Download presentation
Presentation is loading. Please wait.

2
Anthony Worsham, MD Friday, June 18, 2010 Hospital Medicine Best Practices Meeting University of New Mexico

3
Case vignette Background Pathophysiology Guidelines Action recommendations Discussion with Dr. Garcia

4
44-year-old man HPI: ESRD secondary to DMII, CAD CC: sepsis/osteomyelitis Hospital course: osteomyelitis treated with piperacillin/tazobactam right subclavian catheter-associated DVT treated with heparin drip Orthopedics consulted; BKA scheduled was switched to argatroban due to platelet drop morning prior to surgery, patient went into PEA arrest and ACLS protocol initiated, but patient died.

6
73-year-old female transferred for workup of a possible left adnexal mass multiple abdominal surgeries at St. Vincent's secondary to necrotizing fasciitis as well as multiple abdominal abscesses several decubitus ulcers with wound VAC pulmonary embolism at outside hospital on a heparin drip MDR UTI with Klebsiella, Pseudomonas, Candida and VRE malnutrition

9
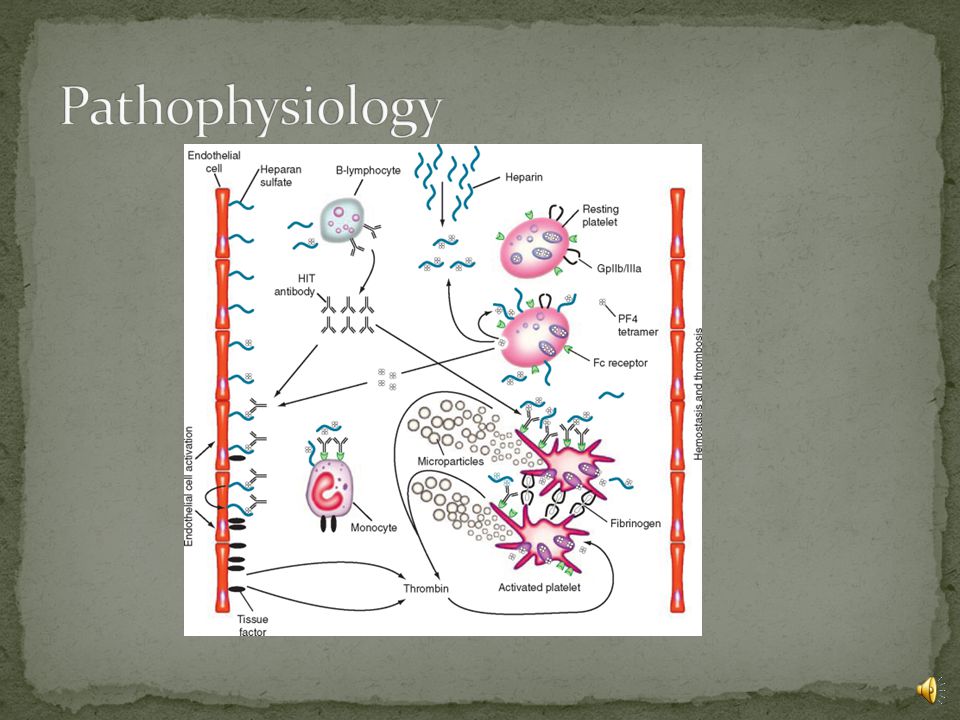
formerly known as HIT Type II thrombocytopenia absolute: <150,000/mL 3 relative: 50 percent or more fall from baseline surgical patients: baseline platelet count is post-surgical peak, not admission Timing: classically incidence 1% to 5% of postoperative patients 0.5% to 1% of medical patients duration of heparin >1 wk v LMWH>fondaparinux) (OR~10-15), type of patient (surgery>medical>pregnancy) OR ~3-4, higher risk in women (odds ratio, 1.5– 2.0) Timing: 5-10 days post heparin exposure Mechanism Platelet activation by binding of heparin-dependent IgG to platelet FcγIIa receptors
 (OR~10-15), type of patient (surgery>medical>pregnancy) OR ~3-4, higher risk in women (odds ratio, 1.5– 2.0) Timing: 5-10 days post heparin exposure Mechanism Platelet activation by binding of heparin-dependent IgG to platelet FcγIIa receptors")
13
Venous thromboembolism DVT (50%) and pulmonary embolism (25%) Arterial thrombosis Limb artery thrombosis (10%–15), thrombotic stroke (5%–10%), myocardial infarction (3%–5%), other (eg, mesenteric artery thrombosis, spinal artery thrombosis) Thrombotic stroke Coumarin necrosis Adrenal hemorrhage Necrotizing skin lesions at heparin injection sites Anaphylactoid reaction DIC 10%–20% of patients who have HIT have overt (decompensated) DIC (eg, hypofibrinogenemia, increased INR, positive protamine sulfate paracoagulation Warkentin TE, Heparin-induced thrombocytopenia, Hematol Oncol Clin N Am 21 (2007) 589–607
 and pulmonary embolism (25%) Arterial thrombosis Limb artery thrombosis (10%–15), thrombotic stroke (5%–10%), myocardial infarction (3%–5%), other (eg, mesenteric artery thrombosis, spinal artery thrombosis) Thrombotic stroke Coumarin necrosis Adrenal hemorrhage Necrotizing skin lesions at heparin injection sites Anaphylactoid reaction DIC 10%–20% of patients who have HIT have overt (decompensated) DIC (eg, hypofibrinogenemia, increased INR, positive protamine sulfate paracoagulation Warkentin TE, Heparin-induced thrombocytopenia, Hematol Oncol Clin N Am 21 (2007) 589–607")
