Download presentation
Presentation is loading. Please wait.

1
Frontal Sinus Surgery Babak Saedi
Associate Professor of Department of Otolaryngology Tehran University of Medical Sciences

2
Anatomy Uncinate process Agger Nasi

3
Anatomy Cribriform Plate Lamina papyracea Fovea ethmoidalis

5
Frontal Sinus Mucociliary Flow & Clearance
Frontal recess obstruction is the primary cause of chronic frontal sinusitis , not the sinus. During frontal recess dissection , if these cell walls are removed up to their attachment at the medial orbital wall , & the frontal recess and medial orbital wall mucosa is preserved intact , ciliary mucus clearance will continue uninterrupted . If this mucus membrane is damaged or removed , the sinus may not function properly after healing . Pseudostratified , ciliated columnar epithelium does not regenerate well after being stripped off of bone .

6
Anatomic Variations

7
Uncinate Process Wormald PJ 2008
. In most cases, the uncinate/medialwall of the agger nasi cell implants on the lamina papyracea. he classic description of the insertions of the uncinateIn 1, insertion into the lamina papyracea; 2, insertion into the skull base; 3, insertion into middle turbinate Wormald PJ 2008

9
Anatomy A common reason for ESS failure is inadequate removal of cells obstructing the outflow of the frontal sinus

10
Single Agger Nasi Cell Without Frontal Cells
the uncinate has a relationship only with the posterior half of the agger nasi cell and not with the anterior half, Wormald PJ 2008

11
Single Agger Nasi Cell Without Frontal Cells
line 1 representing a coronal cut through the anterior aspect of the agger nasi cell anterior to the middle turbinate. The diagonally striped, shaded area represents the area of thefrontal sinus above the frontal beak (black arrow). (From Wormald PJ.The agger nasi cell: the key to understanding the anatomy of the frontal recess. Wormald PJ 2008
. (From Wormald PJ.The agger nasi cell: the key to understanding the anatomy of the frontal recess. Wormald PJ")
12
Single Agger Nasi Cell Without Frontal Cells
line 2 representing a more posterior coronal cut through the posterior aspect of the agger nasi cell. This part of the uncinate forms the medial and posterior medial wall of the agger nasi cell and represents the relationship between the anterior agger nasi cell (shaded with dots) and the frontal beak and the floor of the frontal sinus (diagonally shaded area). Wormald PJ 2008
 and the frontal beak and the floor of the frontal sinus (diagonally shaded area). Wormald PJ")
13
Transition From Frontal Sinus To Frontal Recess
The frontal sinus is relatively easy to identify; as it narrows toward the frontal ostia, it forms a square (Fig. 6-16). At this level. the posterior wall of the two frontal sinuses forms a straight line (Fig. 6-16). As the skull base turns poste- riorly,these squares elongate posteriorly but still maintain a roughly rectangular shape. This is the transition stage from frontal sinus to frontal recess (Fig. 6-16D). As the posterior ends of these boxes become pointed, so the scans reach the frontal recess (Fig. 6-16E). Figures 6-16A, B show the square formation of the frontal sinuses. The transition region is between Fig. 6-16D and 6-16E. The anterior wall bone becomes much thicker as the upper region of the frontal beak is reached (Fig. 6-16C). In Figs. 6-16D, E, the anterior wall is curved indicating that the nasion has been reached. In Fig. 6-16D, the nasion is fully developed and the frontal beak bone is thick. Wormald PJ 2008
. At this level. the posterior wall of the two frontal sinuses forms a straight line (Fig. 6-16). As the skull base turns poste- riorly,these squares elongate posteriorly but still maintain a roughly rectangular shape. This is the transition stage from frontal sinus to frontal recess (Fig. 6-16D). As the posterior ends of these boxes become pointed, so the scans reach the frontal recess (Fig. 6-16E). Figures 6-16A, B show the square formation of the frontal sinuses. The transition region is between Fig. 6-16D and 6-16E. The anterior wall bone becomes much thicker as the upper region of the frontal beak is reached (Fig. 6-16C). In Figs. 6-16D, E, the anterior wall is curved indicating that the nasion has been reached. In Fig. 6-16D, the nasion is fully developed and the frontal beak bone is thick. Wormald PJ")
14
Frontal Cells Type I is a single air cell above the agger nasi. Type II is a group of small air cells above the agger nasi, but below the orbital roof. Type III is a single air cell extending from the agger nasi into the frontal sinus. Finally, type IV is an isolated air cell within the frontal sinus not contiguous with the agger nasi. A Agger nasi cell, IS inner sinus septumType I is a single air cell above the agger nasi. Type II is a group of small air cells above the agger nasi, but below the orbital roof. Type III is a single air cell extending from the agger nasi into the frontal sinus. Finally, type IV is an isolated air cell within the frontal sinus not contiguous with the agger nasi. A Agger nasi cell, IS inner sinus septum Kuhn FA 1994

