Download presentation
Presentation is loading. Please wait.

1
ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal

2
stem cells Lymphocytes Mature in B.marrow to become “B LYMPHOCYTE” react with free antigen directly Thymus T cells recognise the antigen with the help of macrophages activated lymphocytes enter the tissue and meet antigen again results in multiplication and secretion of cytokines or immunoglobins in order to destroy the antigen plasma cells Cytotoxic T cells Helper T cells (CD4 surface protein) Th1 cells - involved in cell mediated immunity. Produce interferon gamma, interleukin 2 & TNF beta. Th2 cells: play a role in humoral responses responsible for Atopy and allergy

3
Immune response in T.B. Infection It manages to evoke both immunity & hypersensitivity in the body Immunity – Good for body –not good for bacteria It localizes the bacteria and clears the infection efficiently with out causing much tissue destruction Hypersensitivity – good for bacteria – not good for body Infection can not be localized Plenty of tissue destruction with on going caseation & necrosis

6
Introduction Tuberculosis and HIV - closely linked since the emergence of AIDS. HIV infection has contributed to a significant increase in the worldwide incidence of tuberculosis Over 4 million persons worldwide have been infected with HIV and tuberculosis Most common cause of death in AIDS patients

7
Have instantly clicked together & linked since the emergence of AIDS Love at first sight No generation gap

8
T.B. HIV HIV & TB both affect each other

9
T.B. HIV Effect of HIV on TB

10
HIV increases the incidence of TB

11
Now answer these 2 questions: What % of world population get Mycobacterium infection at some point in their life (without developing active disease) ? Of them how many of develop active disease ?

12
HIV increases the T.B. infection It is estimated that 1/3 rd population of the world are infected by the Mycobacterium tuberculosis Out of them only 10% have life time chances of developing tuberculosis This scenario is changing with the advent of HIV infection

13
Tuberculosis normally develop through:- 1.progression of recently acquired infection - primary disease 2.reactivation of latent infection 3.exogenous reinfection

14
Concomitant HIV infection increases the possibility of development of T.B. in all the above categories People co-infected with both HIV and latent TB have an up to 800% greater risk of developing active tuberculosis disease and becoming infectious compared to people not infected with HIV

15
Gohn focus

17
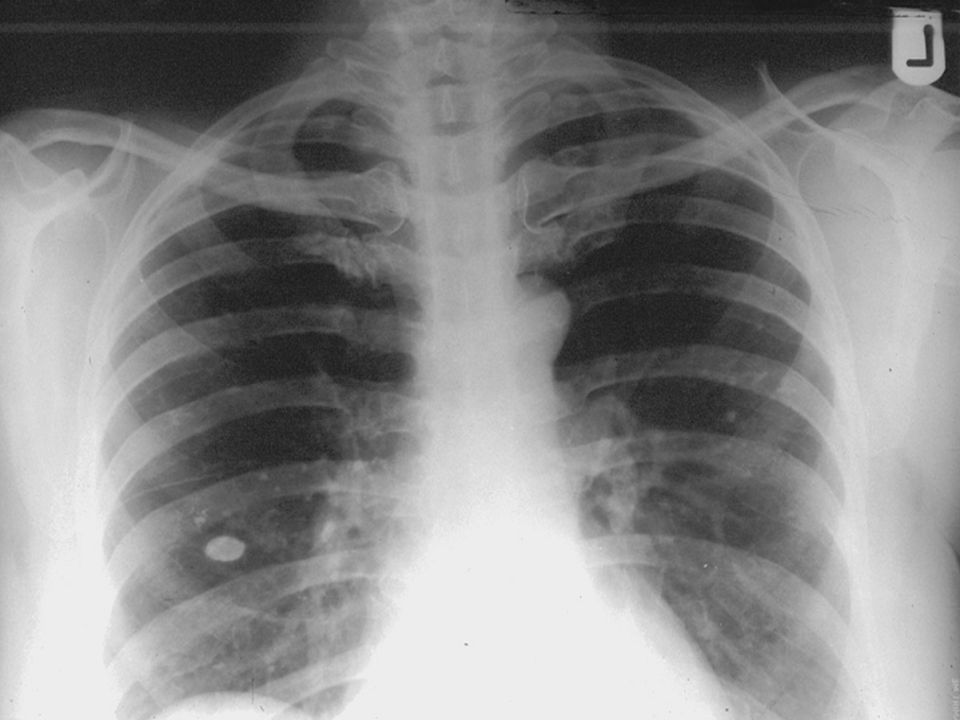
Now answer these questions: What is the main lesion in post primary T.B. What is the main lesion in post primary T.B. Is there hilar lymphadenopathy Is there hilar lymphadenopathy Which lobes are predominently affected Which lobes are predominently affected What is the likelihood of pleural effusion What is the likelihood of pleural effusion

18
Clinical features of HIV-associated post primary pulmonary tuberculosis (in adults) are frequently atypical, particularly in the late stage of HIV infection 1. Non-cavitary disease 2. Lower lobe infiltrates 3. Hilar lymphadenopathy 4. Pleural effusion -Lack of hypersensitivity Lack of immunity

