Download presentation
Presentation is loading. Please wait.

1
Management of Acoustic Neuroma NEMROCK Experience. 1999-2005 Mohamed Abdulla (M.D.) Ass. Professor of Clinical Oncology Kasr El-Aini School of Medicine Cairo University Tanta Cancer Center Meeting June, 2005
 Ass. Professor of Clinical Oncology Kasr El-Aini School of Medicine Cairo University Tanta Cancer Center Meeting June,")
2
Is a benign or non-cancerous growth that arises from the 8th or vestibulo-cochlear nerve.

3
Growth Pattern:

4
Grade I - Tumor is small, occurring only within the internal auditory canal itself. Grade II - Tumor extends into the fluid spaces around the brainstem Grade III - Larger tumor (usually up to 2.5 cm in diameter). Extends up to the brainstem. Grade IV - Very large tumor (up to 5 cm in diameter). Compresses the brainstem, often involves the nerves of swallowing and the 5th cranial nerve (face and eye sensation)
. Extends up to the brainstem. Grade IV - Very large tumor (up to 5 cm in diameter). Compresses the brainstem, often involves the nerves of swallowing and the 5th cranial nerve (face and eye sensation).")
5
Why Important? 5-10% of all cranial lesions. Sensory Roots > Motor > Autonomic. Vestibular division of 8 th CN followed by Trigeminal. Female predominance. 3 rd – 6 th decade of life.

6
Why Risky? Life Threatening Functional Loss Cosmetic

7
Management Options Observation Surgical Resection SRS

8
Surgical Treatment: Surgical Approaches Sub-Occipital Most Widely Used Hearing Preservation Trans- Labyrinthine Better Exposure Hearing Loss Middle Fossa Intracanalicular + Hearing Preservation

9
Stereotactic RS & RT: Evolution in Computer & Software Technology. Development of High Resolution Imaging Modalities with 3-D Image Reconstruction Facility. The Advent of GK & Linac with Advanced Shaping Techniques. Quality Control Parameters.

10
Delivery of High Dose of IR Limited Volume. Normal Tissue Sparing Necrosis & Tumor Shrinkage

11
Resection or SRS? IssueSurgerySRS No. of Cases3230 Years of Study20011998 No Change in Employment 68%69% +ve Recommendation74%95% Mean Tumor Size25 mm22 mm New Balance Problems 78%7% New Onset Tinnitus57%3% New Facial Nerve Dysfunction 63%10% Martin et al, J Neurosurg 94:211-216,2001.

12
Salvage Surgery After Failure of SRS is not MORE DIFFICULT. No Increase in the Frequency of Having Malignant Transformation as a Late Effect of SRS as Compared to Primary resection. Resection or SRS? Douglas et al, Neurosurg Focus, 14(5), 2003
,")
13
Resection or SRS? Lesion < 30 mm In Extra-Canalicular Radiosurgery Lesion > 30 mm In Extra-Canalicular Surgical Resection Douglas et al, Neurosurg Focus, 14(5), 2003
,")
14
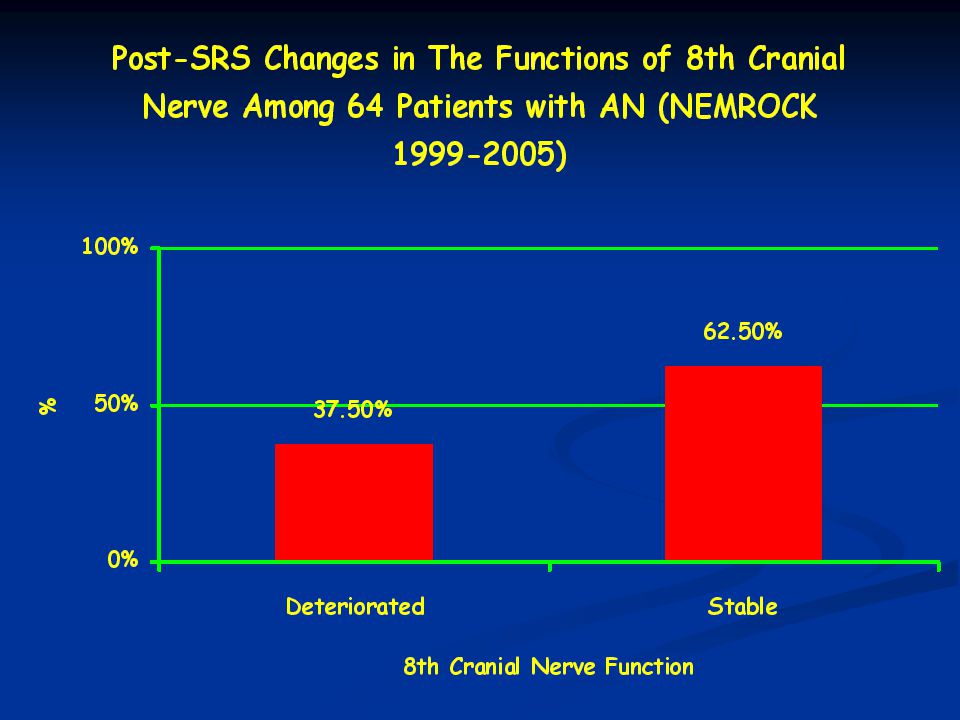
NEMROCK Experience (1999-2005) 64 patients. 29 (M) & 35 (F). 42 ys + 12.3. 54 (Unilateral) 10 (Bilateral) Volume: 8-30 mm Volume: 20 mm + 6.64 Dose Range: 10-20 Gy Follow up: 6-54 months
 10 (Bilateral) Volume: 8-30 mm Volume: 20 mm Dose Range: Gy Follow up: 6-54 months.")
18
SRS in AN: Safe. Upfront Line in Selected Patients. Not Associated with Deterioration of Pre-Treatment Neurological Manifestations. Excellent Response Rate.

Similar presentations








 in Drake et al.>")
(MR)>")




 Ass. Prof. Clinical Oncology Kasr El-Aini School of Medicine Cairo University April,>")


 H. Louis Harkey Department of Neurosurgery University of Mississippi Jackson, MS.>")