15
Frontal Cells Type I - Single cell above the agger nasi
Type II - Two or more cells above the agger cell Type III - Single cell extending from the agger cell into the frontal sinus Type IV - Isolated cell within the frontal sinus

16
Surgical Indications Chronic sinusitis unresolved with maximal medical therapy; Polyps and allergic fungal sinusitis Intracranial complications of sinusitis Mucoceles or mucopyoceles Benign neoplasms such as osteomas, inverting papillomas, or fibrous dysplasia.

19
Finding The Frontal Recess

20
Finding The Frontal Recess

21
Endoscopic Frontal Sinusotomy
Understand the patient’s frontal recess anatomy Ascertain the anatomical reason for frontal recess/frontal sinus obstruction Determine the best surgical approach to the problem The combination of delicate endoscopic techniques, new frontal sinus instruments designed to allow the surgeon to work further up in the frontalsinus, and image-guided surgery, has extended the surgeon’s ability and reduced the need to use some of the other techniques Many patients who might have required the combined above and below (endoscopic and trephine) approach 10 years ago now can be managed endoscopically
 approach 10 years ago now can be managed endoscopically.")
22
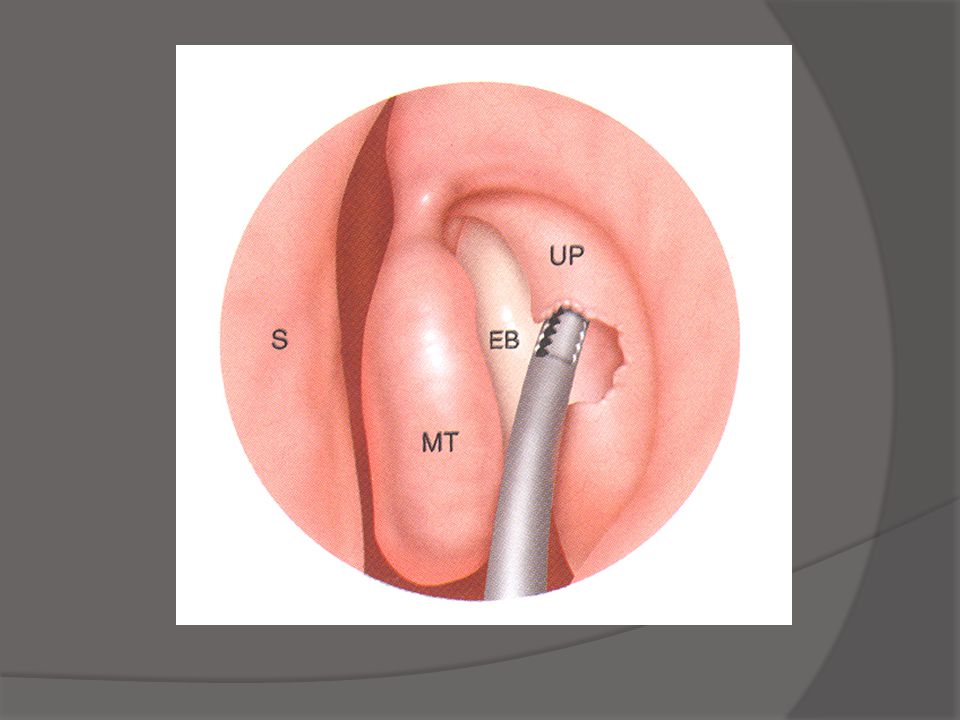
Endoscopic Frontal Sinusotomy Principles
Dissection should be performed from posterior to anterior and from medial to lateral Preserve all frontal recess mucus membrane The frontal ostium can be stented or left alone!!!! /The posterior frontal recess table is commonly very thin and subject to penetration with subsequent cerebrospinal fluid (CSF) leak. The same pertains to the medial posterior frontal recess, bounded by the lateral cribriform plate lamella / sinus mucus membrane does not regenerate over bare bone with normal cilia / frontal sinus not only drains over the medial and posterior walls, but that it can be approached the same way from below (ie, posterior and medial). Consequently, once the ethmoid dissection is complete, the frontal recess cells can be removed with frontal sinus punches (Karl Storz) (Fig. 5) or fractured from posterior to anterior and from medial to lateral with frontal recess curettes / depending on how widely open it is and how well the mucosa drapes over the edge of the frontal ostium. Soft flexible silastic stents rather than semirigid stents should be used / semirigid stents induced circumferential scaring and osteoneogenesis at the frontal ostium in their dog frontal sinus experiments. Soft 0.01 inch thick silastic sheeting cut and rolled into a T shape makes an excellent frontal sinus stent . Kuhn FA 2006
 leak. The same pertains to the medial posterior frontal recess, bounded by the lateral cribriform plate lamella. / sinus mucus membrane does not regenerate over bare bone with normal cilia. / frontal sinus not only drains over the medial and posterior walls, but that it can be approached the same way from below (ie, posterior and medial). Consequently, once the ethmoid dissection is complete, the frontal recess cells can be removed with frontal sinus punches (Karl Storz) (Fig. 5) or fractured from posterior to anterior and from medial to lateral with frontal recess curettes. / depending on how widely open it is and how well the mucosa drapes over the edge of the frontal ostium. Soft flexible silastic stents rather than semirigid stents should be used. / semirigid stents induced circumferential scaring and osteoneogenesis at the frontal ostium in their dog frontal sinus experiments. Soft 0.01 inch thick silastic sheeting cut and rolled into a T shape makes an excellent frontal sinus stent. . Kuhn FA")
24
http://www. dr. babaksaedi. com/DesktopDefault. aspx