14
Differential diagnosis Sepsis DIC TTP/HUS Drug-induced Antibiotics Heparin (see OSU website) ITP
 ITP")
15
2 points1 point0 points Thrombocytopenia>50% fall or nadir 20-100 x 10 9 /L 30-50% fall or nadir 10-19 x 10 9 /L <30% fall or nadir <10 x 10 9 /L Timing of platelet count fall Days 5-10 or <1 day if heparin exposure within past 30 days >Day 10 or unclear (but fits with HIT) or <1 day if heparin exposure within past 30-100 days <1 day (no recent heparin) Thrombosis or other sequelae Proven thrombosis, skin necrosis, or, after heparin bolus, acute systemic reaction Progressive, recurrent, or silent thrombosis; erythematous skin lesions None OTher cause for thrombocytopenia None evidentPossibleDefinite pretest probability of HIT by total points is as follows: 6 to 8=high (60-80%), 4 to 5=intermediate (10-30%); 0 to 3=low (<5%) Lo GK, et al. Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin- induced thrombocytopenia in two clinical settings. J Thromb Haemost 2006; 4: 759–65.
 for the diagnosis of heparin- induced thrombocytopenia in two clinical settings. J Thromb Haemost 2006; 4: 759–65..")
16
ISTH DIC score ≥ 5 sufficient to diagnose or rule out DIC. (91% sensitivity, 97% specificity, 96% positive, predictive value, 97% negative predictive value)
.")
17
functional assay: serotonin release assay (SRA) gold standard technically demanding, requires radiation Send out lab sensitive and specific (>95%) antigen immunoassays enzyme-linked immunosorbent assay [ELISA] high sensitivity, low specificity PIFA ® (Particle ImmunoFiltration Assay) Platelet aggregation assay HIPA (heparin-induced platelet aggregation) Results not immediately available for any test
![functional assay: serotonin release assay (SRA) gold standard technically demanding, requires radiation Send out lab sensitive and specific (>95%) antigen immunoassays enzyme-linked immunosorbent assay [ELISA] high sensitivity, low specificity PIFA ® (Particle ImmunoFiltration Assay) Platelet aggregation assay HIPA (heparin-induced platelet aggregation) Results not immediately available for any test](http://images.slideplayer.com/10/2768478/slides/slide_17.jpg "functional assay: serotonin release assay (SRA) gold standard technically demanding, requires radiation Send out lab sensitive and specific (>95%) antigen immunoassays enzyme-linked immunosorbent assay [ELISA] high sensitivity, low specificity PIFA ® (Particle ImmunoFiltration Assay) Platelet aggregation assay HIPA (heparin-induced platelet aggregation) Results not immediately available for any test")
18
Warkentin TE, et al. Am J Med. 1996;101:502-507.

