Download presentation
Presentation is loading. Please wait.

1
Pediatric Radiography

2
Children do not all reach a sense of understanding at the same predictable age. This ability varies from child to child, and the pediatric technologist must not assume that children will comprehend what is occurring. Generally, however, by the age of 2 or 3 years, most children can be talked through a diagnostic radiographic study without immobilization or parental aid. Most important is a sense of trust, which begins at the first meeting between the patient and the technologist; the first impression that the child has of the technologist is everlasting and forges the bond of a successful relationship.

3
Successful radiographic studies are dependent on two things:
The technologist's attitude and approach to a child. The technical preparation in the room.

4
At the first meeting, most children are accompanied by at least one parent or caregiver. The following steps are important: Introduce yourself as the technologist who will be working with this child. Find out what information the attending physician has given to the parent and patient. Explain what you are going to do and what your needs will be.

5
Tears, fear, and combative resistance are common reactions for a young child. The technologist must take the time to communicate to the parent and the child, in language they can understand, exactly what he or she is going to do. The technologist must try to build an atmosphere of trust in the waiting room before the patient is taken into the radiographic room. This includes discussing the necessity of immobilization as a last resort if the child's cooperation is unattainable.

7
Evaluate Parent's (or Caregiver's) Role
Parent is in room as an observer, lending support and comfort by his or her presence. Parent serves as a participator, assisting with immobilization. Parent is asked to remain in the waiting area and not accompany the child into the radiography room. . Sometimes children who act fearful and combative in the waiting room with the parent present will be more cooperative without their presence. This is the time when the technologist's communication skills are tested

8
REPORTING SUSPECTED CHILD ABUSE
Most medical facilities have a procedure in place to report suspected child abuse. In the past, the term used for this was battered child syndrome (BCS). The current acceptable term is nonaccidental trauma (NAT). Generally, it is not the responsibility of the technologist to make a judgment as to whether child abuse has occurred, but rather to report the facts as they are seen or suspected. If NAT is suspected, the technologist should discuss this with the radiologist or other supervisor as determined by departmental protocol. Laws vary on technologists' responsibilities, and it is most important that all technologists know what their responsibilities are concerning this in the state or province in which they are working.
. The current acceptable term is nonaccidental trauma (NAT). Generally, it is not the responsibility of the technologist to make a judgment as to whether child abuse has occurred, but rather to report the facts as they are seen or suspected. If NAT is suspected, the technologist should discuss this with the radiologist or other supervisor as determined by departmental protocol. Laws vary on technologists responsibilities, and it is most important that all technologists know what their responsibilities are concerning this in the state or province in which they are working.")
9
Pediatric patients in general can include infants through children up to ages 12 to 14. However, older children can be treated more like adults, except for special care in gonadal shielding and reduced exposure factors because of their smaller size. In general, pediatric radiography should always use as short exposure times and as high mA as possible to minimize image blurring that may result from patient motion. However, even with short exposure times, preventing motion during exposures is a constant challenge in pediatric radiography, and effective methods of immobilization are essential.

10
Immobilization devices:
Tam-em board Pigg-O-Stat

11
Tam-em board

12
Pigg-O-Stat Pigg-O-Stat (set for PA chest). A.Bicycle-type seat
B.Side body clamps C.Film holder mount D.Swivel base E.Adjustable lead shield with markers F.Mounting stand on wheels G.Extra set of smaller body clamps

13
The simplest and least expensive form of immobilization involves the use of equipment and supplies that are commonly found in most departments. Tape, sheets or towels, sandbags, covered radiolucent sponge blocks, compression bands, stockinettes, and ace bandages, if used correctly, are effective in immobilization.

14
Sandbags Strong canvas-type material and children's coarse sterilized playing sand should be used. Coarse sand is recommended because if the bag should break open, the sand is more easily cleaned up, and the chance of causing artifacts on radiographs is minimized

15
Tape and bandage Various types of “gentle” tape are used for surgical procedures and sensitive skin. Adhesive tape may show on the radiograph and create an artifact that could obscure the anatomic part of interest. Also, some patients have an allergic reaction to adhesive tape. The fragile skin of infants can be injured by adhesive tape, unless the tape is twisted so that the adhesive surface is not against the skin. Gauze pads placed between skin and adhesive tape also can be used effectively A 4-inch ace bandage is best for small infants and young children, whereas a 6-inch bandage works well for older children. These are best used for immobilizing the legs. When starting the wrapping process, begin at the patient's hips and wrap down to the patient's midcalf. Do not wrap too tightly; this would cut off circulation.