26
Draf Procedures

27
Draf I Anterior ethmoid cells Uncinate process
Obstructing frontal cells

28
Draf II Floor of the frontal sinus Lamina papyracea to Septum
Anterior face of Frontal

29
Draf III Modified Lothrop Interfrontal septum Nasal septum
Frontal sinus floor

30
Surgical Outcomes Following the Endoscopic Modified Lothrop Procedure
Conclusion: EMLP is a safe and effective surgical alternative to OPF for patients with recalcitrant frontal sinus disease. Major complications are rare. A large percentage of patients may require revision surgery Laryngoscope, 117:765–769, 2007

31
Frontal Sinus Trephination
Finding the frontal recess Mucoceles Isolated Type IV frontal cells With endoscopic techniques to assist with Draf II and III

32
Combined Approaches

33
Endoscopic Frontal Sinoplasty
The least invasive procedure It can be used as a stand-alone procedure or with ethmoidectomy It pushes the medial agger nasi cell wall laterally and the ethmoid bulla lamella posteriorly K / simple and straight-forward method of identifying the frontal sinus drainage pathway and identifying the air cell walls compromising it, which need to be removed. / When used as a stand-alone procedure, it provides a straight-forward means of cannulating the frontal sinus and dilating the drainage pathway without damaging the mucociliary clearance mechanism / When performed with endoscopic ethmoidectomy, it is counterin- tuitive to leave any cell walls around the frontal ostium / When viewed endoscopically several months postopera- tively, even though the remaining cell walls around the frontal ostium still seem as though they should have been removed. The frontal ostium looks healthy and is functiona / under fluoro scopic control by endoscopically placing a 70 or 90 guiding cannula into the upper middle meatus and passing the guide wire through it up into the frontal sinus /Once the wire is in the sinus, a balloon catheter is passed over it into the frontal sinus, its position checked fluoroscopically, and the ballloon is inflated to dilate it fully / Kuhn FA 2006