19
Immunity Hypersensitivity

20
Tuberculosis can be a relatively early manifestation of HIV-1 infection Risk of developing tuberculosis, and of disseminated infection, increases as the CD4 T-cell count decreases

21
Immune system is unable to contain the infection resulting in: An increased frequency of extrapulmonary tuberculosis Positive mycobacterial blood cultures Atypical chest radiographic findings

22
Patients with extrapulmonary tuberculosis may present with signs and symptoms specific to the involved site, such as lymphadenopathy headache meningismus pyuria abscess formation back pain abdominal pain

23
Increased incidence of MDR TB in HIV Acquired resistance ( Organisms are sensitive at the beginning) in MDR TB is associated with co- infection due to HIV & tuberculosis In MDRTB outbreaks approximately 90% of the cases were HIV seropositive
 in MDR TB is associated with co- infection due to HIV & tuberculosis In MDRTB outbreaks approximately 90% of the cases were HIV seropositive")
24
Spread of TB poses a serious threat to the world health scenario Multi Drug Resistant

25
Summary Effect of HIV on TB: 1.Increases the incidence of TB by converting the latent infection into active one 2.Changes the clinical features of the post primary tuberculosis non-cavitary disease lower lobe infiltrates hilar lymphadenopathy pleural effusion More extrapulmonary involvement 3. Increased incidence of MDR TB in HIV

26
T.B. HIV

27
T.B. – opportunistic infection in HIV/AIDS Relatively early manifestation of HIV-1 infection median CD4 T-cell count was >300 cells/mm3 Risk of developing tuberculosis & of disseminated infection, increases as the CD4 T-cell count decreases What is normal CD4 cell count ? 600 -1200/ml

28
AIDS generally occurs when CD4 count is below 200/mL or a CD4 lymphocyte percentage below 14% Characterized by the appearance of opportunistic infections, eg.: Tuberculosis Pneumocystis carinii pneumonia Toxoplasmosis Meningitis and other brain infections Fungal infections Malignancies: lymphoma, cervical Ca., Kaposi's sarcoma

29
Tuberculosis acts to accelerate the clinical course of HIV infection 5- to 160-fold increase in viral replication during the acute phase of untreated tuberculosis leads to increased HIV viral load

30
Clinical Presentation of Tuberculosis with HIV

31
Diagnostic difficulties initially because the early symptom - fever, weight loss, and malaise in both TB & HIV are same Diagnostic difficulties initially because the early symptom - fever, weight loss, and malaise in both TB & HIV are same Earlier in the course of HIV disease TB is more likely to present as classical reactivation-type disease Earlier in the course of HIV disease TB is more likely to present as classical reactivation-type disease Patients with advanced immuno suppression are more likely to present with findings consistent with primary tuberculosis Patients with advanced immuno suppression are more likely to present with findings consistent with primary tuberculosis

32
bilateral hilar lymphadenopathy with diffuse interstitial and airspace opacities. CD4 count<200

34
Extensive right paratracheal lymphadenopathy

35
Treatment of HIV-Related Tuberculosis

36
Good, early clinical response to therapy as long as the regimen contains INH and a Rifampicin Good, early clinical response to therapy as long as the regimen contains INH and a Rifampicin Sputum culture conversion & treatment failure rates were similar to those in patients without HIV infection Sputum culture conversion & treatment failure rates were similar to those in patients without HIV infection

37
Treatment of HIV & TB together poses many problems

38
Requires close monitoring because Requires close monitoring because 1. Development of resistance 2. Frequent drug toxicities 3. Possible drug-drug interactions 4. Paradoxical reactions

39
Rifamycins: Rifampicin or Rifampin Rifampicin or Rifampin Rifabutin Rifabutin Rifapentine – long acting so only once a week dose required Rifapentine – long acting so only once a week dose required

40
Patients treated with a once-weekly Isoniazid /Rifapentine continuation-phase regimen Relapse with rifamycin monoresistant T.B. In HIV-seropositive tuberculosis Patients treated with a once-weekly Isoniazid /Rifapentine continuation-phase regimen Relapse with rifamycin monoresistant T.B. In HIV-seropositive tuberculosis HIV-seropositive people with tuberculosis should not be treated with a once-weekly isoniazid/rifapentine regimen HIV-seropositive people with tuberculosis should not be treated with a once-weekly isoniazid/rifapentine regimen

41
Adverse drug reactions Most commonly seen with Rifampicin Most commonly seen with Rifampicin Rifampicin should be avoided/replaced Rifampicin should be avoided/replaced Rash - Thiacetazone should not be used in the treatment of HIV-related tuberculosis because of skin reactions Rash - Thiacetazone should not be used in the treatment of HIV-related tuberculosis because of skin reactions Paresthesia – B6 should be given with INH Paresthesia – B6 should be given with INH Incidence of drug induced hepatitis is many times more in HIV+ TB patients - Frequent monitoring of liver function tests are required Incidence of drug induced hepatitis is many times more in HIV+ TB patients - Frequent monitoring of liver function tests are required