17
COMPRESSION BANDS AND HEAD CLAMPS
Compression or retention bands are valuable aids for immobilization. Compression bands, however, are more effective with pediatric patients when used in combination with sandbags,

18
WEIGHTED ANGLE BLOCKS AS HEAD CLAMPS
These are heavy steel angle blocks with thick, radiolucent sponge pads attached. They are relatively inexpensive to have made compared with the cost of commercially available head clamps. They are very effective and versatile in immobilization, especially when used in combination with sandbags and/or tape, or if the patient is mummified,

19
MUMMIFYING,” OR WRAPPING WITH SHEETS OR TOWELS

21
BONE DEVELOPMENT (OSSIFICATION)
The bones of infants and small children go through various growth changes from birth through adolescence. The pelvis is an example of ossification changes that are apparent in children. As shown in, the divisions of the hip bone between the ilium, the ischium, and the pubis are evident. They appear as individual bones separated by a joint space, which is the cartilaginous growth region in the area of the acetabulum. The heads of the femora also appear to be separated by a joint space that should not be confused with fracture sites or other abnormalities. These are normal cartilaginous growth regions.

23
MINIMAL REPEATS Reduction of repeat exposures is critical, especially in young children, whose developing cells are particularly sensitive to the effects of radiation. Proper immobilization and high mA, short exposure time techniques will reduce the incidence of motion unsharpness. Accurate manual technique charts with patient body weights should be used. Radiographic grids should be used only when the body part examined is greater than 10 centimeters in thickness. Each radiology department should keep a list of specific routines for pediatric imaging exams, including specialized views and limited examination series, to ensure that appropriate projections are obtained and no unnecessary exposures are made.

24
GONADAL PROTECTION Gonads of the child should always be shielded with contact-type shields, unless such shields obscure the essential anatomy of the lower abdomen or pelvic area.

26
Pre-exam Preparation The following should be completed before the patient is brought into the room: •The necessary immobilization and shielding paraphernalia should be in place (sandbags, tape, Tam-em board if used, sheets or towels, stockinette, ace bandages, and shielding devices for patient and for parents if assisting). •Image receptors and markers should be in place and techniques set (if a solo technologist is performing the exam). •Specific projections should have been determined, which may require consultation with the radiologist. •If two technologists are working together, they should clarify the role that each will play during the procedure. A suggested division of responsibilities is to have the assisting technologist set techniques, make exposures, change the IRs, and process the images while the primary technologist positions the patient, instructs the parents (if assisting), and positions the tube, collimation, and required shielding.
. •Image receptors and markers should be in place and techniques set (if a solo technologist is performing the exam). •Specific projections should have been determined, which may require consultation with the radiologist. •If two technologists are working together, they should clarify the role that each will play during the procedure. A suggested division of responsibilities is to have the assisting technologist set techniques, make exposures, change the IRs, and process the images while the primary technologist positions the patient, instructs the parents (if assisting), and positions the tube, collimation, and required shielding.")
27
CHILD PREPARATION After the child is brought into the room and the procedure is explained to the child's and parent's satisfaction, the parent or technologist must remove any clothing, bandages, and/or diapers from the body parts to be radiographed. This is necessary to prevent these items from casting shadows and creating artifacts on the radiographic image because of low exposure factors used for the patient's small size.