34
Modified Lothrop

35
Frontal Recess & Frontal Beak
This drawing illustrates the effect of a small. under- pneumatized agger nasi cell (AN). The frontal beak (FB) is large and the AP diameter of the frontal ostium (FO) small. The frontal recess (FR) is shaded and extends from the beak to the bulla lamella (BE).(B) This drawing illustrates the effect of a well-pneumatized agger nasi cell (AN) with a small frontal beak (FB) and large frontal ostium (FO). if the bulla lamella (BE) does not reach the skull base. a suprabullar recess (5BR) is formed. MT. middle turbinate. Wormald PJ 2008
. The frontal beak (FB) is large and the AP diameter of the frontal ostium (FO) small. The frontal recess (FR) is shaded and extends from the beak to the bulla lamella (BE).(B) This drawing illustrates the effect of a well-pneumatized agger nasi cell (AN) with a small frontal beak (FB) and large frontal ostium (FO). if the bulla lamella (BE) does not reach the skull base. a suprabullar recess (5BR) is formed. MT. middle turbinate. Wormald PJ")
36
Osteoplastic Flap Vs. Draf III
Narrow Nasal Airway Small Frontal Sinus Deep Nasion Floor of sinus < 1.5 cm Heavy thick nasofrontal beak Proliferative osteitis, complicated chronic infection Favor Draf III for mucoceles

37
Osteoplastic Flap Vs. Draf III

38
The frontal osteoplastic flap: does it still have a place in rhinological surgery
The frontal osteoplastic flap still has a role in frontal sinus surgery. The Journal of Laryngology & Otology (2011), 125, 162–168.
, 125, 162–168.")
39
Osteoplastic Flap May be modified to fit the patient

40
Osteoplastic Flap Approach
Osteoplastic and endoscopic (above and below approach) Frontal sinus obliteration / Above and below is the procedure of choice for frontal sinus tumors, such as inverting papilloma, so that the sinus may be imaged postoperatively. It is also the procedure of choice for unobliteration, because it gives the best opportunity to completely remove whatever material was used to obliterate the sinus originally and to open the frontal recess. It also provides access to the farthest extent of the sinus to reconnect distant isolated pockets of mucus membrane to the frontal recess /Contraindications to frontal sinus obliteration are: missing posterior frontal sinus table bone, missing orbital roof bone, extensive supraorbital ethmoid cell pneumatization, frontal sinus tumor, and allergic fungal sinus / FSO is now mostly reserved for only cases involving tumors in the frontal sinus region, extremely difficult revision cases, and cases of frontal sinus trauma. / One cannot be certain the mucus membrane is removed completely while preparing the frontal sinus for obliteration, even by drilling the bone / One definitely cannot be certain of removing the mucus membrane from the dura or the periorbita, in each case, frontal sinus mucosa is adherent to soft tissue, either to the dura or to the periorbita / As a rule, if there is any question about whether all of the frontal sinus mucus membrane can be removed, obliteration should not be performed. / The primary symptom of frontal obliteration failure is persistent, unremitting hard frontal pain. When all conservative methods have failed to account for or to control the pain, it is often necessary to re-explore the sinus. / When unobliterating a frontal sinus, the primary task is to reconnect the peripheral mucosalized areas to a functional frontal ostium. The second major task is recreating a functional connection to the nose or anterior ethmoid sinus / There are clearly instances in which the Lothrop procedure, which is very straightforward when the frontal sinus is open, is the best solution to ensuring a patent ostium. In other instances, the endoscopic frontal sinusotomy is best / Wynn R, et al 2007
 Frontal sinus obliteration. / Above and below is the procedure of choice for frontal sinus tumors, such as inverting papilloma, so that the sinus may be imaged postoperatively. It is also the procedure of choice for unobliteration, because it gives the best opportunity to completely remove whatever material was used to obliterate the sinus originally and to open the frontal recess. It also provides access to the farthest extent of the sinus to reconnect distant isolated pockets of mucus membrane to the frontal recess. /Contraindications to frontal sinus obliteration are: missing posterior frontal sinus table bone, missing orbital roof bone, extensive supraorbital ethmoid cell pneumatization, frontal sinus tumor, and allergic fungal sinus. / FSO is now mostly reserved for only cases involving tumors in the frontal sinus region, extremely difficult revision cases, and cases of frontal sinus trauma. / One cannot be certain the mucus membrane is removed completely while preparing the frontal sinus for obliteration, even by drilling the bone. / One definitely cannot be certain of removing the mucus membrane from the dura or the periorbita, in each case, frontal sinus mucosa is adherent to soft tissue, either to the dura or to the periorbita. / As a rule, if there is any question about whether all of the frontal sinus mucus membrane can be removed, obliteration should not be performed. / The primary symptom of frontal obliteration failure is persistent, unremitting hard frontal pain. When all conservative methods have failed to account for or to control the pain, it is often necessary to re-explore the sinus. / When unobliterating a frontal sinus, the primary task is to reconnect the peripheral mucosalized areas to a functional frontal ostium. The second major task is recreating a functional connection to the nose or anterior ethmoid sinus. / There are clearly instances in which the Lothrop procedure, which is very straightforward when the frontal sinus is open, is the best solution to ensuring a patent ostium. In other instances, the endoscopic frontal sinusotomy is best. / Wynn R, et al")
41
Riedel's Procedure Osteomyelitis of the anterior wall of the frontal sinus Failure of frontal sinus obliteration Some tumors of the frontal sinus Riedel's procedure can help eradicate frontal sinus disease and symptoms when drainage and obliteration have failed and there is persistent disease involving the anterior wall of the frontal sinus or the sinus itself. A extradural Riedel's procedure preferable in dealing with chronic infection or locally invasive disease. . Riedel's procedure maintains a barrier in the form of the posterior wall of the frontal sinus and the intracranial contents. Postoperative disfigurement, the main criticism of this procedure, can be reduced to some extent by chamfering the margins of the frontal sinus along with the supraorbital rims (Figs to 53-21).[27] Reconstruction of the anterior wall can be performed at a later date if necessary. Because the frontal sinus mucosa is completely removed, the chance of recurrent complications are few, and if recurrence happens, it can easily be recognized.
.[27] Reconstruction of the anterior wall can be performed at a later date if necessary. Because the frontal sinus mucosa is completely removed, the chance of recurrent complications are few, and if recurrence happens, it can easily be recognized.")
42
Pearl #1 Carefully Examine the Anatomy in more than one CT plane
Size of the frontal recess Size of the frontal sinus Bony thickening or neo-osteogenesis Identify the frontal sinus drainage pathway Note the position of the anterior ethmoidal artery

