Download presentation
Presentation is loading. Please wait.

1
NASBS-2007 Endoscopic Cranial Base Neuroanatomy as Observed through Endonasal Transphenoidal Approach Promod Pillai, Mario Ammirati

2
ESBS 2007 Evolution of Skull base Neurosurgery Pioneers ( 19 th Century) Francesco Durante (1845-1934)-olfactory groove meningioma Francesco Durante (1845-1934)-olfactory groove meningioma Charles Balance-earliest case of acoustic tumor removal Charles Balance-earliest case of acoustic tumor removal Fedor Krause (1857-1937) Fedor Krause (1857-1937) de Martel( 1875-1940) de Martel( 1875-1940)
 Francesco Durante ( )-olfactory groove meningioma Francesco Durante ( )-olfactory groove meningioma Charles Balance-earliest case of acoustic tumor removal Charles Balance-earliest case of acoustic tumor removal Fedor Krause ( ) Fedor Krause ( ) de Martel( ) de Martel( )")
3
ESBS 2007 Neurosurgery has changed !

4
ESBS 2007 Evolution of Skull base Neurosurgery Early 20 th Century Early 20 th Century Harvey Cushing(1869-1939) Harvey Cushing(1869-1939) Walter Dandy (1886-1946) Walter Dandy (1886-1946) Hertbert Olivecrona(1891-1980) Hertbert Olivecrona(1891-1980) Charles Frazier(1870-1936) Charles Frazier(1870-1936)
 Harvey Cushing( ) Walter Dandy ( ) Walter Dandy ( ) Hertbert Olivecrona( ) Hertbert Olivecrona( ) Charles Frazier( ) Charles Frazier( )")
5
ESBS 2007 Evolution of Skull Base Surgery Contemporary Skull Base Surgery Contemporary Skull Base Surgery Al-Mefty Al-Mefty Dolenc Dolenc Jannetta Jannetta Rhoton Rhoton Samii Samii Sen Sen Sekhar Sekhar Spetzler Spetzler Yasargil Yasargil many more ! many more !

6
ESBS 2007 Present status of Skull base Surgery Significant attention and interest in the recent past. Significant attention and interest in the recent past. Skull Base Surgery has benefited from Advances – Imaging and diagnostic technology, Skull Base Surgery has benefited from Advances – Imaging and diagnostic technology, Surgical instrumentation, Reconstructive techniques Surgical instrumentation, Reconstructive techniques

7
ESBS 2007 Criticism for Skull Base Surgery Skull base surgeons seemed more interested in the surgery itself than in patients! Is there any justification of Skull base Surgery programs! Is there any future for Skull Base Surgery?

8
ESBS 2007 Criticism for Skull Base Surgery Whom to blame? Whom to blame? Only the preoperative and postoperative images were shown demonstrating “complete removal” of the lesions! No history or clinical findings given ! What is the quality of life after surgery ?

9
ESBS 2007 Future of Skull Base Surgery Quality of life matters! Quality of life matters!

10
ESBS 2007 Future of Skull Base Surgery Adaptation, modification, and expansion of existing techniques or technologies (often from other specialties) have been hallmarks of surgical advancement Innovation and creativity have been driving forces behind surgical progress.
 have been hallmarks of surgical advancement Innovation and creativity have been driving forces behind surgical progress.")
11
ESBS 2007 Multidisciplinary Approach

12
ESBS 2007 Alternatives or adjuvants to Armamentarium? Stereotactic Radiosurgery Endoscope Endovascular Therapy Molecular Therapy

13
ESBS 2007

14
Mile stone of modern and contemporary neurosurgery in the treatment of pituitary tumors

15
ESBS 2007 Endoscopic Cranial Base Anatomy Objective Learn and familiarize with cranial base anatomy Learn and familiarize with cranial base anatomy as viewed through sphenoid sinus using endoscope as viewed through sphenoid sinus using endoscope

16
ESBS 2007 Endoscopic Cranial Base Anatomy Material and methods Six freshly frozen cadaver heads Endoscopes Angled lenses for peripheral structures Dissection was guided with frame less stereotaxy