42
Drug-Drug Interactions

43
Certain antituberculosis drugs may interact adversely with medications commonly used by HIV-infected individuals Rifamycin derivatives Rifampicin (most potent inducer) Rifabutin Rifapentine (less potent) induce the hepatic cytochrome P450 enzyme system
 Rifabutin Rifapentine (less potent) induce the hepatic cytochrome P450 enzyme system")
44
Results in increased metabolism & reduced serum levels of certain drugs which includes protease inhibitors (PIs) nonnucleoside reverse transcriptase inhibitors (NNRTIs) Used for the treatment of AIDS
 nonnucleoside reverse transcriptase inhibitors (NNRTIs) Used for the treatment of AIDS")
45
This results in subtherapeutic levels and the potential development of viral resistance to these important agents Rifabutin can be substituted for Rifampicin in the treatment regimen

46
PIs and NNRTIs affect the metabolism of rifabutin, resulting in altered serum levels and the possibility of drug toxicity, adjustments in rifabutin dosage are often necessary Patients can take the standard rifampin-based treatment regimen if not taking PIs or NNRTIs

47
Paradoxical Reactions

48
Temporary exacerbation of symptoms, signs, or radiographic manifestations of tuberculosis seen after beginning ATT Occur in HIV-infected patients with active tuberculosis Develop after simultaneous administration of both antiretroviral & ATT

49
Due to increase in the cellular immunity caused by ART Diagnosis of a paradoxical reaction should be made after a thorough evaluation to exclude other etiologies, such as tuberculosis treatment failure

50
Initiation of Antiretroviral Therapy in coinfected Patient. Lot of confusion & uncertainity prevails at present No standard regimens!

51
So don’t start fighting over it!

52
Initiation of Antiretroviral Therapy in coinfected Patient Treatment of tuberculosis to be initiated immediately Treatment of HIV infection usually started after 2 months potentially decreasing the risk of a paradoxical reaction Tuberculosis and HIV can be treated concurrently using a Rifabutin-based regimen

53
Whether to start ART as soon as possible or wait until antituberculosis treatment is well established is not clear at present Decision should be made on a case-by-case basis If already receiving ART, regimen to be continued and modifications to either the tuberculosis regimen or to the antiretroviral regimen can be made as indicated

54
Many of the side effects like GIT upset Rash Preipheral neuropathy Flu like symptoms Can be due to both ATT or ART In case of ATT, they can be with held and started one by one again This can not be done with ART – resistance. So treatment guided by prior knowledge

55
Latent Tuberculosis Infection positive tuberculin skin test for HIV infected persons is >=5 mm Prevalence of (+) test decrease with decreasing CD4 T-cell counts Persons with low CD4 T lymphocyte count should have periodic X ray chest done esp. in high risk group Why?

56
HIV-infected individuals with latent TB infection have an extraordinarily high rate of progression to active tuberculosis compared to HIV-uninfected persons Treatment of LTBI very effective in preventing persons infected with M tuberculosis from developing active disease Annual screening of all HIV-infected persons for LTBI, and treatment of those coinfected with M tuberculosis, is recommended

57
OptionTotal Duration (months) Initial PhaseContinuation Phase DrugsInterval and Duration* DrugsInterval and Duration # I6 INH RIF PZA EMB (or SM) (HRZEorS) Daily for 8 weeks INH RIF (HR) Daily for 16 weeks or Twice weekly for 16 weeks II6 INH RIF PZA EMB (or SM) (HRZEorS) Daily for 2 weeks then Twice weekly for 6 week INH RIF Twice weekly for 18 weeks III6 INH RIF PZA EMB (or SM) (HRZEorS) Thrice weekly for 26 weeks Recommended regimen
 Initial PhaseContinuation Phase DrugsInterval and Duration* DrugsInterval and Duration # I6 INH RIF PZA EMB (or SM) (HRZEorS) Daily for 8 weeks INH RIF (HR) Daily for 16 weeks or Twice weekly for 16 weeks II6 INH RIF PZA EMB (or SM) (HRZEorS) Daily for 2 weeks then Twice weekly for 6 week INH RIF Twice weekly for 18 weeks III6 INH RIF PZA EMB (or SM) (HRZEorS) Thrice weekly for 26 weeks Recommended regimen")
58
DrugsDuration (months) Interval Comments Isoniazid9 Daily or Twice weekly Directly observed therapy if given twice weekly. Isoniazid may be used with nucleoside and nonnucleoside reverse transcriptase and protease inhibitors. Rifampin+ pyrazinamide 2 2 - 3 Daily Twice weekly Directly observed therapy if given twice weekly. Rifampin may be used with certain combinations of protease inhibitors. Rifampin*4 DailyUse if patient unable to tolerate isoniazid or pyrazinamide. Rifampin may be used with certain combinations of protease inhibitors

Similar presentations