28
Chest AP Technical Factors
• IR size—determined by the size of the patient • IR crosswise (if supine, place cassette under patient) • Grid not required • Small focal spot • 70 to 80 kV, shortest exposure time possible Shielding Contact lead shielding should be placed over the pelvic area with upper margin to level of iliac crests.
 • Grid not required. • Small focal spot. • 70 to 80 kV, shortest exposure time possible. Shielding. Contact lead shielding should be placed over the pelvic area with upper margin to level of iliac crests.")
29
Patient Position—With Patient Supine
• Patient is supine, arms extended to remove scapula from the lung fields. • Arms are secured to the table with sandbags or Velcro straps if Tam-em board is used. • Legs are extended to prevent rotation of pelvis. Hips and legs are secured by placing sandbags at the level of the hip to the top of the knee. If a Tam-em board is used, hip and legs are Velcro strapped to the board. • With parental assistance (if parent is not pregnant), do the following: 1.Have parent remove child's chest clothing. 2.Provide parent with lead apron and gloves. 3.Place child on the IR. 4.Parent should extend child's arms over head with one hand while keeping head tilted back to prevent superimposing upper lungs. With other hand, hold child's legs at level of the knees, applying pressure as necessary to prevent movement. 5.Place parent in a position that will not obstruct technologist's view of patient while exposure is made. 6.Place lead gloves over the top of the parent's hands if parent is not wearing the gloves. (It may be easier to hold on to the patient if not wearing the gloves.)
, do the following: 1.Have parent remove child s chest clothing. 2.Provide parent with lead apron and gloves. 3.Place child on the IR. 4.Parent should extend child s arms over head with one hand while keeping head tilted back to prevent superimposing upper lungs. With other hand, hold child s legs at level of the knees, applying pressure as necessary to prevent movement. 5.Place parent in a position that will not obstruct technologist s view of patient while exposure is made. 6.Place lead gloves over the top of the parent s hands if parent is not wearing the gloves. (It may be easier to hold on to the patient if not wearing the gloves.)")
30
Part Position • Place the patient in the middle of the IR with the shoulders 2 inches (5 cm) below the top of the IR. • Ensure that the thorax is not rotated. Central Ray • CR perpendicular to the IR, centered to the midsagittal plane at the level of midthorax, which is approximately at the mammillary (nipple) line • SID of 50 to 60 inches (127 to 212 cm); tube raised as high as possible Collimation Closely collimate on four sides to outer chest margins. Respiration Make exposure upon second full inspiration. If child is crying, watch respiration and make exposure immediately after the child fully inhales. .
 line. • SID of 50 to 60 inches (127 to 212 cm); tube raised as high as possible. Collimation. Closely collimate on four sides to outer chest margins. Respiration. Make exposure upon second full inspiration. If child is crying, watch respiration and make exposure immediately after the child fully inhales. .")
33
Patient Position—With Patient Erect
• Patient is placed on seat with legs down through center opening. Adjust seat to correct height so top of IR is about 1 inch (2.5 cm) above shoulders. • Arms are raised and side body clamps are placed firmly against patient and are secured by base adjustment and adjustable strap. • Lead shield is raised to a level about 1 inch above iliac crest. • Correct R and L markers and “insp” (inspiration) marker are set to be exposed on lower image. • Ensure no rotation Central Ray • CR perpendicular to IR at level of midlung fields (at mammary line) • SID of 72 inches (180 cm) Collimation Collimate closely on four sides to outer chest margins. Respiration If child is crying, watch respiration and make exposure as child fully inhales and holds breath. (Children can frequently hold their breath on inspiration after a practice session.)
 above shoulders. • Arms are raised and side body clamps are placed firmly against patient and are secured by base adjustment and adjustable strap. • Lead shield is raised to a level about 1 inch above iliac crest. • Correct R and L markers and insp (inspiration) marker are set to be exposed on lower image. • Ensure no rotation. Central Ray. • CR perpendicular to IR at level of midlung fields (at mammary line) • SID of 72 inches (180 cm) Collimation. Collimate closely on four sides to outer chest margins. Respiration. If child is crying, watch respiration and make exposure as child fully inhales and holds breath. (Children can frequently hold their breath on inspiration after a practice session.)")
36
Radiographic Criteria
Structures Shown: • Entire lungs should be included from apices (C7-T12 level) to costophrenic angles. • The air-filled trachea from T1 down is demonstrated, as well as the hilum region markings, heart, and bony thorax. Position: Chin is sufficiently elevated to prevent superimposition of apices. • No rotation, as evidenced by equal distance from lateral rib margins on each side to the spine and distance from both SC joints to the spine. • Full inspiration—visualizes 9 (occasionally 10) posterior ribs above diaphragm on most patients. Collimation and CR: • Collimation margins on all four sides with equal margins on top and bottom, indicating a correct CR location to midlung fields (T6 or T7). Exposure Criteria: • Sufficient lung contrast to visualize fine lung markings within lungs. • Faint outlines of ribs and vertebrae visible through heart and mediastinal structures. • No motion, as evidenced by sharp outlines of rib margins, diaphragm, and heart shadows