17
ESBS 2007 Endoscopic Cranial Base Anatomy Preliminary dissection Nasal Cavities Four walls and 2 opening

18
ESBS 2007 Endoscopic Cranial Base Anatomy Nasal Cavity Walls Inferior wall- Floor Medial wall- septum Lateral nasal wall Superior wall Roof Superior wall Roof

19
ESBS 2007 Endoscopic Cranial Base Anatomy Nasal Cavity OpeningsAnteriorPosterior

20
ESBS 2007 Endoscopic Cranial Base Anatomy Medial wall “Septum” “Septum”

21
ESBS 2007 Endoscopic Cranial Base Anatomy Lateral wall

22
ESBS 2007 Endoscopic Cranial Base Anatomy Sphenoid sinus

23
ESBS 2007 Endoscopic Cranial Base Anatomy Exposure of suprasellar region

24
ESBS 2007 Endoscopic Cranial Base Anatomy Exposure of retro sphenoid area

25
ESBS 2007 Endoscopic Cranial Base Anatomy Exposure of para sellar area

26
ESBS 2007 Endoscopic Cranial Base Anatomy Discussion

27
ESBS 2007 Transphenoidal surgery Advantages 1.Excellent three dimensional view 1.Excellent three dimensional view 2.Easy manipulation of zoom and focus features 2.Easy manipulation of zoom and focus features 3.Speculum protects the mucosa from instruments injury 3.Speculum protects the mucosa from instruments injury 4.Better manipulability of instruments 4.Better manipulability of instruments

28
ESBS 2007 Transphenoidal surgery Possible drawbacks Limited exposure and Limited working space Limited exposure and Limited working space Narrow field of view - “Cant work around the corner” Narrow field of view - “Cant work around the corner” Failure to visualize optic chiasma /suprasellar space during transdiaphramatic dissection Failure to visualize optic chiasma /suprasellar space during transdiaphramatic dissection Sinonasal complications, patient discomfort Sinonasal complications, patient discomfort

29
ESBS 2007 Neuroendoscopy, past, present and future Early history Max Nitze- First endoscope 1879 Max Nitze- First endoscope 1879 L'Espinasse(1910) first neuroendoscopic procedure using cystoscope L'Espinasse(1910) first neuroendoscopic procedure using cystoscope Walter Dandy(1922)- Choroid Plexectomy Walter Dandy(1922)- Choroid Plexectomy
 first neuroendoscopic procedure using cystoscope L Espinasse(1910) first neuroendoscopic procedure using cystoscope Walter Dandy(1922)- Choroid Plexectomy Walter Dandy(1922)- Choroid Plexectomy")
30
ESBS 2007 Neuroendoscopy, past, present and future Decline Technical difficulties and high death rates Development of microneurosurgery(1960’s) As microneurosurgery gained popularity, the use of endoscopy waned further.
 As microneurosurgery gained popularity, the use of endoscopy waned further.")
31
ESBS 2007 Neuroendoscopy, past, present and future Rediscovery of endoscope with technical advances New lens types -“SELFOC” lens New lens types -“SELFOC” lens Invention of computer chip television video cameras and CCDs( Charge Coupled Devices) Invention of computer chip television video cameras and CCDs( Charge Coupled Devices) Fiberoptics Fiberoptics
 Invention of computer chip television video cameras and CCDs( Charge Coupled Devices) Fiberoptics Fiberoptics")
32
ESBS 2007 Neuroendoscopy, past, present and future Rediscovery of Neuroendoscopy ETV-The success of neuroendoscopy in recent years has relied heavily on the success of ETV for the treatment of obstructive hydrocephalus ETV-The success of neuroendoscopy in recent years has relied heavily on the success of ETV for the treatment of obstructive hydrocephalus Intraventricular tumors, skull base tumors, craniosynostosis, degenerative spine disease, intracranial cysts, and rare subtypes of hydrocephalus

33
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Present status endoscopic transnasal, nontransseptal, transsphenoidal pituitary surgery endoscopic transnasal, nontransseptal, transsphenoidal pituitary surgery Jho and Carrau 1990s Jho and Carrau 1990s Kassam and Snyderman Kassam and Snyderman Cappabianca and de Divitiis Cappabianca and de Divitiis Frank et al Frank et al