43
Pearl # 2 Identify the Anterior Ethmoidal Artery
Superior extension of anterior wall of bulla Nipple on the medial orbital wall 1-4 mm’s below skull base Typically posterior to supraorbital ethmoid cells

44
Pearl #3: Plan the least invasive approach possible
Ethmoidectomy with Middle Meatal Antrostomy without frontal recess surgery Frontal recess surgery Endoscopic frontal sinusotomy Frontal sinus trephination Unilateral extend frontal sinus surgery (Draf II) Endoscopic Modified Lothrop (Draf III) Osteoplastic flap with or without obliteration
 Endoscopic Modified Lothrop (Draf III) Osteoplastic flap with or without obliteration.")
45
Pearl #4 Positively Identify the Skull Base Posteriorly
Skeletonize from posterior to anterior Open cells immediately posterior to the middle turbinate Identify the sinus with a seeker

46
Pearl #5 Positively identify the frontal sinus with a probe
Need a relatively dry field 45 degree telescopes are helpful Identify medial orbital wall and stay close to it dissecting superiorly Opening to frontal sinus typically medial Identify opening with a probe

47
Pearl # 6 Preserve the Mucosa
Consider leaving polyps if sinus is open Remove osteitic intersinus septae carefully Do not traumatize unless sinus can be opened widely Standard frontal sinusotomy Draf Type II Works well if you can: Preserve mucosa Remove bony partitions Create an ostium >4-5 mm

48
Pearl #7 Keep the Sinus Open Postoperatively
Remove fibrin and blood from frontal recess and frontal sinus Remove residual bone Antibiotics, topical steroids? Oral Steroids?

49
Conclusion Very little evidence based medicine
Do the least invasive procedures first Be aware of various surgical options Image guidance a valuable tool First do no harm

Similar presentations






















 Root Ala Dorsum>")