 to costophrenic angles. • The air-filled trachea from T1 down is demonstrated, as well as the hilum region markings, heart, and bony thorax. Position: Chin is sufficiently elevated to prevent superimposition of apices. • No rotation, as evidenced by equal distance from lateral rib margins on each side to the spine and distance from both SC joints to the spine. • Full inspiration—visualizes 9 (occasionally 10) posterior ribs above diaphragm on most patients. Collimation and CR: • Collimation margins on all four sides with equal margins on top and bottom, indicating a correct CR location to midlung fields (T6 or T7). Exposure Criteria: • Sufficient lung contrast to visualize fine lung markings within lungs. • Faint outlines of ribs and vertebrae visible through heart and mediastinal structures. • No motion, as evidenced by sharp outlines of rib margins, diaphragm, and heart shadows.")
37
Lateral Chest Technical Factors
• IR size—determined by the size of the patient • IR lengthwise under patient (unless horizontal beam is taken on Tam-em board) • Grid not required • Small focal spot • 75 to 80 kV, shortest exposure time possible
 • Grid not required. • Small focal spot. • 75 to 80 kV, shortest exposure time possible.")
38
Shielding Contact lead shielding should be placed directly over pelvic area with upper margin at the top of the iliac crest. Patient Position—With Patient Recumbent • Patient is lying on side in true lateral (generally left lateral) position with arms extended above head to remove arms from lung field. Bend arms at the elbows for patient comfort and stability with head placed between arms. • Place one sandbag across arm that is closest to the IR. • Place a second sandbag over the top of the upside humerus. • Place a third sandbag between the legs at the level of the knee while bending the legs forward. • A fourth sandbag is placed across the top of the hips to further immobilize the patient. • If a Tam-em board is used, patient position does not change from the AP projection. Turn x-ray tube for horizontal beam projection, and place vertical cassette against the lateral wall of the chest as shown . • If parental assistance is required, perform the following steps:
 position with arms extended above head to remove arms from lung field. Bend arms at the elbows for patient comfort and stability with head placed between arms. • Place one sandbag across arm that is closest to the IR. • Place a second sandbag over the top of the upside humerus. • Place a third sandbag between the legs at the level of the knee while bending the legs forward. • A fourth sandbag is placed across the top of the hips to further immobilize the patient. • If a Tam-em board is used, patient position does not change from the AP projection. Turn x-ray tube for horizontal beam projection, and place vertical cassette against the lateral wall of the chest as shown . • If parental assistance is required, perform the following steps:")
41
Central Ray • CR perpendicular to the IR centered to the midcoronal plane at the level of the mammillary (nipple) line • With use of Tam-em board, the x-ray tube centered in horizontal beam lateral position to midcoronal plane of thorax at level of mammillary line • SID of 50 to 60 inches (127 to 212 cm) Collimation Closely collimate on four sides to outer chest margins. Respiration Make exposure upon second full inspiration. If child is crying, watch respiration and make exposure when the child fully inhales.
 Collimation. Closely collimate on four sides to outer chest margins. Respiration. Make exposure upon second full inspiration. If child is crying, watch respiration and make exposure when the child fully inhales.")
42
Patient Position—With Patient Erect
• Patient is placed on seat and adjusted to correct height so top of film holder is about 1 inch (2.5 cm) above shoulders. • Arms are raised and side body clamps placed firmly against patient and secured by base adjustment and by adjustable strap. • Lead shield is raised to a level about 1 inch (2.5 cm) above iliac crest. • Correct R and L markers and inspiration marker are set to be exposed on image. • Ensure that no rotation exists. Procedure if lateral follows PA projection: If patient is already in position from the PA projection, then patient and swivel base are turned 90° to lateral position. Lead shield remains in position, and lead marker is changed to indicate correct lateral. IR is placed in film holder mount. Central Ray • CR perpendicular to IR at level of midthorax (mammillary line) • SID of 72 inches (180 cm) Collimation Collimate closely on four sides to outer chest margins. Respiration If child is crying, watch respiration and make exposure as child fully inhales and holds breath
 above shoulders. • Arms are raised and side body clamps placed firmly against patient and secured by base adjustment and by adjustable strap. • Lead shield is raised to a level about 1 inch (2.5 cm) above iliac crest. • Correct R and L markers and inspiration marker are set to be exposed on image. • Ensure that no rotation exists. Procedure if lateral follows PA projection: If patient is already in position from the PA projection, then patient and swivel base are turned 90° to lateral position. Lead shield remains in position, and lead marker is changed to indicate correct lateral. IR is placed in film holder mount. Central Ray. • CR perpendicular to IR at level of midthorax (mammillary line) • SID of 72 inches (180 cm) Collimation. Collimate closely on four sides to outer chest margins. Respiration. If child is crying, watch respiration and make exposure as child fully inhales and holds breath.")
44
Radiographic Criteria
Structures Shown: • Entire lungs from apices to costophrenic angles and from sternum anteriorly to posterior ribs. Position: • Chin and arms should be elevated sufficiently to prevent excessive soft tissues from superimposing apices. • No rotation should exist; bilateral posterior ribs and costophrenic angles should be superimposed. Collimation and CR: • Collimation borders on four sides with near equal margins on top and bottom with CR to midlung fields. Exposure Criteria: • No motion is evidenced by sharp outline of diaphragm, rib borders, and lung markings. • Sufficient exposure to faintly visualize rib outlines and lung markings through the heart shadow and upper lung region without overexposing other regions of the lungs.