34
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Present status “Stone in the pond effect!!” “Stone in the pond effect!!” de Divitiis E, Neurosurgery. 2006 Sep;59(3):512-20
:")
35
ESBS 2007 Endoscopic Pituitary Surgery Otolaryngeological advantages Avoids -perforation, septal deformity, saddle nose deformity, nasal obstruction, and long-term epistaxis and crusting Avoids -perforation, septal deformity, saddle nose deformity, nasal obstruction, and long-term epistaxis and crusting

36
ESBS 2007 Endoscopic Pituitary Surgery Otolaryngeological advantages Avoids possible dental complications from the sublabial approach Avoids possible dental complications from the sublabial approach Rapid recovery from the otolaryngologic aspect of the surgery Rapid recovery from the otolaryngologic aspect of the surgery Reduced Postoperative discomfort-pain, Hospital stay Reduced Postoperative discomfort-pain, Hospital stay

37
ESBS 2007 Endoscopic Pituitary Surgery Neurosurgical advantages smaller bony opening makes the reconstruction quicker and easier smaller bony opening makes the reconstruction quicker and easier Argument against Anterior wall of spehenoid sinus is removed-tight recconstrucion and packing may be difficult- Bigger sphenoid opening Anterior wall of spehenoid sinus is removed-tight recconstrucion and packing may be difficult- Bigger sphenoid opening

38
ESBS 2007 Endoscopic Pituitary Surgery Neurosurgical advantages “less aggressive and more precise than traditional surgery” “less aggressive and more precise than traditional surgery” “Least traumatic” “Least traumatic” Argument against Binasal endoscopic approach is “more invasive” Binasal endoscopic approach is “more invasive” Possibility of injury to septal mucosa/middle turbinate Possibility of injury to septal mucosa/middle turbinate

39
ESBS 2007 Endoscopic Pituitary Surgery Neurosurgical advantages Visualization of the lateral sphenoid wall including the carotid arteries and optic nerves Visualization of the lateral sphenoid wall including the carotid arteries and optic nerves Direct visualization of normal pituitary and dura Direct visualization of normal pituitary and dura

40
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Pitfalls Pitfalls Less familiarity- “learning curve” Less familiarity- “learning curve” Limited Zoom capability Limited Zoom capability Need for refocus maneuvers Need for refocus maneuvers Possibility of injury to septal mucosa/middle turbinate Possibility of injury to septal mucosa/middle turbinate

41
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Pitfalls Pitfalls The scope greatly limits the degrees of freedom of the other instruments, making instrument manipulations difficult and often ineffective The scope greatly limits the degrees of freedom of the other instruments, making instrument manipulations difficult and often ineffective Binasal endoscopic approach is “more invasive” Binasal endoscopic approach is “more invasive” Visualization is not synonymous with operability Visualization is not synonymous with operability

42
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Pitfalls Pitfalls Two dimensional “Flat” Images- No depth perception Anterior wall of spehenoid sinus is removed-tight recconstrucion and packing may be difficult- Bigger sphenoid opening Difficulty in Reconstruction – esp with extended endonasal approaches