19
Initial treatment decisions made on clinical grounds Confirm thrombocytopenia (repeat CBC) Test for DIC Test for HIT antibodies Assess for thromboses (eg, ultrasound for lower-limb DVT) Stop all heparin (including heparin “flushes” and, possibly, use of heparin-coated intravascular catheters [catheters in situ for several days may not have significant residual heparin) Initiate alternative anticoagulation (options: argatroban, lepirudin, bivalirudin, fondaparinux [?]) if HIT is strongly suspected
![Initial treatment decisions made on clinical grounds Confirm thrombocytopenia (repeat CBC) Test for DIC Test for HIT antibodies Assess for thromboses (eg, ultrasound for lower-limb DVT) Stop all heparin (including heparin flushes and, possibly, use of heparin-coated intravascular catheters [catheters in situ for several days may not have significant residual heparin) Initiate alternative anticoagulation (options: argatroban, lepirudin, bivalirudin, fondaparinux [ ]) if HIT is strongly suspected](http://images.slideplayer.com/10/2768478/slides/slide_19.jpg "Initial treatment decisions made on clinical grounds Confirm thrombocytopenia (repeat CBC) Test for DIC Test for HIT antibodies Assess for thromboses (eg, ultrasound for lower-limb DVT) Stop all heparin (including heparin flushes and, possibly, use of heparin-coated intravascular catheters [catheters in situ for several days may not have significant residual heparin) Initiate alternative anticoagulation (options: argatroban, lepirudin, bivalirudin, fondaparinux [ ]) if HIT is strongly suspected")
20
Di Nisio M, et al. Direct thrombin inhibitors. NEJM 2005;353:1028-40.

21
Exosite 1 = dock for substrates such as fibrin Exosite 2 = heparin binding domain

22
argatroban hepatically cleared lepirudin renally cleared ?higher risk of bleeds bivalirudin Mostly used during cardiac surgery Di Nisio M, et al. Direct thrombin inhibitors. NEJM 2005;353:1028-40. argatroban: thrombosis decreased to 13-19% vs 35% historical controls; bleeding rate 6-11% lepirudin: thrombosis decreased to 4% vs 15% historical controls; bleeding rate 14% bivalirudin: mostly used during PCI or cardiothoracic surgery