46
AP and Lateral Upper Limbs

47
Technical Factors • IR size determined by the size of the patient • Grid not used for any body part smaller than 10 centimeters • Extremity/detail screens used if available • Small focal spot • 55 to 65 kV, shortest exposure time possible Shielding Secure or place lead shield over entire pelvic area. Patient Position • Place patient in the supine position. • Immobilize patient body part not to be radiographed either on the Tam-em board or with sandbags before the part to be radiographed is positioned. • When radiographing a long bone, place IR under the limb to be radiographed, including both proximal and distal joints. • When radiographing a joint, place IR under the joint to be radiographed, including a minimum of 1 to 2 inches (2.5 to 5 cm) of proximal and distal long bones.
 of proximal and distal long bones.")
48
Immobilization Immobilize the hand, forearm, and humerus with tape or compression band, or have parent immobilize while wearing lead gloves. Central Ray • CR perpendicular to the IR directed to the midpoint of the part to be radiographed • Minimum SID of 40 inches (100 cm) Collimation Collimate closely on four sides to area of interest
 Collimation. Collimate closely on four sides to area of interest.")
52
Radiographic Criteria
Position: • Generally two views 90° from each other should be obtained. (An exception is the hand requiring a PA and oblique.) Collimation and CR: • Collimation borders should be evident on four sides without cutting off essential anatomy. Exposure Criteria: • No motion is evidenced by sharp trabecular markings and bone margins. • Optimal exposure demonstrating soft tissue and joint space regions without underexposing the more dense shaft regions of long bones
 Collimation and CR: • Collimation borders should be evident on four sides without cutting off essential anatomy. Exposure Criteria: • No motion is evidenced by sharp trabecular markings and bone margins. • Optimal exposure demonstrating soft tissue and joint space regions without underexposing the more dense shaft regions of long bones.")
53
AP and Lateral Lower Limbs