43
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Average duration of surgery- Minutes Endoscopic surgery 98 Microscopic surgery 106 Endoscopic repeat surgery 107 Microscopic repeat surgery 129 Frank G et al Neuroendocrinology. 2006;83(3-4):240-8.
:")
44
ESBS 2007 Outcome Laws ER Jr et al Clinical series of 3093 patients of transphenoidal surgery- J Am Coll Surg. 2001 Dec;193(6):651-9
:")
45
ESBS 2007 Repeated transsphenoidal surgery to treat recurrent or residual pituitary adenoma. Benviniste et al J Neurosurg. 2005 Jun;102(6):1004-12 96 patients 96 patients No mortality Morbidity – 1% Remission 93% for non functioning 57 % for functioning adenomas 57 % for functioning adenomas 3 rd surgery in about 10% patients
: patients 96 patients No mortality Morbidity – 1% Remission 93% for non functioning 57 % for functioning adenomas 57 % for functioning adenomas 3 rd surgery in about 10% patients.")
46
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Complications in Endoscopically treated patients with recurrent tumors- CSF leak during surgery 7 (35%) CSF leak after surgery 1 ( 5%) Pneumoencephalocele 1 (5%) Diabetes insipidus 0 Hypofunction of the anterior lobe 3 (15%) Frank G et al Neuroendocrinology. 2006;83(3-4):240-8
:")
47
ESBS 2007 Complications Endoscopy Vs Transphenoidal Fully endoscopic *Transseptal−trans− 300 patients sphenoidal- Nasal septum perforation 0.7 6.7 Postoperative epistaxis 1.3 10 Anterior pituitary insufficiency 2.7 19.4 Diabetes insipidus 5.3 17.8 Loss of vision None 1.8 Carotid artery injury None 1.1 CNS injury None 1.3 Intrasellar hemorrhage 0.7 2.9 Cerebrospinal fluid leak 1.7 3.9 Meningitis None 1.5 Death None 0.9 Kabil MS et al Minim Invasive Neurosurg. 2005 Dec;48(6):348-54 *Results of a National survey (Ciric et al., 1997).
: *Results of a National survey (Ciric et al., 1997)..")
48
ESBS 2007 Authors- YearPatients Bleedin g Trans DI- Perm -DI CSF leakmeningitis Pituitary dysfunctio n visual lossRemission Kelly RT-20069017 2 Shaw-200426 15 Rudnik-200570 4.300 71 Rudnik A-2006125 7 73 Netea-Maier- 200535 77 Kabil -20053002 5.31.7 2.7 87-93 Jho HD-2001128 4361.211 78 Kenan K-2006781.25.11.22.4 50-66 Cappabianca- 20021461.4 3.43 13.1 Endoscopic Pituitary Surgery- Clinical series

49
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Progression of technique Endoscopy has stimulated new applications of relatively a static surgical technique Endoscopy has stimulated new applications of relatively a static surgical technique

50
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Recent advances Recent advances Description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches Description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches Emergence of “Endoneurosurgeons” Emergence of “Endoneurosurgeons” Expanded endonasal approaches- frontal sinus to C2 in the sagittal plane and from the sella to the jugular bulb in the coronal plane Expanded endonasal approaches- frontal sinus to C2 in the sagittal plane and from the sella to the jugular bulb in the coronal plane

51
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Extended approaches Extended approaches Modifications of standard endoscopic Modifications of standard endoscopic transphenoidal approach allow additional exposure to other cranial base lesions Exposure from planum sphenoidale to craniovertebral junction. Exposure from planum sphenoidale to craniovertebral junction.

52
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Challenges of extended approaches Challenges of extended approaches Proper selection of the patients Proper selection of the patients Potential success also depends on anatomy, consistency, blood supply and relationship to neurovascular structures Potential success also depends on anatomy, consistency, blood supply and relationship to neurovascular structures Reconstruction of Skull Base Reconstruction of Skull Base

53
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Criticisms of extended approaches Criticisms of extended approaches Is it really minimally invasive? Is it really minimally invasive? Usefulness in intradural/arachnoidal lesion Usefulness in intradural/arachnoidal lesion Managing intraoperative catastrophes Managing intraoperative catastrophes Proper Skull base reconstruction and avoidance of CSF leak Proper Skull base reconstruction and avoidance of CSF leak

54
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Criticisms of extended approaches Criticisms of extended approaches The claim that endoscopic surgery is superior to endonasal surgery is sometimes seen as a marketing device to try to change traditional patterns of referral for pituitary surgery

55
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques We know that the endoscopic techniques in skull base surgery is going to stay We know that the endoscopic techniques in skull base surgery is going to stay But we need to know – But we need to know – are we dealing with treatment modality which provides significant advantage over the conventional modality in terms of short and long term outcomes? are we dealing with treatment modality which provides significant advantage over the conventional modality in terms of short and long term outcomes? Is it a replacement or adjuvant ? Is it a replacement or adjuvant ?