23
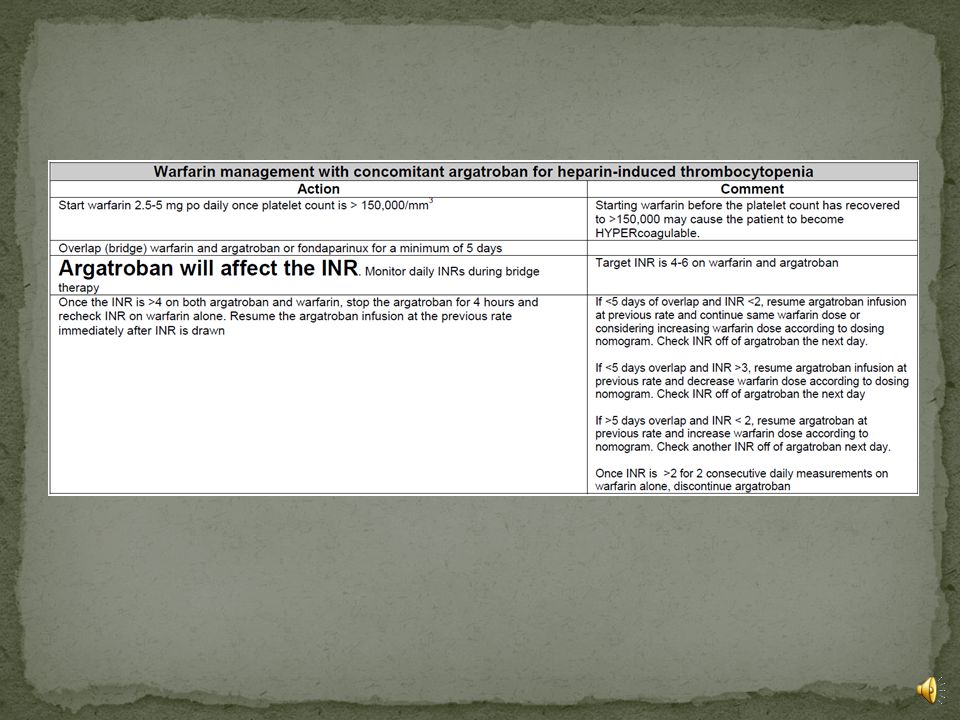
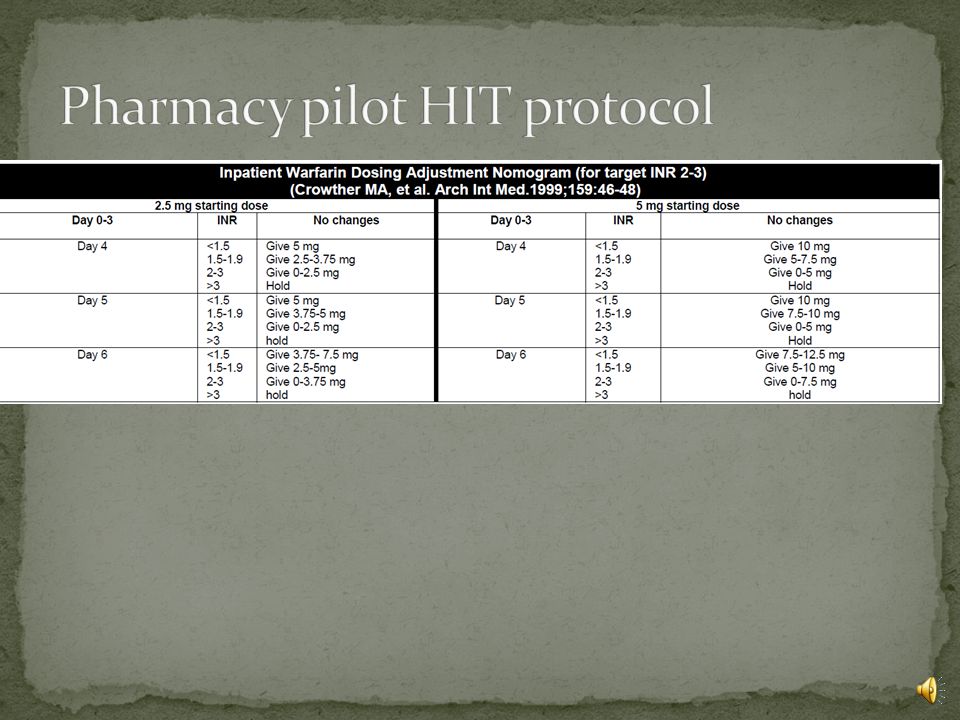
postpone warfarin until platelet count > 150 × 10 9 /L warfarin and DTI should overlap 4-5-days target INR for concomitant warfarin/argatroban 4.0 Warkentin T et al,Treatment and Prevention of Heparin-Induced Thrombocytopenia: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest June 2008 133:340S-380S
 Chest June :340S-380S")
30
When should hematology consult be obtained? Would placing a HIT protocol in CPOE be helpful?

Similar presentations














,as adjuvant therapy following resection of AJCC stage IIB.>")










 IPC/GCS or, UFH 5000 SQ q 12 hrs or, Enoxaparin 40mg SQ daily IPC/GCS or, UFH 5000.>")