54
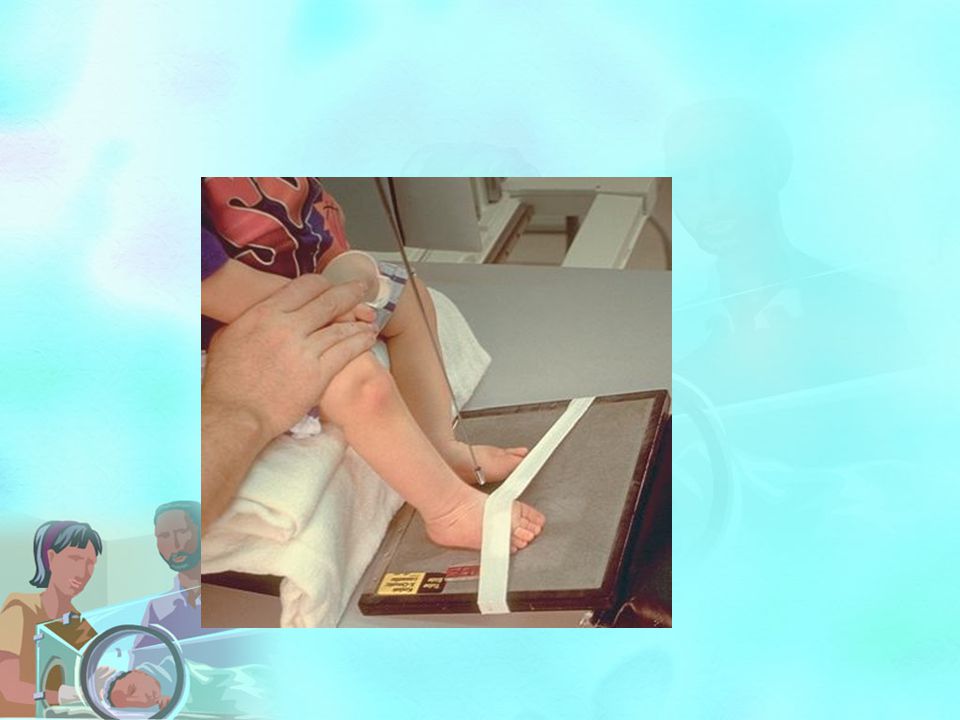
Technical Factors • IR size determined by the size of the body part to be radiographed, IR crosswise • Grid not necessary for infants and small children • 60 to 70 kV, shortest exposure time possible • Small focal spot Shielding Male or female gonadal shields correctly placed so as not to obscure hips and proximal femora Patient Position and Central Ray AP and lateral • Patient is supine with IR under patient centered to affected limb or placed diagonally for bilateral limbs if needed to include entire limbs from hips to feet. • Immobilize with tape and/or compression band, or have parent hold leg in position with one hand on the pelvis above the hip region and one hand holding the foot (wearing lead gloves and apron.) • For lateral, rotate leg externally and immobilize with tape, or have parent hold as for AP projection. • For bilateral limbs, abduct both limbs into “frog-leg” position. Immobilize with tape or compression band across knees and/or ankles. • CR is perpendicular to mid area of limbs. • Minimum SID is 40 inches (100 cm).
 • For lateral, rotate leg externally and immobilize with tape, or have parent hold as for AP projection. • For bilateral limbs, abduct both limbs into frog-leg position. Immobilize with tape or compression band across knees and/or ankles. • CR is perpendicular to mid area of limbs. • Minimum SID is 40 inches (100 cm).")
60
KUB abdomen, AP erect Lateral and dorsal decubitus

61
• IR size—determined by the size of patient, IR lengthwise
Technical Factors • IR size—determined by the size of patient, IR lengthwise • High-speed film-screen • Moving or stationary grid, if 10 cm or larger • 65 to 85 kV NB to 18 years, shortest exposure time possible Shielding • Gonadal shield on all males—size appropriate for age (tape shield in place) • No gonadal shielding on females Patient and Part Position • Patient is supine, aligned to midline of table and/or cassette. • Immobilize with soft flexible sandbags and compression band. Newborns and young infants • Position the arms away from the body and mold a large flexible sandbag over each arm. Because it is difficult to straighten the little, short legs of infants, place one sandbag under their knees and another over the top to immobilize their legs. Babies, if they feel snug and warm, are usually calm unless they are in pain. If a baby is crying, a pacifier may help and will not interfere with the exam.
 • No gonadal shielding on females. Patient and Part Position. • Patient is supine, aligned to midline of table and/or cassette. • Immobilize with soft flexible sandbags and compression band. Newborns and young infants. • Position the arms away from the body and mold a large flexible sandbag over each arm. Because it is difficult to straighten the little, short legs of infants, place one sandbag under their knees and another over the top to immobilize their legs. Babies, if they feel snug and warm, are usually calm unless they are in pain. If a baby is crying, a pacifier may help and will not interfere with the exam.")
62
Infants and toddlers • Restrain the arms the same as for younger infants. Place a sandbag under the knees and tighten a compression band over both femora and knees. Be sure to place padding under the band so that it does not cut into the child's legs. Compression bands on most x-ray tables are designed for adults, so this restraint works best if the spaces between the band and the patient are padded with foam sponges or towels. If parents are providing assistance, do the following: •Provide parent with lead apron and gloves. •Position tube and cassette and set exposure factors before positioning. •Position patient so that technologist's view is not obstructed. •Usually, it is necessary to have a parent hold only the child's arms. The legs can be satisfactorily immobilized as described above.