56
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques We clearly need to have outcome studies which address Extent of tumor removal Extent of tumor removal Tumor recurrence/residue Tumor recurrence/residue Surgical morbidities Surgical morbidities Reconstruction of anatomy Reconstruction of anatomy

57
ESBS 2007 Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region

58
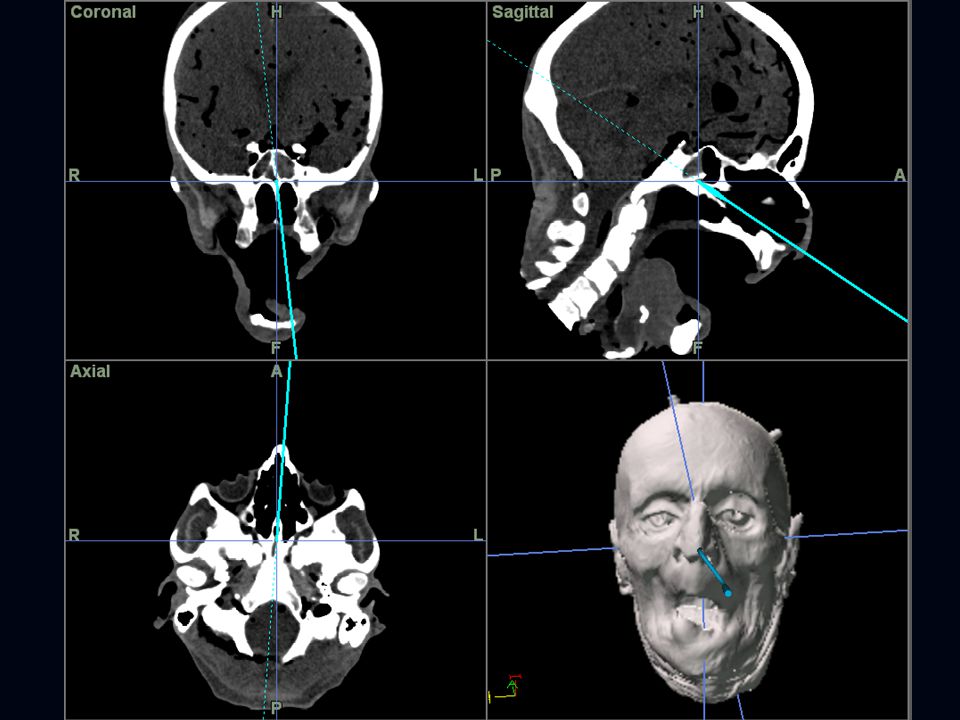
ESBS 2007 Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region Endonasal transphenoidal approaches were performed in freshly frozen cadaver heads using both endoscope and microscope Endonasal transphenoidal approaches were performed in freshly frozen cadaver heads using both endoscope and microscope Using Image guidance, we have attempted to quantify the surgical exposure in each approaches Using Image guidance, we have attempted to quantify the surgical exposure in each approaches

60
ESBS 2007 Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region Results Endoscopic approach provided a panoramic view Endoscopic approach provided a panoramic view Exposure in axial and sagittal planes were significantly improved Exposure in axial and sagittal planes were significantly improved Better visualisation of the supradiaphramatic structures, area behind the anterior wall of the sella Better visualisation of the supradiaphramatic structures, area behind the anterior wall of the sella

61
ESBS 2007 Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region Results No significant exposure advantage in the coronal plane compared with microscopic approach No significant exposure advantage in the coronal plane compared with microscopic approach There was limitation of exposure in the coronal plane ipsilateral to ostium through which the endoscope is introduced There was limitation of exposure in the coronal plane ipsilateral to ostium through which the endoscope is introduced

62
ESBS 2007 Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region Endoscopic approaches 2 dimensional view 2 dimensional view Depth perception is poor Depth perception is poor Limited manipulability and working area for instruments Limited manipulability and working area for instruments

