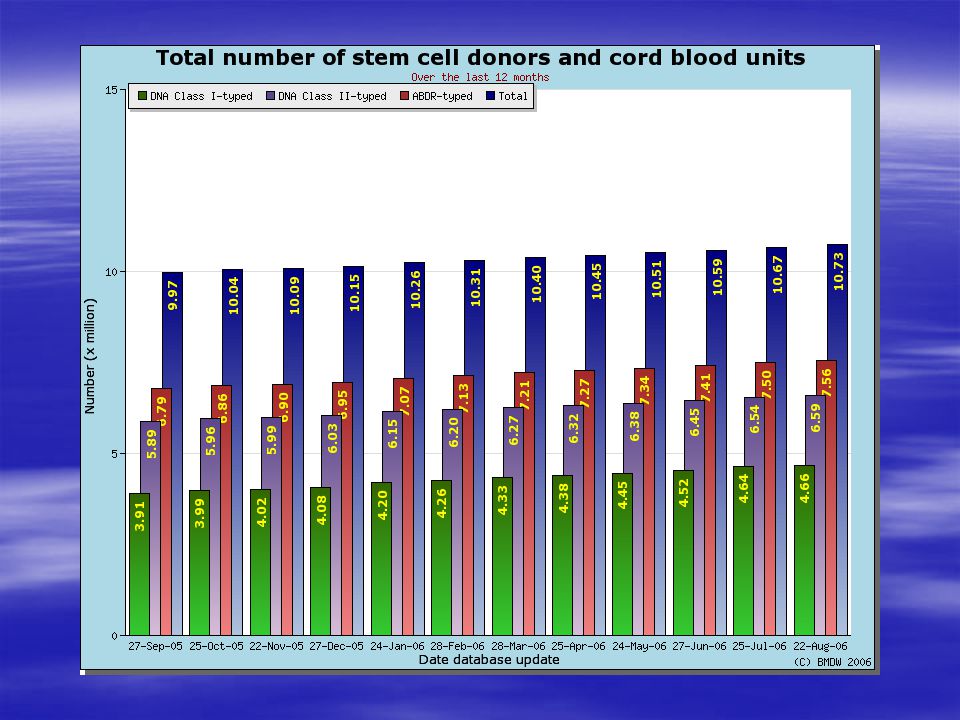
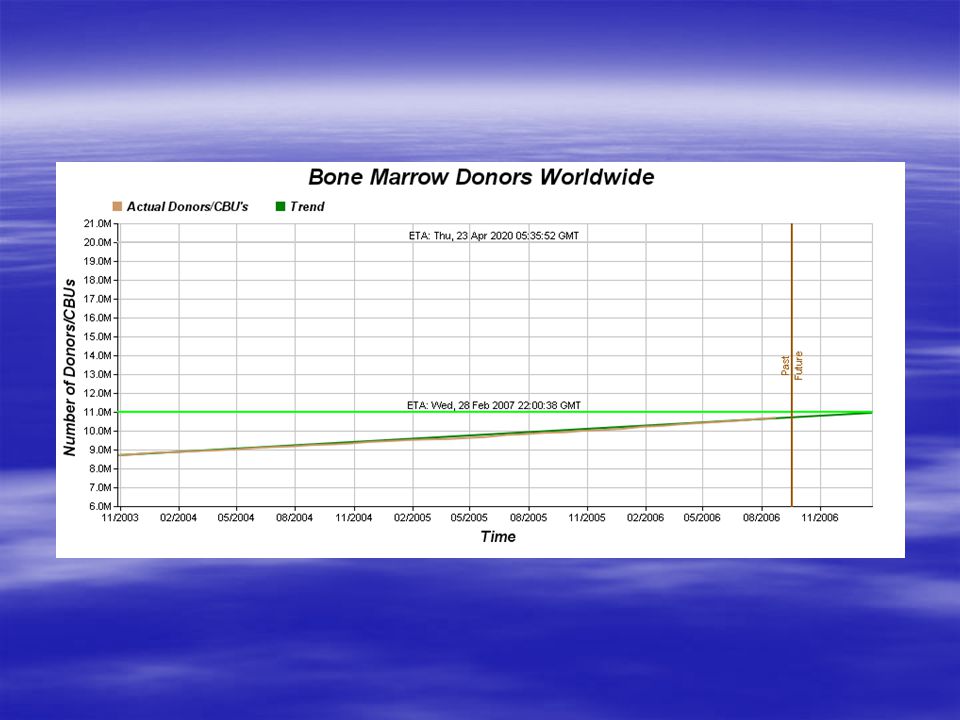
Bone Marrow Donors Worldwide As of August 22, 2006 – 10 733 542 donors and cord blood units 58 stem cell donor registries from 43 countries 38 cord blood banks from 21 countries 571 users from 420 organizations

Similar presentations














 Overview Willis H Navarro, MD Medical Director, Transplant Services, NMDP Associate Clinical Professor,>")
 the immunology goes two ways. There is host vs. graft.>")