64
Central Ray • With infants and small children, CR and cassette centered 1 inch (2.5 cm) above the umbilicus • With older children and adolescents, CR centered at the level of iliac crest • Minimum SID of 40 inches (102 cm) Respiration • With infants and children, watch the breathing pattern. When the abdomen is still, make the exposure. If the patient is crying, make the exposure as the baby takes a breath to let out a cry. • Children over 5 years of age usually can hold their breath after a practice session. Radiographic Criteria
 Respiration. • With infants and children, watch the breathing pattern. When the abdomen is still, make the exposure. If the patient is crying, make the exposure as the baby takes a breath to let out a cry. • Children over 5 years of age usually can hold their breath after a practice session. Radiographic Criteria.")
65
Structures Shown: • Soft tissue border outlines and gas-filled structures such as the stomach and intestines, calcifications (if present), and faint bony skeletal structures are shown. Position: The vertebral column is aligned to the center of the radiograph. • No rotation should exist: pelvis, hips, and lower rib cage should be symmetric. Collimation and CR: Collimation borders from symphysis pubis to diaphragm and to bilateral borders of abdomen. Exposure Criteria: No motion should be evident, and diaphragm and gas patterns should appear sharp. • Optimal contrast and exposure will visualize bony structure outlines such as ribs and vertebrae through abdominal contents without overexposing gas-filled structures.

67
AP Erect

68
Respiration • With infants and children, watch the breathing pattern. When the abdomen is still, make the exposure. If the patient is crying, make the exposure as the baby takes a breath in to let out a cry. • Children older than 5 years of age usually can hold their breath after a practice session

71
Radiographic Criteria
Structures Shown: • Entire contents of abdomen, including gas patterns and air-fluid levels and soft tissue if not obscured by excessive fluid in distended abdomen. Position: • The vertebral column is aligned to the center of the radiograph. • No rotation should exist: pelvis and hips should be symmetric. Collimation and CR: • Collimation to borders of abdomen from symphysis pubis to diaphragm. Exposure Criteria: • No motion should be evident, and diaphragm and gas pattern borders should appear sharp. • Bony pelvis and vertebral body outlines should be evident through abdominal contents without overexposing air-filled structures.

72
Lateral Decubitus and Dorsal Decubitus

73
Lateral decubitus • Patient on side on a radiolucent foam block with back against IR • Horizontal CR directed to 1 inch (2.5 cm) superior to umbilicus Dorsal decubitus • Patient is supine on a rectangular radiolucent foam block. • Legs are immobilized with sandbags as for a supine AP abdomen. • Gently pull arms above head and ask parent to hold arms and head with newborn or small infant. • Place IR lengthwise, parallel to the midsagittal plane against side of patient (support with cassette holder device or with sandbags).
 superior to umbilicus. Dorsal decubitus. • Patient is supine on a rectangular radiolucent foam block. • Legs are immobilized with sandbags as for a supine AP abdomen. • Gently pull arms above head and ask parent to hold arms and head with newborn or small infant. • Place IR lengthwise, parallel to the midsagittal plane against side of patient (support with cassette holder device or with sandbags).")
76
Radiographic Criteria (Dorsal Decubitus)
Structures Shown: • Abdominal structures in the prevertebral region as well as air-fluid levels within abdomen; diaphragm included superiorly and pelvis and hips inferiorly. Position: • No rotation should exist: posterior ribs should be superimposed. Collimation and CR: • At least minimal collimation borders should be visible on four sides, with center of collimation field (CR) to midcoronal plane, midway between diaphragm and symphysis pubis. Exposure Criteria: • No motion should be evident, and diaphragm and gas patterns should appear sharp. • Abdominal soft tissue detail should be visible without overexposing gas-filled structures. • Faint rib outlines should be visible through abdominal contents
 to midcoronal plane, midway between diaphragm and symphysis pubis. Exposure Criteria: • No motion should be evident, and diaphragm and gas patterns should appear sharp. • Abdominal soft tissue detail should be visible without overexposing gas-filled structures. • Faint rib outlines should be visible through abdominal contents.")
Similar presentations





























. Step by Step Guide to a Typical Radiographic Examination Request Form Check form is fully completed and signed. Check pregnancy question.>")

. Perioperative nursing handbook. (p. 165-167).>")

.>")