63
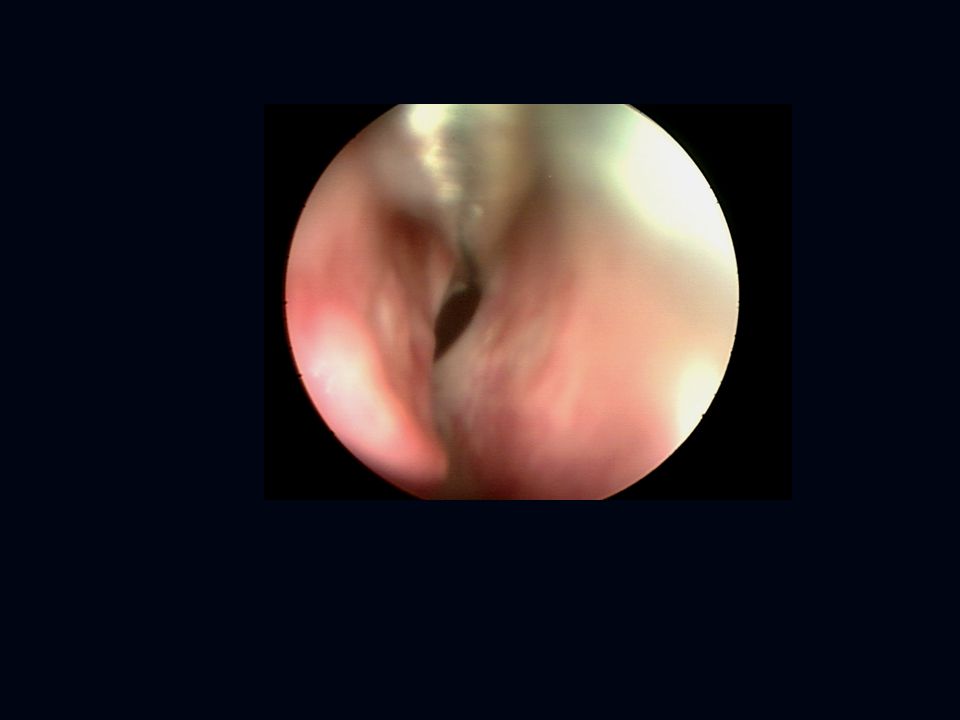
Right Nostril Septum Middle Turbinate

64
ostium

66
Within the sphenoid sinus –through left Nostril Sphenoid septum

68
Diaphragma sella opened exposing the supra sellar structures Floor of the sella Pituitary gland Optic Chiasma

69
Infundibulum Lamina terminalis

70
Optic Chiasma Infundibulum

78
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques-Future Radiographic imaging and image-guided surgery Radiographic imaging and image-guided surgery Three-dimensional imaging and reconstructions for surgical review and planning Three-dimensional imaging and reconstructions for surgical review and planning The knowledge and experience of the surgeon is far more important than any technology or instrumentation The knowledge and experience of the surgeon is far more important than any technology or instrumentation Continued advances in endoscopic equipment, radiographic techniques, and IGS systems will permit to continue to stretch the minimally invasive boundaries in treating skull base pathology. Continued advances in endoscopic equipment, radiographic techniques, and IGS systems will permit to continue to stretch the minimally invasive boundaries in treating skull base pathology.

79
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques-Future Surgical instrumentation Surgical instrumentation Image guidance system Image guidance system Surgical simulators and robotics Surgical simulators and robotics

80
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques-Future Evolution of endoscopic neurosurgery (“endoneurosurgery”) with the description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches (endoscopic skull base instruments, image guidance systems, ultrasonic aspirators), and the innovations of reconstruction techniques Evolution of endoscopic neurosurgery (“endoneurosurgery”) with the description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches (endoscopic skull base instruments, image guidance systems, ultrasonic aspirators), and the innovations of reconstruction techniques
 with the description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches (endoscopic skull base instruments, image guidance systems, ultrasonic aspirators), and the innovations of reconstruction techniques Evolution of endoscopic neurosurgery ( endoneurosurgery ) with the description of unfamiliar endoscopic anatomy, the development of supporting technologies adapted to transnasal endoscopic approaches (endoscopic skull base instruments, image guidance systems, ultrasonic aspirators), and the innovations of reconstruction techniques")
81
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques Choice of approaches? Choice of approaches? Microscope Endoscope combined

82
ESBS 2007 Endoscopic and Minimally Invasive Skull Base Techniques-Future The future of endoscopy in skull base surgery will involve its use both as the primary surgical approach and as an adjunct to the microscope. The future of endoscopy in skull base surgery will involve its use both as the primary surgical approach and as an adjunct to the microscope. New combined endoscopic and microscopic surgical approaches will play an important role in the future of skull base surgery. New combined endoscopic and microscopic surgical approaches will play an important role in the future of skull base surgery.

Similar presentations












 Ass. Professor of Clinical Oncology Kasr El-Aini School of Medicine.>")





, FACS, FCCP Department of Surgery. Division of Cardiothoracic.>")








